I guess I'll give some background, as a long article dissecting digdeeper would appear unwarranted and cold without one, like some kind of sucker-punch.
I used to follow digdeeper's website. I followed it for a couple years. At first, it was largely for advice relating to nanonymity (privacy+security+anonymity), which I had been taking more and more seriously as time went on. At the same time, my thinking also became more conspiratorial. I don't blame digdeeper's website for this. However, I did turn towards his other articles on society as I became more conspiratorially-minded.
A little after my conspiratorial thinking had reached its peak, and declined somewhat (from being borderline insane, to merely being mostly out of touch with reality), I joined digdeeper's MUC, and found community there. I was there for a couple years.
As time passed, I became less conspiratorial in my thinking. I won't explain how this happened exactly (CIA abducted me and brainwashed me with MK ULTRA techniques). It lead me to question all of my beliefs, and re-evaluate how I come to determine the veracity of my beliefs in the first place. This was a two or so year process. It began slow, and accelerated as time went on.
By the end of the process, I left digdeeper's community.
I like writing, and I write often, which lead me to eventually write about digdeeper's site. I don't share much of what I write, but I figured I would share this, because it could be useful. I wrote most of what I will be sharing over a fairly long period of time, incrementally.
This is part of a greater analysis. I never got quite done with that analysis, in terms of ironing it out to make it readable to others. I've been thinking of putting some parts of it up for a few months now. I figured that for the time being, I'll start with this, since it's the most complete of anything I've written regarding his site. Putting out a massive article going over the entire website is probably a bit much to start off with.
Well, in hindsight, that didn't work out. This ended up being a massive article. Still though, it doesn't cover his whole site. I don't think I'll end up wasting my time on that, as it would be insane. My writing was driven by my deconstruction of my previous beliefs. Now that I've shed them, I see little point in going to such lengths. If digdeeper had profound, unique insights to offer, I would go deeper in my analysis of his politics, but his political analysis is shallow, in my view.
I would rather not share my other writing here, and taint it by attaching it to an analysis of some dumb website, so, this website will probably not have much activity. I guess I could share my analyses of other dumb websites e.g Luke Smith's site, or websites from other dumb religious fundamentalists.
I think for the most part such analyses are not stimulating or valuable, as the authors behind such sites have ideas that are not well-thought out, and put little effort into their articles sharing their ideas. Critiquing them is like bare-knuckle boxing with middle-schoolers as a grown adult. Your mind will atrophy if those sorts of people are all you focus on.
It's been a long time since I've visited digdeeper's website, but when I think of it, it makes me sad.
I feel that digdeeper has spent a great deal of time and effort creating a website with an incoherent message, which the vast majority of people will never find compelling. As a result, digdeeper will live in frustration due to his inability to produce his desired change in the world.
Of course very few, if not any, neocities websites will produce meaningful political change in the world. But this isn't entirely what I mean to say. Among other things, like the veracity of one's message, and how compelling one's message is, some of the determining factors in the appeal of one's message is its relevance in addressing the people's material concerns. This largely influences how compelling and truthful messaging is perceived to be.
If the message someone carries is compelling and truthful, they will probably find others they don't even know who carry the same message, and promote it. This can contribute to a shifting tide, toward changes in the world that one would like to see. Digdeeper doesn't have this and probably never will, because of his incoherent beliefs. As he is, he is constrained to a community of contrarians with middling levels of insight into politics. They compensate for this middling insight with conspiratorial thinking.
Digdeeper's website is for the most part the same as it was when I left, beyond design changes, and minute updates to articles which do not meaningfully alter their conclusions.
His heavy focus on conspiracism leads him astray. He spends too much time on divisive, often-fringe rhetoric, like debunked conspiracies, and the supposed censorship of grifters, pseudoscientists, and snake oil salesmen, as opposed to focusing on issues with greater significance, which tend to carry wider appeal as a result.
His focus on conspiracism ultimately undermines his efforts to combat capitalism, as the logical conclusion of many conspiracy theories, when society acts upon the knowledge that they purvey, is typically destructive for the masses and beneficial to the capitalist class e.g vaccine hesitancy (harm to health, profit to health insurance companies, lowered quality of life for populace makes them more exploitable), rejection of public education (lowered critical thinking skills at population level, population more manipulable), climate change denial (average citizen's quality of life lowered across virtually all metrics, to the benefit of the most wealthy).
Often times as these conspiracies grow in popularity and recognition by elements of the establishment, they become more exploitative, assuming that the conspiracy/conspiracies were not exploitative to begin with. For instance, look at how RFK Jr. and his goons have rode the anti-vaccine wave in America. Using the widespread skepticism of medical institutions, and of vaccines, they've managed to legalize the usage of carcinogenic pesticides, in order to increase profits for corporations, while promoting laughable solutions to chronic diseases like beef tallow in fries. People like digdeeper allowed this to happen.
Digdeeper's paranoia deprives him of a substantive path towards revolution. Any possible outlet has already been written off subconsciously. He has nothing but people as deluded as himself to chat with online. They are so far and few that you could hardly hope to encounter one of them in the wild.
There are many conmen and idiots that digdeeper regards as trustworthy sources of information.
Miles Mathis and Winston Wu are decent examples, though other fools like Ray Peat exist.
Miles Mathis has profoundly-idiotic, objectively-wrong mathematical conjectures. He thinks that pi = 4. He thinks the derivatives used in calculus for elemental functions are wrong. Mathematics is one of the two fields — philosophy being the other — where things can be objectively true or false. Mathematical knowledge can translate into reality, as it often comes through the observation and study of reality. Mathematicians far more intelligent than Mathis (who is not a mathematician) have proven the veracity of these things.
Furthermore people have created technology using their knowledge of calculus and basic geometry. If they were wrong, their technology literally could not function. So, Mathis is just dead wrong when it comes to these topics as they translate into applied mathematics.
Mathis doesn't believe in anything. Everything is fake to him. It stems from his personal incredulity and delusions of grandeur. His argument about Stephen Hawking being fake literally boils down to the fact that it's very unlikely for Hawking to have lived for as long as he did. This is not proof of anything but that. He could have simply lived way longer than expected. It happens with some ALS patients. It's rare, but it happens. Also, given how important he was to physics, I wouldn't be surprised if he got better care than most. And he's dead now isn't he? He died of ALS years ago.
According to Mathis, the Boston Marathon bombing, Sandy Hook, the Zodiac killings, the Lincoln assassination, Waco, Iwo Jima, the Titanic, Custer's Last Stand, and all sorts of other significant historical events were faked. Basically all historical leaders for the last couple hundred years are Jewish conspirators. I don't want to get into a super long polemic against Mathis, but his theories can be disproven. They stem from his lack of knowledge about how history is studied, seeing meaningful patterns where there aren't any, presumptions based in ignorance (in the sense that he'll think he's found a discrepancy somewhere when he really just doesn't know how that thing works or the context of the supposed discrepancy), and from sheer incredulity.
He uses unverifiable sources to prove conspiracies, like by saying people involved in an event like Waco are still alive. What is someone going to do? Locate a supposed crisis actor and interview them? Nobody who believes Miles Mathis will put in the work to do that, and nobody else will care enough to bother, because they already know that Mathis is insane.
I don't know what kind of mental disorder he has, but it's likely lead him to thinking the way he does. He's convinced that there's a grand conspiracy to silence him. He literally thinks people like Edward Snowden were dispatched to distract the masses from him. The conspiracies he believes in would have so many moving parts, countless people involved in them, and have gone on for so long. Surely there would be solid, irrefutable evidence to back them up? Yet there isn't.
I take issue with holding a person who is clearly a maniac with many false theories, so many that they should be discounted as a serious person, in regard, as some enlightened pariah.
Winston Wu is a conspiracy theorist with an awful article supposedly proving the Moon landings to have been faked, with arguments that consist almost exclusively of him misinterpreting mundane information as evidence of a conspiracy, as well as arguments based in his nonexistent understanding of physics, like not understanding how heat would transfer in a near-vacuum, or not understanding conservation of momentum, or how light works to form shadows; other times he misrepresented information like quotes to make people and articles say things that they never said. I don't believe that he intentionally did these things, I think that he just plagiarized most of his argumentation from others. He has the naivete of a child, it shows in the sections where he cites Bart Sibrel.
He also believes in nonsense like parapsychology, which is basically the "study" of ESP, telekinesis, and other psychic abilities. He believes in "miracles", aliens, and ghosts as well. His article "Debunking PseudoSkeptical Arguments of Paranormal Debunkers" outlines his belief in all of these things. In this same article, he reveals that he is "skeptical" of evolution, and promoted the laughable "documentary" 'Expelled: No Intelligence Allowed'. The article consists mostly of him blindly accepting nonsense put out by grifters, conmen, pseudoscientists, and crazy people.
Upon the discovery that Winston Wu is, by his own admission, schizophrenic, his behavior makes sense.[1]
It's sad.
I'm sure that digdeeper doesn't agree with much of what Mathis says, and perhaps not all of what Wu says, which brings the problem of why digdeeper considers anything that they say.
Digdeeper likely needs to maintain very low standards for himself in order to provide himself with enough people to interact with so as to not go insane.
It can be seen with the free speech mantra for digdeeper's XMPP server. Although the server is no longer truly free speech, ideas remain uncensored. Digdeeper doesn't go about suppressing any ideas, he is open to chatting with anybody.He falsely assumes that everyone's ideas are worth dignifying.
Some people's ideas aren't worth dignifying. Some people, to me at least, aren't worth chatting to. Not anymore. Nazis for example. I used to have no standards, and so I'd befriend Nazis online. I could agree to disagree with certain beliefs of theirs. I mean, I used to not even disagree with some of their beliefs, but now I do. And I won't just agree to disagree. Nazis are idiots with no comprehension of history, who can do nothing but try and gish gallop their way through a debate, and fail. They're idiots. And they're dangerous idiots. Their ideology resulted in the deaths of tens of millions of people in the last century. Now we can see fascistic ideologies manifesting in America, and the logical conclusions of them playing out in Israel. People should not dignify monstrosities, nor should they the worshippers of monstrosities.
It's the same with flat earthers. While not as dangerous as Nazis, they're still complete imbeciles who don't believe in something that _ancient people_ were able to figure out. These are extremely stupid people. They choose to not believe that the earth is a globe. When you provide them with evidence, they use rhetorical tricks, like a vast, omnipresent, omnipotent conspiracy to hide the truth, in order to discount your evidence. When you refute their evidence in a way where they can't use this pathetic trick of theirs, they stick their heads in the sand. When they have no other options, they lie.
For example, I told a member of digdeeper's MUC that 'The Final Experiment' was livestreamed. He lied and said that it wasn't. When I posted a livestream, he said it must've been pre-recorded, even though there was real-time interaction which is impossible to fake unless they had bots, or conspirators writing comments. Another time, while arguing with this same flat earther, he asserted that the Moon was a hologram, after I used the Moon to prove that the earth is round. Ultimately, what else could he do to maintain his belief? Nothing. If all else fails, assert the Moon itself to be the product of a conspiracy.
Pretending that these sorts of people have anything valuable to offer is so very detrimental to one's personal enrichment, in terms of how one's interactions with others help them better understand the world.
After leaving digdeeper's community, I realized that the only value these sorts of people provided me with was in agreeing with me on conspiracies. They provided me validation. That's what it was. Digdeeper's server is a cesspit of anti-intellectual buffoons who can hardly cope with reality by themselves, and who affirm one another's delusions, while arguing against some of each other's delusions, but only in favor of promoting their own delusions. I would simply overlook their glaring idiocy as an eccentricity, a quirk, a minor personal flaw. It is far more than that. It is what it is: idiocy. It's not eccentricity or some minor flaw in their personality. These people have very little to otherwise offer, unfortunately.
It is sad. It is a waste of human potential. If they chose to not be willfully-ignorant, they could learn some things, and maybe have happier lives.
Since I left the community, there were a handful of times I joined the MUC under a pseudonym. It was less than five times. The anecdotes I gave with the flat earther came from two of them.
I returned as an anonymous person so that I could see things from an outside perspective. I wanted to see if the people I spent so long chatting with were really just closed-minded idiots living in an echo-chamber. As it turned out, they were. Immediately, if I so much as gave any dissension, people would ask me why I even joined the MUC, why am I promoting the status-quo; they'd accuse me of shilling. Digdeeper did this himself. It was just like it was when I had first joined the server.
The very first time I had joined the digdeeper MUC, I'd stumbled upon a vaccine discussion. At the time, I had opposed the COVID vaccines, but not all vaccines (I never have). Just about everyone talking opposed vaccines categorically. And they were displeased to have me giving pushback. Immediately, they questioned my intentions for dissenting. Why am I promoting the status quo? Why am I shilling? Again, digdeeper himself did this.
No nuance, no intellectual rigor or curiosity. It was pure rhetoric and nothing more.
Unfortunately, I learned when to be silent, and when to talk, and wasted quite some time in that MUC.
Truly, they were the ones living in an echo-chamber, not the rest of the world. And I got to learn from experience. I was there. Spending all of this time online, on XMPP, chatting with people who confirmed my biases. This small, insular community online. Not actually engaging with the substance of conflicting viewpoints, just using rhetorical tricks to dismiss them to free myself from cognitive dissonance.
I mean, I remember on one of the occasions where I pseudonymously entered the digdeeper MUC to chat, after having officially abandoned the place, one imbecile laughed because I dropped a Wikipedia article. This very same person probably lives their life thinking of how the sheeple masses are programmed into closed-mindedness, meanwhile they compulsively laugh if I so much as show them a Wikipedia article. They've been infected with a mind worm. All I need to do to set them off is write the word "Wikipedia", and all of a sudden they have this visceral, compulsive, emotional response, like an animal.
Wikipedia is not perfect, the quality of articles varies from page to page. The article I sent was a catalogue of third-party evidence for the Moon landings. It wasn't some historical article where the veracity of the information could be a real issue. It's the equivalent of sending somebody a wikipedia page with the statistics of golf players. It's a list of third-party observations, with the names of each observation event, which can then be searched up online. It's certainly not something to be dismissed out of hand. Saying "This is from Wikipedia, therefore it's wrong" is not a substantive argument.
Now, if you have an actual basis for discrediting Wikipedia, that's different. Depending on the context, you can dismiss certain things, but only after presenting your basis for discrediting the source. This person had no basis for discrediting anything, they were just some fool.
I suppose I'll start off with digdeeper's article "Dirty tricks of conspiracy deniers", as it contains many solid examples of his self-impeding conspiracism.[2]
"Dirty Tricks of Conspiracy Deniers" is a deeply contradictory article that betrays its own logic, in respect to scientifically-based reasoning behind conspiratorial thought.
The article's introduction creates a portrait of an all-present conspiracy to get the masses to trust mainstream narratives to their own detriment, in service of empowering some nebulous group of conspirators.
He introduces the "dirty tricks", presumably rhetorical tricks, that he will speak of.
He characterizes anti-conspiracy thinkers as cultish.
He speaks of certain individuals as "anti-conspiracy" thinkers, almost in the sense of being persons who only believe in "official" narratives, persons who will only believe something if it has the government stamp of approval on it.
I think you probably won't often find people who are "anti-conspiracy", in the sense that they literally only believe in official narratives presented by governments or large authoritative organizations of some form. You can find people who generally believe in the narratives that portray these governments and/or large authoritative organizations as not being purely sinister conspirators, concocting devilish conspiracies, but they usually do this on the basis of actual evidence.
There are some people out there who could be deemed disingenuous "skeptics", that do not consider the evidence relating to an event in its entirety. They tend to be snarky, and full of themselves. Honestly, off of my personal experience, only a few come to mind. They were liberals who were Zionists, who probably to this day think fondly of Obama and Hillary, and who denied things like how the U.S. Government deliberately concocted lies about Saddam Hussein's government in order to justify the invasion of Iraq. They do this out of their ideological investment in neoliberalism. They are unable to reckon with its reality, for how it would show their supposed belief in egalitarianism to be disingenuous.
Either way, I haven't seen these sorts of disingenuous people around COVID conspiracies, or likely any of the conspiracies that will be brought up.
With that being said, digdeeper is preparing us to witness how he is going to unmask cult-like behavior perpetuated by the establishment to the masses:[3]There is an army of people out there whose goal is to make you automatically trust mainstream narratives on all topics and dismiss all others even as possibilities to explore (and you - as a reader of this site - do not like being such a mental slave, right?). To accomplish this, they have given up all pretense of fair play and are just throwing all the dirty tricks they can find at you. It's a war - only for the mind space instead of physical territory; and in war, everything is allowed (or so they think). So far, the anti-conspiracy cult leaders seem to be winning the war. Their traps are varied and numerous; a person that's not careful is likely to fall into at least one, and become a victim of the cult. They seem to have gained a lot of grunts during COVID, in particular. Grunts that went around social media, doing the jobs of the higher-ups by - usually - repeating their tricks. This article is my attempt at reclaiming the lost souls, before they fall too deep into the anti-conspiracy swamp and become YouTube influencers attacking conspiracy theories (ugh). And - of course - to convince the conspiracy theorists that we are on the right side of history and keep them around. Hopefully by exposing the shady behaviors of the cultists and showing that the conspiracy-denying emperor is bare - we can begin tipping the scale towards our side, and win the war in the end. So let's go:
Science denialism comes in many forms: climate change deniers, people who are anti-vaxxers, who believe COVID is a hoax, that evolution isn't real, and who think the Earth is flat.
He quotes a CBC article after linking to it, which I have cited here.[5] Let's look at the article:
>How to convince a science denier to reconsider their beliefs
>It's possible to change the mind of someone who holds views that aren't backed up by scientific evidence, according to science philosopher Lee McIntyre.
>Science denialism comes in many forms: climate change deniers, people who are anti-vaxxers, who believe COVID is a hoax, that evolution isn't real, and who think the Earth is flat.
>McIntyre spoke to Quirks & Quarks host Bob McDonald about how science deniers construct and defend their beliefs with evidence-based insights into how to change their minds.
>Here is part of their conversation.
>You write in your book that there's a common script behind all science denial reasoning, and that if we know the script, we can change it. So, what is the script?
>This script was discovered by Mark and Chris Hoofnagle, and it was developed further by John Cook and Stephen Lewandowsky, who are cognitive scientists and it goes like this: there are five tropes of science denial reasoning.
>Every science denier cherry picks data, believes in conspiracy theories, engages in illogical reasoning, relies on fake experts and denigrates real experts, and here's my favourite: that science has to be perfect in order to be credible.
This is all true, conspiracy theorists that effectively deny "science" do cherrypick evidence. Digdeeper will literally do this in just a few moments, as you will see. It's impossible for conspiracists not to cherrypick, because if they didn't, they wouldn't be conspiracy theorists who all but deny "science" in terms of its most influential, well-evidenced theories such as evolution, or climate change, or globular earth. If you reject these theories, you aren't a "scientific thinker", it's true.
Continuing with the CBC article:
>There was a study in Nature Human Behavior in June of 2019 which vindicated that model. It's called technique rebuttal and I was very gratified to see that that was really the first empirical evidence to show that it could be effective in convincing science deniers to give up their beliefs.
>Technique rebuttal is simply to understand those five tropes and to learn how to use that to push back. So, for instance, somebody who claims that science has to be perfect to be credible.
>Often, I would say to the flat Earthers something like, "OK, so you claim that you're being more scientific than the scientist?"
>"Yes."
>"And your beliefs are based on evidence?"
>"Yes."
>"So what evidence would it take to convince you that you were wrong?"
>They weren't prepared to talk about that. And my experience is that if you listen to somebody and you make it clear that you're respecting them as a person — even if you're not respecting their belief, but you asked them why they believe it — they'll eventually say something that you can use.
End of quoting
Digdeeper goes on to quote a livescience article:
>The U.S. has a science problem. Around half of the country's citizens reject the facts of evolution; fewer than a third agree there is a scientific consensus on human-caused climate change, and the number who accept the importance of vaccines is ticking downward.
I will continue quoting the article: [6]
>One key thing to understand about people who engage in science denial is that very few people deny science as a whole, according to research by Yale University psychologist Dan Kahan, also presenting at SPSP on Saturday. For example, the more liberal a person is, the more likely he or she is to agree that humans are causing global warming; a conservative is far more likely to blame natural climate variation or say scientists are making the whole thing up.
>But that same conservative may be just fine with the evidence for the efficacy of vaccines, and there is virtually no partisan split on issues like the safety of nanotechnology, the use of artificial sweeteners in drinks or the health impacts of living near high-voltage power lines, Kahan wrote in a book chapter soon to be published in the "Oxford Handbook on the Science of Science Communication."
It is also true that people who believe in false conspiracy theories, usually scientifically-related, often do not reject all scientific knowledge and research. One thing you can see with them is that they will sometimes join in on mocking flat earthers, or become angered when they are compared to flat earthers. Digdeeper does this in his article. They don't understand that the things they believe are really only slightly less dumb than what flat earthers believe, and ultimately are conclusions they've reached by the same rhetorical tricks as flat earthers. They've merely reached a less severe outcome. In their lack of self-awareness, they become angered.
Digdeeper then quotes a third article from the APA: [7]
>On hot button topics such as climate change, vaccines, and genetically modified foods, science denial is rampant—and it crosses party and ideological lines. What are the psychological forces that lead people to disbelieve scientific consensus? Is science denial worse than it’s ever been?
I'll give further context:
>Since the beginning of the COVID-19 pandemic, misinformation has often seemed to spread as fast as the virus itself. Millions of people have disregarded scientists' advice on vaccines and masks and tried unproven and potentially unsafe treatments. It's the latest but far from the only example of science denial and of how public doubt and disbelief of science can harm people's health and the health of the planet.
>Science has become polarized and politicized, but science denial crosses party lines. On hot button topics such as vaccines, climate change, and genetically modified foods, people across the political spectrum are susceptible to the psychological forces that lead them to disbelieve what scientists are telling them and to seek out information that confirms rather than challenges their biases.
>But the other thing for us is that it is now deadly. There is no other time in history that we can think about science denial causing so many deaths. There are people who are denying to the grave right now. We have so many examples of people who are on ventilators and who are still resisting the fact that it could possibly be COVID because they believe it's a hoax.
This happened, you can find several instances on YouTube of people who acted foolishly regarding COVID, and sadly died, or nearly died, as a result.
Okay, that's enough; you can find hundreds more with a similar theme if you really want to. All these sources assume that "science" is some kind of an oracle that "says" a particular belief (such as climate change or certain COVID narratives) which you're then supposed to accept to be a good scientific and rational boy / girl.I never saw anyone in those articles assume science to be an oracle that dictates specific beliefs. People reach beliefs through scientific research, which we'll be getting into. That being said, another characteristic of conspiracy theorists who reject scientific knowledge and research that they dislike is melodrama. They recall the words of their perceived opponents in the most dramatic sense possible.
If science was some oracle that dictated certain beliefs, there wouldn't be any scientific research. There would just be people sitting around, regurgitating propaganda in common life and in institutions. But this doesn't happen. Research is conducted, new things are learned, and over time, scientific knowledge, what is widely regarded as being "true" more or less, evolves.
The people in those articles spoke of belief in "science" as the adherence to certain practices, in relation to certain beliefs reached through scientific research. For example, adherence to things like vaccination, or social distancing during COVID, on the basis that COVID is a harmful disease, as determined by scientific research, and that things like the COVID vaccines were safe, certainly safer than COVID, and were effective at preventing COVID, certainly more effective than natural immunity. You may disagree with this, you may think otherwise, and you're wrong for that. I will be getting to the COVID section later (I've already gone over it as I'm writing this section). This is going to be a relatively comprehensive analysis.
Now let's contrast that with what science is in reality. From our beloved NASA:
>Science is . . . Observing the world. Watching and listening Observing and recording.
Not quite. This distills "science" down to a meaningless string of verbs. You didn't fully quote the article. Let me quote it in full: [8]
>Anyone can have an idea about how nature works. Some people think their idea is correct because "it seems right" or "it makes sense." But for a scientist (who could be you!), this is not enough. A scientist will test the idea in the real world. An idea that predicts how the world works is called a hypothesis. >If an idea, or hypothesis, correctly predicts how something will behave, we call it a theory. If an idea explains all the facts, or evidence, that we have found, we also call it a theory.
>"Scientific method" usually means a series of steps that scientists follow to discover how nature works.
>These steps will work fine for a school science fair project. But this is not usually the way science actually happens!
>Sometimes the observations come before the idea or theory.
>For thousands of years, people observed certain "stars" wander around the night sky in looping patterns. Finally, in 1514 Nicolaus Copernicus came up with the idea of "Heliocentrism" (meaning Sun centered) ... That idea explained the wandering patterns of the planets. It also predicted where they would "wander" next. This idea became a theory.
>Sometimes science happens mostly inside a scientist's head.
>Albert Einstein and his theories were like that. It took a long time before scientists were able to test them and show that they were correct.
>Science is not just a tidy package of knowledge.
>Science is not just a step-by-step approach to discovery.
Science is not some uniform method of gathering knowledge. It's not just "the scientific method" or something. It is somewhat amorphous in how it is conducted. However, it has some key features. The core aspects of the process of scientific reasoning are falsification and prediction. The testing of ideas to determine whether they are false or true.
Where certain beliefs can become unscientific is when they persist in declaring the world to be a certain way when their claims about reality are demonstrably false, or their claims are inherently unfalsifiable.
So, anytime a mainstream shill tries to call you un- or anti- scientific because you deny their pet theory or agree with a "conspiracy theory", you can send them to NASA for the corrective lesson.
You can send them to NASA, where they will hopefully read the full article, and find absolutely no contradictions. Nor does it really matter what some random, anonymous person who works for NASA wrote on a webpage. They don't dictate the ontology of human knowledge and thought. You yourself are treating "mainstream" sources like NASA as an oracle, while supposedly critiquing others for doing this, when they are not even doing this. Conspiracists often make appeals to authority like this, we'll see this happen a lot later on.
Considering the necessity of falsifiability and predictability, people might not be unjustified in calling you anti-science. Asserting the world to be flat is un/anti-scientific, as there is a mountain of evidence proving this to be false, and that evidence all demonstrates the earth to be a globe. The flat earth model's predictions, what little there are, fail. Plenty of globular earth model-related evidence can be tested on your own.
To reject the fact that the earth is a globe demands that you deploy rhetorical techniques in order to discredit evidence that says otherwise. In doing so, you save yourself from having to actually grapple with the evidence. This is not scientific. This is dogmatic.
Asserting that all (or most) vaccines cause long-term harm to many people by causing autism, is also un/anti-scientific for many of the same reasons that flat earth would be unscientific. However, there is a difference. You can test the flat earth hypothesis on your own. To continue believing the earth is flat in spite of your observations proving otherwise would probably require you to disbelieve your external and internal senses.
You as an individual cannot test the hypothesis that vaccines cause autism. To test that hypothesis necessitates a lot of scientists performing long-term studies. At this point, you introduce the potential of conspiracy. If a bunch of scientists from all over the world test the hypothesis of vaccines causing autism, and determine this to be false, they could all be in on a conspiracy to hide the truth that vaccines do cause autism. But, assuming there is no evidence of a conspiracy, you must presuppose that however many people it would take to pull off that conspiracy can keep it a total secret. That presupposition of yours will allow you to deny evidence that conflicts with your belief that vaccines cause autism — a belief for which you would not have actual evidence. A scientific theory is not a criticism of other existing theories that does not make any of its own predictions. It is a series of facts that are woven together to create a coherent theory that makes predictions about reality. Your opposition to the evidence-based consensus on vaccines would not be something scientific.
The same can be said of the harmfulness of COVID mRNA vaccines. You as an individual cannot verify if COVID mRNA vaccines are more harmful to society than COVID itself, as this necessitates a large amount of studies into the vaccines, what harms they can cause, the frequency at which these harms can be caused, and comparison against COVID, and against alternative solutions proposed by people who dislike the vaccines e.g natural immunity.
You as an individual, with respect to things like the harmfulness of vaccines in general, or of COVID vaccines, can formulate an opinion of them based on anecdotal evidence. But anecdotal evidence is biased towards the individual, and only corresponds to their subjective view of reality. It is not empirical evidence that points towards an objective reality, external to one's subjective, lived experiences. This is why scientific thinkers do not rely solely upon anecdotal evidence.
Can anecdotal evidence prompt scientific study? Absolutely, and historically it has done this. But, once the research is conducted, and the anecdotal claim appears falsified, the justification behind that anecdotally-based belief is greatly diminished. Alternatively, one can find scientific evidence to justify the anecdotally-based belief, this also happens. More often, people find that there is some truth to an anecdotal belief, but that it is not entirely true, and there are elements to it that they were previously unaware of, and they develop a nuanced perspective through researching it.
Vaccines and COVID vaccines have been studied to determine their harmfulness, which has found that they are very safe. As such, rhetorical techniques must be deployed to discredit the evidence pointing towards vaccines being largely beneficial and safe. This is not scientific, however. It ultimately leads one to absurdities, like the belief that tens to hundreds of thousands of people across the world, from all different walks of life, with all sorts of differing beliefs, and potentially vested interests in actually working to undermine one another rather than to collaborate in a conspiracy, could keep a conspiracy totally secret.
Now, you may be thinking, They haven't kept it totally secret
, or Evidence in favor of my conspiratorial belief exists
. I don't doubt that you personally believe that there's evidence pointing to the ousting of a conspiracy, or that you have scientific evidence. But, you have to actually grapple with that evidence, you have to actually analyze it.
This is a common fallacy perpetrated by conspiracy theorists. I'll call it an appeal to dissension. They falsely think that if there's an "expert" in some field who disagrees with the consensus regarding something, then the consensus cannot be deemed true, or cannot be entirely true. This doesn't necessarily follow. You need to actually look into the reasoning of the "expert" in its totality. In doing this, you'll often find that the "expert" is wrong. The process of doing this can be laborious, far more time-consuming than the average person can manage, and so most conspiracy theorists never bother to do this.
The same fallacy is made with respect to the supposed ousting of conspiracies, such as by phony whistleblowers. The conspiracisy theorists will point to a supposed whistleblower, who purportedly exposed a conspiracy to falsify evidence for something like, climate change per se. But they don't actually analyze that situation in its entirety, and ultimately discover the "whistleblower" to be a liar of some sort. Just because there is a dissenting voice somewhere does not mean that a truth which is agreed upon by many people is not actually true.
Asserting that 9/11 was an inside job is not necessarily anti-science.
It depends on the scenario. For instance, to postulate that it was a controlled demolition is not anti-science. That is physically possible. Controlled demolitions of buildings are possible. Things like C4, semtex, and thermite exist. Now, something like saying a DEW (directed energy weapon), or miniature nuclear device took the towers down is definitely not scientific, that would be anti-science. While theoretically possible, those situations are not actually possible in reality, given the nature of DEWs and nuclear weapons.
Conspiracies relating to 9/11 being an inside job are similar to things like the vaccine-autism hypothesis, or conspiracies about COVID mRNA vaccines, in the sense of the breadth of the conspiracy. Conspiracies such as this become a matter of compiling evidence, determining the evidence's credibility, and attempting to determine the probability of a scenario to have happened a certain way. The issue is that when discussing the conspiracy theory, any particular theory can never be proven or disproven as being right or wrong to an absolute certainty. However, a person who believes/disbelieves a particular theory must have some presuppositions that they hold to be true. For instance, if you believe 9/11 to have been an inside job, you have to believe that however many people it took to demolish the Twin Towers and WTC 7 can stay absolutely silent and you have to believe that they rigged the towers to blow without leaving any forensic evidence of this behind. This is not a rational presupposition, however.
Attempting to rationalize such presuppositions by citing exposed conspiracies like the Manhattan Project is a non-starter, more on that later.
Continuing with digdeeper's article: [2]
Again, nothing about science "saying" something and requiring you to "accept" it. The modern Orwellian redefinition of science as "something that says" is just an attempt by authoritarians to claim it as a vehicle for spreading their pet theories, or burying undesirable ones.
You have yet to even demonstrate people demanding you to accept certain things. People provide moralistic reasons for why you should accept scientific ideas. Because most people are moral — I think at least — and have some moral obligations they likely adhere to, thanks to how they were conditioned by society, they perceive these suggestions as demands. But they aren't.
And since science radiates an aura of respect, it would obviously be the first target for thought control attempts. But the real definitions actually make it clear that science cannot reject any theories apriori - not even "conspiracy theories" - as long as the proper methodologies are followed.
You are correct that theories can't be rejected a priori. But the thing is... they aren't rejected a priori. There's a reasoned basis for their rejection. Your perception of theories being rejected a priori likely comes down to a failure to fully track the chronology of the discourse of ideas.
There are also scientific theories that are so robust that they effectively rule out other theories. The globular model of the earth would be a rudimentary example. Scientists aren't going to waste their time seriously considering some new "proof" of flat earth, if all of the work they're doing hinges on a globular model of the earth, and that model does permit them to perform their work perfectly, as intended. They already know that flat earth is nonsense, because every day they perform work that they couldn't perform were flat earth true. The same can be true for other theories.
Or in the words of William James, founder of Society of Psychical Research, who studied (among other things) mediums (and discovered results he could not conventionally explain):
William James, an influential philosopher who also had some irrational beliefs, much like all people. This is another fallacious line of reasoning made by conspiracy theorists. They think that if a person they view as being influential holds an irrational belief, that irrational belief must be true, or is at least credible. It's an appeal to authority.
It can be on the basis of intelligence, like with William James, but it can also simply be on the basis of power. Take for instance things like hyperbaric chambers, or receiving transfusions of blood from young people. These are things that some grotesquely wealthy psychopaths practice. But they're also pseudoscientific placebo treatments. They are the desperate attempts of psychotic individuals with too much money, who wish to live forever, trying to transcend their temporal existence. It says everything about their character (particularly vampiric practices like taking the blood of young people) and nothing about the veracity of those practices.
Many people seem to believe in universal intelligence. They don't realize that intelligence is often regional, and not universal. That people can be very intelligent in regards to certain things, in terms of the veracity of their beliefs, and the influence of their beliefs by how compelling they are, but not very intelligent when it comes to other things. William James could be an example, although I'm not much familiar with his philosophy. Conspiracy theorists often believe in this sort of universal intelligence.
>Science means, first of all, a certain dispassionate method. To suppose that it means a certain set of results that one should pin one’s faith upon and hug forever is sadly to mistake its genius, and degrades the scientific body to the status of a sect.
This is true, to which I ask, what is more dispassionate i.e scientific: a double-blind, randomized, placebo-controlled trial, or scouring the internet for anecdotes tailored towards your personal worldview? The answer is obvious.
Degrading "the scientific body to the status of a sect" is exactly what the anti-conspiracists are doing. All while historically, science has been about people questioning and eventually toppling the prevailing views; usually, many competing theories were around at the same time. This has happened in physics, biology, everywhere; and is still happening when you actually look into the journals instead of relying on media coverage (the mainstream media is almost entirely controlled by the authoritarians). When Darwin came around to challenge Lamarck, no one screamed about the alleged destruction of science. It was simply accepted as something natural; but if the authoritarians were in charge, we'd be stuck with Lamarck forever (not that I think Lamarckian views are somehow worse; in fact they are having a resurrection these days - just showing an example of the perils of "scientific" authoritarianism).
Lamarckian views are not having a resurrection. That website ostensibly postures as some scientific, anti-creationist source of knowledge, but is merely a pipeline for people to effectively become creationists, by surmising a divine force to have created life.[9]
Scientific progress is driven by the refutation of consensus, which typically results in an advancement of knowledge. That simply hasn't happened with the scientific conspiracies you believe in, like with the COVID vaccines.
You essentially compared conspiracy theorists to people like Darwin. There's some differences between the two. The academic debates held around the mid-to-late 1800s into the 1900s regarding physics, mathematics, and biology, were held by — well, academics. Experts in a particular field. These experts sometimes held correspondence with each other for a while before beginning to debate each other in front of other people. When they did debate physically, they would debate among other experts in their field. Eventually, whichever stance was most tenable would win out. This could take a very long time as the evidence necessary to prove/disprove a theory was not always immediately available.
Being a person on the internet who cherrypicks scientific studies that they do not comprehend is not the same thing as being an academic engaged in long-form debate with other academics. You can point to academics who promote your conspiracy theories, but in the context of your website, those people are wrong, which I'll get to.
Many of the "debates" that you view as being unsettled are in fact settled. Now, no matter is categorically "settled", but there are conclusions people reach through research and discussion, which have a long-term impact on how they operate in their lives. You could say that heliocentricity is unsettled, for instance, but you'd be an imbecile for saying that. Realistically speaking, rationally speaking, it is settled. You can then decide to tredge up a bunch of old arguments, and rehash them, and then be ultimately disproven, wasting everyone's time, but that'd wouldn't be an efficient use of your time. It's dumb.
Most people will not waste their time with such nonsense.
It is not the "anti-conspiracists" degrading the scientific body. It is conspiracists, like by bringing into question subjects like the current theory of evolution, or climate change, or the effectiveness of vaccines. They're wasting everyone's time, sowing doubt, and encouraging others to believe in things that are wrong, which has harmful effects upon society, for one by causing disease and killing people, but secondly, merely by eroding trust in society, and causing people to become more vulnerable to supposedly "anti-establishment" swindlers, see it happen with Trump.
They're actively reversing the advancement of human knowledge. It's anti-intellectual. All that "anti-conspiracists" have done is adhere to consensus, as dictated by falsifiability and predictability. That's science. Refute the consensus, the burden of proof is on you. That's what everyone has done up until now, including Darwin and Copernicus and whatever other brilliant scientists you want to attach yourself to.
You falsely view yourselves to be like Darwin or Copernicus, or Semmelweis, but you aren't, you're just deluded. You're nothing like Semmelweis or any brilliant scientist who put out ideas that could not be falsified at the time of their advent due to technological and scientific limitations. Semmelweis' ideas were later vindicated as scientific knowledge advanced. You are simply misinterpreting evidence that already exists, and refusing to listen to criticism of your misinterpretations. Your arguments have nothing to do with our potentially limited abilities in observing reality and how these relate to current scientific theories, you're too disinterested in actual science to engage in such discussions. Your arguments relate to the veracity of information pertaining to subjects of which conspiracies are concocted. Modern medicine, COVID vaccines, the Moon landing, 9/11, and so forth. This is nothing like surmising that there's something on the hands of medical practicioners which is causing infections, after correlating handwashing with lowered patient mortality, but being unable to demonstrate qualitatively what it is on the hands that is causing death.
The article from NASA you cited literally mentions how not all of Einstein's ideas could be falsified at the time they were presented. Did people tear down Einstein and shun him? Did the evil establishment of consensus crash down upon him? No. He was a legitimate, reasonable scientist, he didn't behave in the manner of a conspiracy grifter, which is why this never happened.
Analogies pertaining to figures like Semmelweis or even Einstein could hardly apply to anything coming from individuals who concoct scientifically-related conspiracies. These figures' ideas went on to be validated, usually within a few decades. They introduced novel, revolutionary ideas such as the concept of something on human hands causing illness, or a hypothesis pertaining to light that would force us to completely restructure how we view reality. This category of revolutionary ideas is not remotely similar to thinking that the Moon landing didn't happen because we didn't keep going there over and over again until this very day.
The other scientifically-related conspiracies brought up in this article e.g modern medicine being ineffective, COVID vaccines being largely harmful, are also not similar either, I've been over them already as I'm writing this.
Of course, authoritarians using science as a cover have always been around, and they always brought disaster with them - "In 1847 Semmelweis, who was an obstetrician, (a doctor specializing in childbirth), published evidence that when doctors washed their hands before examining or treating patients, the mortality rate for women in his birthing ward in Vienna, Austria, was greatly reduced"; "Semmelweis had become clinically depressed when his work was rejected and he started behaving oddly. He was lured by another doctor into an insane asylum in Vienna. Realizing it was a trap, Semmelweis tried to get out, but was held and badly beaten by guards and placed in a straightjacket. He died two weeks later, most likely from injuries he suffered during the beating". The peak of "scientific" authoritarianism is murder of the dissidents. Today, it happens to be the anti-conspiracy community playing that role and holding science and humanity back.
It is deeply ironic for one to say that the anti-conspiracy community are the ones holding science and humanity back. The scientists in fields relating to biology who continue to advance human knowledge, making discoveries, in relation to their theory of evolution. Or people who develop and distribute vaccines, which have historically saved the lives of countless people, and made premature death to disease less of a commonality. Or people who went to the Moon. This is a completely absurd reversal of the reality of the situation, which is again common amongst conspiratorial thinkers.
You'd think people would finally figure out to not fall for their tricks, but somehow they don't. Funnily, when they accuse anyone who refuses to bow down of "science denial", they end up being the actual science deniers because they deny that popular theories can be questioned - when it's the essence of science to do so.
Who is denying that popular theories can be questioned? You can question whatever you want, it doesn't mean that you're right.
Again, science cannot reject theories - not even conspiracy theories - apriori. Appeals to "scientific consensus" appear every so often in the authoritarian publications as an excuse for rejecting theories; about that, I will just quote Michael Crichton:
>I want to pause here and talk about this notion of consensus, and the rise of what has been called consensus science. I regard consensus science as an extremely pernicious development that ought to be stopped cold in its tracks. Historically, the claim of consensus has been the first refuge of scoundrels; it is a way to avoid debate by claiming that the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had.
>Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics. Science, on the contrary, requires only one investigator who happens to be right, which means that he or she has results that are verifiable by reference to the real world. In science consensus is irrelevant. What is relevant is reproducible results. The greatest scientists in history are great precisely because they broke with the consensus. There is no such thing as consensus science. If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.
What Michael Crichton's saying here sounds appealing to the science-illiterate conspiracist, but upon scrutiny falls apart.
What is science? Well, it is in part a process of theorization that adheres to falsifiability and predictability, as I mentioned earlier, but when considered as an entity, it is a body of knowledge. That body of knowledge, in order to be uniform and coherent, must be driven by consensus. People have to have things that they agree upon, and they have to agree upon most things. Not necessarily everything. The things they don't agree upon will usually be ongoing fields of research and matters that aren't entirely settled.
Knowledge will be obtained through scientific research, subjected to rigorous standards, and entered into this larger body of knowledge by an advancement of the consensus. The advancement will usually either be a refutation of the consensus, or merely a contribution to the knowledge-base of the consensus, which broadens its perspective.
You cannot have a unified body of knowledge without consensus. It's absolutely necessary in order to have it. The alternative is centralized curation, which is authoritarian, and flawed.
Science has always been consensus driven. There hasn't been a "development" of it, it's always been here. There has been a development, that is, a rise in the popularity, of scumbag grifters, like Michael Crichton (climate change-denier), preying on gullible people in society, which has had significant, harmful effects upon society, and there has thus been a greater need to rely upon the knowledge dubbed 'scientific consensus' to refute them.
Here's the issue with your interpretation of Crichton's statement. When you think that one investigator may be "right", they could in actuality have come to a conclusion due to faulty practices or unreliable data or any other number of reasons. This is where reproducible results come into play. The consensus that Crichton ought to be speaking of here is reproducible results in relation to the current base of knowledge, though I doubt that is what he is actually talking about, I'm only saying he "ought" to be, so that I can glean something valuable from his otherwise worthless words. Peer-review (I don't know how you feel about it, but a lot of conspiracy theorists seem to view it as a weapon of oppression) is merely falsification by other scientists. It is reproducing an experiment to see if you get the same results. If you do not, then you try to figure out why that is, and it might lead to the conclusion that the experiment's hypothesis is false. If you wish to shift the current base of scientific knowledge, the burden lies with you to demonstrate that some part of that knowledge is false. Merely asserting things to be a certain way is not good enough, because anyone can do that for any reason. Truthfulness has nothing to do with it.
Assuming that you have evidence which could suggest something to have been falsified by a conspiracy, and this evidence is refuted, then the conspiracy is disproven. If you do not have evidence, or you continue believing in the conspiracy after the evidence has been refuted, you've all but abandoned scientific thought. At that point, you are deciding how probable a particular set of circumstances was to have happened. For example, how probable it was that we went to the Moon. If you have no basis for determining the probability, then the probability is literally just a baseless opinion of yours. It's akin to thinking the earth is flat because it looks flat, and questioning the chances of the earth being a globe caused by the Big Bang etc etc. It is a primitive, instinctive thought process. You can think that way, nothing is stopping you, but it's not rational in the slightest, don't bother pretending otherwise.
This is when the conspiracy denier picks the least serious, weakest, or most "out there" conspiracy theory to insert inside the box with all the others and dismiss them together. It is like releasing a skunk into the zoo to prevent people from checking out all the other animals. Some examples:
There is a reason why people lump conspiracy theorists together. There is no uniformity within their thoughts. The only common denominator is that they don't believe in official narratives. There's an endless variety of conspiracy theories. When it comes to real history, there are different interpretations of events, but they all tend to agree on most important things, and there's not a million wildly-different interpretations. Take the issue of Israel and Palestine. There are not many overarching interpretations. There are many granular interpretations of the issue. But, when it comes to large events, many people can agree on certain narratives. This creates a coherent, somewhat unified discourse.
To give an analogy, in the conspiracy community, people can't even agree on whether or not Israel and Palestine are actual places that exist, that it's not just a whole conspiracy to fool us for the secret reason. Non-conspiracists could at least agree that these places do exist, because they have that level of rationality. They could also agree on certain events having happened, like atrocities committed against Palestinians during the Nakba, but Zionists may have their (false) justifications for these atrocities. They can at the very least acknowledge that they indeed happened. In the conspiracy realm, they can't even do that. There's zero cohesiveness.
Essentially, conspiracists can't even get off the ground. They can't start the engine.
The reason why people focus on the most outlandish theories is because those are the most sensational and laughable ones. You are expecting people to magically know what you think before you have layed out your exact beliefs. Still, I'll concede that some people do use flat earthers in order to mock other less gullible conspiracy theorists. For this reason it's important to establish exactly what a conspiracy theorist believes, point by point. Something you haven't done much of beyond your article on COVID. You're not helping yourself here. You've been speaking vaguely this entire article.
Vaccine and climate change skepticisms poisoned by the association with the flat Earth. The conspiracy deniers know that if a person dares to research a really well supported conspiracy theory (such as the 9/11 demolition theory or the moon landing hoax), they will forever be free from the mainstream mental chain.
If those are your most well supported theories, then you don't have much. The Moon landing conspiracy is a joke.
I feel that this relates less to dismissing conspiracists as psychologically defective, and more about understanding how they come to possess their beliefs. This is useful in understanding the sociological phenomena which drive conspiratorial beliefs in society. The example you've given may focus more upon conspiracists as individuals, but overall, there's value in psychological analysis of them for the sake of understanding what may have caused them to be as they are.
According to this site, people believe in conspiracy theories because they have these psychological traits:
>paranoid or suspicious thinking
>eccentricity
>low trust in others
>stronger need to feel special
>belief in the world as a dangerous place
>seeing meaningful patterns where none exist
There's nothing inherently wrong with most of those traits.
See, if our paranoia, distrust or pattern detection prevents us from eating cancer-causing GM food and / or injecting poisonous COVID vaccines - then we won
Yes, this is part of our primitive, instinctive, superstitious thought. Those instincts are not always wrong. You did not mention two of the more significant mental traits:
>stronger need to feel special
>seeing meaningful patterns where none exist
All of the mental traits can have genetic and environmental causes. You can't blame people for believing the world is a dangerous place if their life has lead them to think that. So the same for a low trust in others. But, when you combine a need to feel special and seeing meaningful patterns where none exist with the other traits, you can begin to hold irrational beliefs.
And when we do, it will be clear that the head-in-the-sand style psychology isn't doing the mainstream shills any favors (I could drop a few "died suddenly" cases here, but let's be nice
People die. This could be an example of seeing meaningful patterns where none exist. Most people probably die "suddenly".
We can rationalize our instincts. If they are true, then they were true, but if not, then they weren't. The point is that we don't operate solely off of instinct. Take Teflon as an example. When Teflon cookware first came out, nobody in my family used it. They avoided it. They were suspicious of it. It was a strange synthetic compound promoted by an untrustworthy company. Additionally — and this is important, it's what makes this homologous from COVID vaccines — there was no real need to be using it. Nobody was gonna die of respiratory failure for not using Teflon. In the end, their suspicions were proven correct after scientific study into Teflon was performed. Now there's supposedly safe versions of Teflon, so I guess it doesn't matter anymore, although I haven't bothered to see if they're actually safe, I just don't use the stuff.
To return to sociological phenomena. Our current capitalist system can cause people to develop the mental traits which, according to that study, are general to conspiracists. It doesn't happen instantaneously. Take a lack of job opportunity as an example. Lack of work is due in large part to automation. But, because of how much brainwashing there is in society, in respect to obtaining employment, and how one's inability to obtain employment is viewed more as a personal failure than a failure of an individual to triumph against an inhuman system, people can look to explanations other than automation, and they do for the most part. It becomes not the fault of automation, but the fault of "illegal immigrants", or of supposedly unqualified women, brown people, and black people, "stealing" jobs. Given America's history of racism, it can be easier for someone to blame minority groups for their problems as opposed to the system at large. Sometimes, these people may instead begrudgingly acknowledge that it may not be the fault of minorities, but that they still need to persecute those minorities in order to get themselves into a position where they can change the system. This, of course, will never happen, as they're playing into the game of oligarchs and politicians. And it never does happen.
Conspiracists often see the corruption of the government, and of corporations. They often have some awareness of their great crimes. But, they focus more on their fictitious crimes, the ones purported by conspiracy theories, than the real ones. This causes them to often have less knowledge of their actual crimes, which undermines their ability to produce positive change in the world. To the conspiracy theorist, the crimes of the CIA and of the NSA and of banks and corporations are merely a diving board for them to delve into their made-up conspiracy theory. The crimes don't quite get the attention they deserve, often they're even normalized by the conspiracists as facts of life, to be accepted. They will condescendingly tell you about how they know all about it, how it's nothing new, and then they will posture as being superior to you with their esoteric conspiracy knowledge. But do they really know all about it, or is it just a headline that they recall? They do not truly care for government corruption, or the ills of capitalism. It's more of a game to them. They want to feel special by possessing esoteric knowledge.
You get the drill. Anytime the conspiracy deniers mention a conspiracy theory, they strike it down with the relevant adjective (or more than one); and the opposite for the mainstream theories. Being exposed to such associations hundreds of times, eventually, your brain begins to attach the concept of conspiracy theories to falsity and mainstream theory to truth.
There is some truth to this point, when you speak of adjective-laced diatribes against conspiracy theories.
In my experience, I feel that information refuting conspiracy theories has become more difficult to find with the passage of time.
If you look for articles debunking conspiracy theories, often times the first things you find are very weak, nowhere near comprehensive refutations. Digdeeper brings it up of course, by saying that the establishment focuses on "weak" points in conspiracies, but ignores the "stronger" points. I don't think that they avoid "stronger" points, often times the unmentioned points are actually quite idiotic, but they are definitely far from comprehensive in their debunking.
This leaves wiggle room for the conspiracists. It gives them the opportunity to remain in their ignorance. I do not mean to excuse conspiracy theorists for remaining in their ignorance by not searching for more potent articles, with more comprehensive refutations of their beliefs, but there is undoubtedly blame to be set upon the mainstream media for giving them this opportunity. Now, of course, it is not the media's duty to conceive of every possible argument in favor of a conspiracy theory and refute it, but sometimes they do miss arguments that get a fair amount of circulation, and are perceived as being compelling.
When criticizing power, you often run into people who try to shift the failures of institutions onto the duty of "individuals". When speaking of education and conspiracy theories, while there is a degree of responsibility for individuals to learn things, this does not mean that institutions have not failed to educate them, and bear some degree of responsibility for this as well. This does not mean that institutions should not bother to educate them. This does not mean that we shouldn't address society's failure to educate people to an extent that they won't have certain false beliefs.
You have to understand that there are some people in society, quite a lot, who have slipped through the cracks in some way that has made them vulnerable to conspiracy theories, and who are probably not well educated, and who simply are not going to challenge themselves, and you have to be willing to reach out to them and address their incorrect beliefs. You have to be willing to go over just about every one of their arguments, and explain why they are wrong. People need to be willing to do this, and popular sources of knowledge need to as well.
At the present time, many people are unwilling to do this.
The great prevalence of conspiracy theories relating to evolution, vaccines, and climate change is a testament to our institutions' failure in educating us about these subjects. America, with its horrible standards of public education, is unsurprisingly the global hub of these sorts of conspiracy theories. Had people possessed a more robust knowledge, they would be less likely to fall victim to conspiracies regarding these scientific theories and technologies.
Our institutions haven't just failed in educating us, they've actively worked to diminish our understandings of these things. See how social media algorithms are designed to trap people within echo-chambers, and can gradually ease people into conspiratorial beliefs, by slowly serving them more and more content relating to conspiratorial ideas. Our governments should have regulations against these algorithms, in order to keep them from manipulating us into using them for as long as possible, as frequently as possible, which can entail bringing us down conspiracy pipelines, but they never will, as its not in their interest.
Search engines are designed to prioritize slop results, and websites often are designed to compete in this environment. This definitely contributes to the difficulty in seeking out comprehensive refutations of conspiracy theories.
I won't go as far to say that the average person should have a knowledge of evolution or climate change so advanced that they should be capable of refuting any argument a denier of those things will make. But, I think it would be fair to say that many people are not capable of persuasively counter-arguing these things. Often times, people will resort to appeals to authority. These appeals to authority aren't necessarily wrong, but they are not convincing argumentation. They don't provide an in-depth understanding of why something is wrong, and why the other thing is right. And this allows conspiracists to feel like marginalized truth-seekers, attacked for merely asking questions. You should be able to drive a denier of those things towards making irrational arguments. Your inability to persuasively dismantle their irrational arguments is not a personal failing.
Other times, when you look into conspiracy theories, you find diatribes denouncing them, with little substantive refutation of them. Holocaust denial is a good example. It's often shouted down as antisemitism in the Orwellian sense which digdeeper refers to. Sure, you can call it antisemitic. But that doesn't mean anything to the person who believes that it's an international jewish conspiracy. And it doesn't mean much to the "free-thinker" who doesn't know much about the Holocaust, and is passively observing your argument, beginning to question why you cannot refute the denialism, beginning to notice these lingering questions, these gaps in their knowledge that can't seem to be filled in, because they don't enjoy learning, and cannot find anyone who can spoonfeed them historical knowledge.
Shouting people down, dismissing them out of hand, or being perceived as arguing in this manner, can drive others towards believing in conspiracy theories. There's actually a somewhat valid instance of this on Luke Smith's website. Smith has this article where he reveals himself to be a racist imbecile. In it, he cites a debate between this scientific racist named Jean Philippe Rushton and a genetics professor named David Suzuki as a formative experience in his path to becoming a racist pseudo-intellectual religious fundamentalist. Maybe I'll publish my thoughts on that terrible article of his here some time.
In essence, Jean Philippe Rushton, some racist grifter, debated a geneticist named David Suzuki. The subject was whether or not black people are genetically inferior beings. Rushton gish gallops his way through the debate, making a bunch of weak arguments. Faced with this onslaught of weak arguments, instead of individually refuting them one by one, Suzuki resorts to rhetorical techniques to dismiss them and nullify Rushton's case, while also appearing to be quite emotional, in stark contrast to Rushton who was largely calm and collected. Make no mistake, Suzuki's rhetorical refutations are not invalid. But, when you're dealing with a collective audience, which will contain stupid people e.g Luke Smith, this won't appear convincing. People will begin to wonder why you're not grappling with your opponent's arguments. They'll begin to wonder why it's largely tautologies that you're throwing out. These are ignorant people who do not understand the scientific bases for these tautologies, and you have to guide them towards those bases. Right here is a quote from the comment section of the Rushton-Suzuki debate:
Suzuki did not dispute any of Rushton's data, nor did he present any of his own alternative explanations as to why these differences exist.
Suzuki did offer alternative explanations, and did dispute some of his data, but he didn't do this in a sufficiently convincing manner. He should have delved into Rushton's fraudulent work, and exposed it live, but he didn't, for whatever reason. This left these lingering questions for the dumb viewers of the debate.
Again, I don't mean to completely shift the blame off of individuals here. You could easily look into the points that both Suzuki and Rushton made, and you'd see that Rushton was a fraud, but many people, probably most people, will not do this. Evidently, Luke Smith did not do this.
Indeed, thorough refutations of scientific racism are uncommon in the mainstream.
But maybe I'm being unrealistic, maybe Suzuki should not have dismantled Rushton's weak points head-on. Either way, it's an example of the phenomenon I wished to express at play, albeit only a "somewhat valid" example.
When it comes to theories regarding subjects like scientific racism, regular people are in my opinion not largely to blame for their inability to refute them.
Scientific racists resort to increasingly abstract lines of argumentation as you argue with them. At a certain point, an average person may find theirself unable to adequately comprehend the evidence being discussed. They may instead simply make some logically fallacious arguments, which while valid, do not stand on their own as being valid.
In these cases, you need experts who can refute their misinformation.
Two culturally relevant purveyors of conspiracy theories who sometimes need to be refuted by experts are Avi Loeb and Eric Weinstein.
Some of the conspiracy theories they purvey can be refuted by anyone, but others may not be. For example, a regular person is not going to be able to examine Avi Loeb's physics calculations, which supposedly prove some object in outer space to be a spacecraft, and recognize the serious flaws in them, which nullify their conclusions. A regular person being confronted by a conspiracist with this sort of complex evidence (which the conspiracist theirself does not comprehend) is powerless. They have to rely upon others.
The same could be said for Eric Weinstein with his theory of everything. A regular person probably cannot refute such a thing. But, anyone with a formal education in physics above the high school level probably can.
When speaking of matters like the Holocaust though, anyone should be able to refute conspiracy theories. It's all history, for the most part. Undoubtedly, scientifically-related arguments may be brought up, but they're superficial enough that anyone can engage with them. An inability to do this reflects one's personal failure to educate theirself, and the failure of their system to educate them.
In the vein of historical conspiracies, I wouldn't blame the mainstream media for not effectively instructing people on how to refute Holocaust denial, because that's just hollow and pathetic. People's failure to refute historic conspiracy theories is borne of a lack of knowledge of history. You should not be learning about the Holocaust through some articles debunking Holocaust denial. Nor should you for any historic event. You should learn about it directly. Once you have a thorough knowledge of it, you can disarm some idiot in real time.
But from the perspective of refuting scientifically-related conspiracy theories, I feel that the media definitely deserves blame. A standard education may not equip you to deal with some particularly abstract scientifically-related conspiracy theories, and you may not have the time to study the topics relating to them in order to refute them without any guidance. Some level of guidance is necessary.
Yet still, the media is not obliged to refute conspiracy theories 24/7. There are times where writers may bring up a conspiracy theory, and do not want to tacitly validate it, so they may attack it with adjectives. The alternative is that they demonstrate why those conspiracies are wrong every single time they write an article in which they bring them up, completely abandoning the intended subject of the article. They could instead depend upon people to do their own research, to actually lift a finger to learn something. Like I said: cohesiveness. People shouldn't have to rehash the same stuff over and over again. You'll never get anywhere if you live like that. Some things are better off leaving as "settled", under certain circumstances.
I will not be giving digdeeper a bunch of adjectives, I will be giving him a reasoned, evidenced opinion, which will leave him to be the one making rhetorically-based arguments.
We will cover two topics here: COVID-19 and the moon landing; though this applies to every single conspiracy theory out there. Let's start with corona:
>Hydroxychloroquine, an antimalarial drug, is a cure-all drug for the coronavirus.
>COVID-19 vaccines plant a tracking chip in your body.
>Certain flu vaccines carry the coronavirus instead.
>Wearing a mask increases your chances of getting COVID-19.
No one claimed HCQ is a cure-all, just that it works. Nice try, exaggerating the claim to the highest possible extent so that people think it's "too good to be true" and just dismiss it completely.
The difference is insignificant, because the outcomes are the same. HCQ doesn't and did not help treat COVID, and encouraging people to use it put their lives in danger. Whether someone takes it to treat their COVID, or to use it as a "cure", whatever the hell the difference should even be, the outcome is the same. So, whatever difference you perceive is irrelevant.
People could cause damage to their hearts by taking HCQ, which could kill them.
Many studies didn't find any benefit in the administration of HCQ, in mild and severe COVID cases.
Here is the first of several I will present: [14][15]
>Prophylaxis for COVID-19: a systematic review
>Results: We identified 13 studies (from 2119 database records) and 117 RCTs (from 5565 RCTs listed in the registries) that met the inclusion criteria. Non-RCT studies reported on cross-sectional studies using hydroxychloroquine (HCQ) in humans (n ¼ 2) or reported on animal studies (n ¼ 7), most of which used antibodies. All five completed RCTs focused on the use of HCQ as either PrEP or PEP, and these and the cross-sectional studies reported no prophylactic effect. The majority of ongoing RCTs evaluated HCQ or other existing candidates including nonesevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines, anti(retro)virals or use of vitamins and supplements.
>Conclusions: The key message from completed studies and RCTs seems to be that HCQ does not work. There is little evidence regarding other compounds, with all RCTs using candidates other than HCQ still ongoing. It remains to be seen if the portfolio of existing molecules being evaluated in RCTs will identify successful prophylaxis against COVID-19 or if there is a need for the development of new candidates.
No benefit was discovered
Here's another: [16]
>Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients With COVID-19
>Question Does treatment with hydroxychloroquine improve clinical outcomes of adults hospitalized with coronavirus disease 2019 (COVID-19)?
>Findings In this randomized clinical trial that included 479 hospitalized adults with respiratory symptoms from COVID-19, the distribution of the day 14 clinical status score (measured using a 7-category ordinal scale) was not significantly different for patients randomized to receive hydroxychloroquine compared with placebo (adjusted odds ratio, 1.02).
>Meaning These findings do not support the use of hydroxychloroquine for treatment of COVID-19 among hospitalized adults.
No benefit was discovered.
This study found increased risk of adverse events from HCQ without any benefit: [17]
>The efficacy and safety of hydroxychloroquine for COVID-19 prophylaxis and clinical assessment: an updated meta-analysis of randomized trials
>Background: Coronavirus disease 2019 (COVID-19), a disease that affected tens of millions of people, upended the lives of countless individuals around the globe. The chloroquine (CQ) and its analogue hydroxychloroquine (HCQ) were the most frequently cited as potential treatments and preventatives against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The primary aim of this investigation was to scrutinize the effectiveness and safety of HCQ for COVID-19 prevention and to present powerful evidence and reference for clinical practice.
>Methods: PubMed, Ovid and the Cochrane COVID-19 Register of Controlled Trials (CENTRAL) were systematically searched from inception to January 31, 2022. Randomized controlled trials (RCTs) trials that included participants who were SARS-CoV-2 negative at the time of registration were enrolled in this meta-analysis. The intervention group took HCQ or CQ orally. The control group was not blinded by quinine or placebo. Pooled relative risk (RR) of SARS-CoV-2 infection, mortality, hospitalization, adverse events, and compliance were calculated. The software tools utilized for statistical analyses were Stata 14 and Review Manager 5.3.
>Results: A total of 9 studies including 7,825 participants were enrolled. Bias of individual studies were assessed as low risk. The pooled RR for SARS-CoV-2 infection was 0.75 [95% confidence interval (CI): 0.68-0.83] (z=-4.01, P<0.0001; I2=11%). The pooled RR for hospitalization was 0.72 (95% CI: 0.35-1.50) (z=0.87, P=0.39; I2=0.0%). The pooled RR for mortality and adverse events were 3.26 (95% CI: 0.13-79.74) (z=0.72, P=0.47; I2=0.0%) and 1.90 (95% CI: 1.20-3.02) (z=2.73, P=0.0063; I2=94%).
>Conclusions: Results of this meta-analysis indicated significant impact of HCQ on SARS-CoV-2 infection with higher risk of adverse events. These findings must be considered with caution, and further research is necessary to delineate the specific circumstances where HCQ may be effective for COVID-19 prevention.
The full text of the study can be found here: [18]
This study also discovered no benefits. [19]
>‘We have concluded that there is no beneficial effect of hydroxychloroquine in patients hospitalised with COVID-19. We have therefore decided to stop enrolling participants to the hydroxychloroquine arm of the RECOVERY trial with immediate effect. We are now releasing the preliminary results as they have important implications for patient care and public health.
>‘A total of 1542 patients were randomised to hydroxychloroquine and compared with 3132 patients randomised to usual care alone. There was no significant difference in the primary endpoint of 28-day mortality (25.7% hydroxychloroquine vs. 23.5% usual care; hazard ratio 1.11 [95% confidence interval 0.98-1.26]; p=0.10). There was also no evidence of beneficial effects on hospital stay duration or other outcomes.
This study found no benefits, but did identify an increased risk of adverse effects: [20]
>COVID-19 has quickly become a public health problem worldwide, and treatment for this new disease is needed. Hydroxychloroquine is an antimalarial that in vitro studies have shown action against SARS-CoV-2, which is why it has been the target of clinical studies with conflicting results. Therefore, the aim of this systematic review was to assess the association of hydroxychloroquine use with the virological cure, clinical recovery, mortality, and development of adverse effects in patients with COVID-19. PubMed, Cochrane Library, and Lilacs were searched until 7 January 2021, for randomized clinical trials with COVID-19 patients treated with hydroxychloroquine or chloroquine. Of the 130 studies found, 12 met the inclusion criteria. Compared to the patient’s control group, the risk ratio (RR) for the virological cure and clinical recovery with hydroxychloroquine or chloroquine use was 1.04 (95%CI 0.91–1.17) and 1.03 (95%CI 0.92–1.13), respectively. Hydroxychloroquine (with or without azithromycin) was also not associated with mortality (RR = 1.09, 95%CI 0.98–1.20). Treatment with hydroxychloroquine was associated with any adverse effects (RR = 1.50, 95%CI 1.18–1.81). Hydroxychloroquine or chloroquine use did not have a significant effect on virological cure, the time of clinical recovery, and improvement in survival in COVID-19 patients. However, patients who used hydroxychloroquine showed an increase in adverse effects.
This study also found no benefits: [21]
>Methods: We conducted a multicenter, randomized, open-label, three-group, controlled trial involving hospitalized patients with suspected or confirmed Covid-19 who were receiving either no supplemental oxygen or a maximum of 4 liters per minute of supplemental oxygen. Patients were randomly assigned in a 1:1:1 ratio to receive standard care, standard care plus hydroxychloroquine at a dose of 400 mg twice daily, or standard care plus hydroxychloroquine at a dose of 400 mg twice daily plus azithromycin at a dose of 500 mg once daily for 7 days. The primary outcome was clinical status at 15 days as assessed with the use of a seven-level ordinal scale (with levels ranging from one to seven and higher scores indicating a worse condition) in the modified intention-to-treat population (patients with a confirmed diagnosis of Covid-19). Safety was also assessed.
>Results: A total of 667 patients underwent randomization; 504 patients had confirmed Covid-19 and were included in the modified intention-to-treat analysis. As compared with standard care, the proportional odds of having a higher score on the seven-point ordinal scale at 15 days was not affected by either hydroxychloroquine alone (odds ratio, 1.21; 95% confidence interval [CI], 0.69 to 2.11; P = 1.00) or hydroxychloroquine plus azithromycin (odds ratio, 0.99; 95% CI, 0.57 to 1.73; P = 1.00). Prolongation of the corrected QT interval and elevation of liver-enzyme levels were more frequent in patients receiving hydroxychloroquine, alone or with azithromycin, than in those who were not receiving either agent.
>Conclusions: Among patients hospitalized with mild-to-moderate Covid-19, the use of hydroxychloroquine, alone or with azithromycin, did not improve clinical status at 15 days as compared with standard care. (Funded by the Coalition Covid-19 Brazil and EMS Pharma; ClinicalTrials.gov number, NCT04322123.).
As did this one: [22]
>Objective: To investigate whether hydroxychloroquine could reduce COVID-19 severity in adult outpatients.
>Design: Randomized, double-blind, placebo-controlled trial conducted from 22 March through 20 May 2020. (ClinicalTrials.gov: NCT04308668).
>Setting: Internet-based trial across the United States and Canada (40 states and 3 provinces).
>Participants: Symptomatic, nonhospitalized adults with laboratory-confirmed COVID-19 or probable COVID-19 and high-risk exposure within 4 days of symptom onset.
>Intervention: Oral hydroxychloroquine (800 mg once, followed by 600 mg in 6 to 8 hours, then 600 mg daily for 4 more days) or masked placebo.
>Measurements: Symptoms and severity at baseline and then at days 3, 5, 10, and 14 using a 10-point visual analogue scale. The primary end point was change in overall symptom severity over 14 days.
>Results: Of 491 patients randomly assigned to a group, 423 contributed primary end point data. Of these, 341 (81%) had laboratory-confirmed infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or epidemiologically linked exposure to a person with laboratory-confirmed infection; 56% (236 of 423) were enrolled within 1 day of symptoms starting. Change in symptom severity over 14 days did not differ between the hydroxychloroquine and placebo groups (difference in symptom severity: relative, 12%; absolute, -0.27 point [95% CI, -0.61 to 0.07 point]; P = 0.117). At 14 days, 24% (49 of 201) of participants receiving hydroxychloroquine had ongoing symptoms compared with 30% (59 of 194) receiving placebo (P = 0.21). Medication adverse effects occurred in 43% (92 of 212) of participants receiving hydroxychloroquine versus 22% (46 of 211) receiving placebo (P < 0.001). With placebo, 10 hospitalizations occurred (2 non-COVID-19-related), including 1 hospitalized death. With hydroxychloroquine, 4 hospitalizations occurred plus 1 nonhospitalized death (P = 0.29).
End of quoting studies
That tracking chip claim is very rare. We have to realize that for any conspiracy topic, some people will come up with highly "out there" theories. These might still have merit, but honest media outlets should use the strongest, most popular and developed theories as examples. The usual conspiracy theory in terms of the vaccines is that they've been designed to hurt and / or kill people. It's the one stated by experts like Michael Yeadon, Sherri Tenpenny and Shankara Chetty. I've collected plenty of evidence for it, too.
Yet you cite bizarre conspiracies that are just as dumb as the tracking chip claim, like nanomachines. It is as I said, conspiracists tend to lack self-awareness and falsely view themselves as being rational compared to other conspiracists. At best, your views can only be less dumb. You also commited the appeal to authority I brought up earlier. These people you're speaking of are wrong, and are hardly experts.
The most qualified of them all is Michael Yeadon, the other two are random physicians.
That article interviewing Yeadon made a bunch of claims about "mass depopulation": [23]
>“That’s what I would do if I wanted to get rid of 90 or 95% of the world’s population. And I think that’s what they’re doing.”
Didn't happen though, did it?
Tenpenny made a bunch of baseless claims citing supposed studies without naming them in that article interviewing her, while also fearmongering about mass death a great deal, which of course never came to be. She also doesn't seem to know that you can patent natural things. [24]
>the NIH is now fighting with Moderna over patent rights because you can’t patent anything that’s out in nature
Companies have patented seeds.
Chetty also fearmongered about mass death, which never came to be. [25]
>“If I had to give you my opinion, as to what is happening on a global scale,” he said, “[the] spike protein is one of the most contrived toxins or poisons that man has ever made. And the aim of this toxin is to kill billions without anyone noticing it. So, it’s a poison with an agenda.”
More fearmongering about mass death which never came to be.
Every last one of these people was wrong. I have fairly comprehensive evidence refuting claims of vaccines killing people, which comes up in the refutation of your COVID article.
About the latter two claims, I've literally never heard of them - and I've done hundreds of hours of research for my Corona report. Usually people say that masks just don't work. Of course, the best supported conspiracy theories are completely missed in this article - such as faking the case and death statistics. Those conspiracies about statistics are not missed, you can find articles discussing them online if you look for them.
For someone who did hundreds of hours of research, you sure made a very poorly founded case.
Let's now see how the shills handle moon landing conspiracy theories.
This is where you completely abandon the entire façade of rational, scientific thought.
First of all, what's the strongest argument for the moon landing being a hoax? From Debunking Skeptics:
>1. NASA's inability to send men to the moon today means they could not have in 1969
>The strongest argument here is that if NASA can't go to the moon today after 40 years of technological advancements, then it certainly couldn't have in 1969, plain and simple.
Boom. Easy, and kills the entire moon myth in one sentence (but please read the entire argument).
In my opinion, the foundations of moon hoax shouldn't be the photo analysis arguments; they are just too dependent on interpretation most of the time, and require skill in the relevant discipline. On the other hand, argument number #1 is easily understandable by even children, and irrefutable
i.e In my opinion, the foundations of the Moon hoax argument should not be based upon empirical evidence, but should instead be based upon personal rhetoric, so that one can disqualify evidence they're unable to comprehend.
You have just betrayed everything that you've been crusading for so melodramatically. Your solution, in order to refute dissent, is to employ rhetorical tricks to discredit evidence that contradicts your belief.
People should not focus on empirical evidence, they should focus on personal rhetoric. That's the essence of what you're saying here. This isn't scientific, nor is it rational.
If it's simple and irrefutable then it's probably unfalsifiable, in which case, it probably doesn't have any bearing on our lives. It's a baseless tautology. It's akin to saying "God caused this thing". We can't test it. We can't refute it. So it's immaterial. It has little bearing on our lives.
You're now the one who is committing "dirty tricks".
The point you brought up is not irrefutable, as you say it is. The issue comes down to FUNDING. This is a widely known reason why the Moon missions ceased. The government stopped funding it. It was super expensive, there was no profit to be made off of it that could reimburse the enormous costs of it, and the money could be used to address material concerns back on earth. If you researched the Moon landing, you would know this. If the media doesn't bring this up in every single article, so that you're not able to cherrypick news articles and make it seem like there's a conspiracy afoot, it's probably for that very reason. Most sane people won't consider this argument, because they've already subconsciously dealt with it, or seen it somewhere else. Type the phrase "why did nasa stop going to the moon" into just about any search engine. It will yield you the explanation I just gave. Here's four articles that I found within a few minutes which explain why the missions ended.[26][27][28][29]
It is quite literally just a baseless assertion. But, don't worry, I'll be going over Winston Wu's article and refuting his supposed scientific evidence.
None of the "why do people still believe moon landing conspiracy theories?" turds the media shits out every so often bother to touch this argument. That alone should make you question their honesty.
Probably because most sane people would never even come up with such a stupid argument. The media not having an encyclopedic knowledge of Moon landing conspiracy theorist arguments ought to make you question their integrity, not how they handle things like the Gaza genocide or the Epstein coverup.
What do they mention? The "There aren't any stars in the background" argument which Debunking Skeptics says explicitly not to use. "The Moon landing is fake because Stanley Kubrick filmed it". Wow! No one actually says this. First we prove it's a fake, then some people try to find out who's responsible - but it's not relevant to proving the fakery itself. Maybe we will never know who did it, but the hoax evidence will still stand on its own. The "The American flags appear to "flap" in the breeze", for which the excuse that it was physically moved is given. But they won't show you the actual footage so you can judge for yourself if their explanation works:
You are either bad at searching for evidence, were fooled into not bothering to search for evidence, or you are willfully ignorant.
The documentary called "For All Mankind" has the full clip. You can watch it on YouTube, although I would not recommend this, as the version on YouTube is not HD. I torrented an HD version of the documentary. It's on thepiratebay. The YouTube versions can be found here.[30][31]
This documentary is one of the most famous Moon landing documentaries. Recommendation lists of Moon landing documentaries regularly place it toward the top. If you searched for documentaries with footage, you'd have found it almost immediately. You can also just look for full clips of the scene on YouTube. They exist.
This is another trope of the conspiracist: willfull ignorance. They act as if "they" won't show you the full footage, because the conspiracists literally know next to nothing about what they're discussing, and have not engaged in the topic in good faith. You have to spoonfeed them knowledge, to get them to reconsider their opinion. They won't make the effort to test their own opinion.
Here is a longer clip with 169 million views on YouTube.[32] I searched "moon landing flag scene". It was on the first page. This is indefensible.
The fact of the matter is you probably don't know the first thing about the Apollo missions, because you only researched them through conspiracy theorists like Winston Wu. It is in fact you who is the member of a cult of dogma, not others. You sit there, and absorb flimsy rhetorical arguments in favor of the Moon landing having been faked, and don't put any effort into actually seeking out differing perspectives. While doing this, you pretend that other more-knowledgeable people are doing the same. They're not.
Other covered arguments like "No Crater at Landing Site" and "The "C" rock" are - again - minor ones. Though even the C rock is portrayed weakly because it doesn't mention the C on the ground. In my opinion, the foundations of Moon hoax shouldn't be the photo analysis arguments; they are just too dependent on interpretation most of the time, and require skill in the relevant discipline. On the other hand, argument number #1 is easily understandable by even children, and irrefutable. Yet the mainstream always focuses on the photo analysis because they can whip out a mildly believable excuse and prevent you from digging deeper. But hey, if the conspiracy deniers love the photo analysis arguments so much, why don't they touch this one? Literally proving there to be an artificial light in the photos. Another strong argument that's completely ignored are the deaths of Apollo One astronauts.
It's a shame that Winston Wu's website is now cloudflared. It makes my task more time-consuming. Anyway, I'll be going over these arguments. Wu's article is a textbook case of gish galloping.
If our ideas are as stupid, as insane, as easily dismissible as they claim - they should be happy to embarrass us on the big stage. Actually, the conspiracy deniers have already proven they do not mind butting heads with their opponents if they perceive them as weak - as shown with the avalanche of many hours long debates with flat Earthers available on YouTube
This is a very romantic view of yours. You assume that people who are wrong will regularly admit this, whether it be the purveyor of a conspiracy theory, or the people who listen to that purveyor. This isn't what happens in reality. Your example of "many hours long debates with flat Earthers" is a testament to this fact. Flat earthers are wrong on every level, and routinely get destroyed by people who know what they're talking about. But do they change their minds? No. There's no meaningful correlation between the level of debate had with them and the frequency of people wisening up. It's almost as if debate doesn't change people's minds and only legitimizes fools.
These people are personally invested in their ideology. They derive pleasure from being special, lone geniuses who have discovered the truth that everyone else has missed.
Conspiracists often find the lone genius trope very appealing. Most "experts" who validate, or outright seed the conspiracists' beliefs posture themselves as lone geniuses, as people who stand alone in some field, trying to spread the truth they've discovered, suppressed by the myopic establishment.
Digdeeper has already shown his interest in this trope with his whinging about Semmelweis and Copernicus.
Those debaters are not prominent scientists. RFK is a worm-operated Manchurian candidate, he knows nothing of what he speaks. The sort of debates that you're probably thinking of are not even debates to begin with. They're verbal debates. They're popularity contests. An hour-long debate made up of five minute increments where one person says one thing and the other person says some other things. The debate ends, the audience (who probably aren't educated much on the topic of the debate) goes home, and decide for themselves who won. The winner is the guy who sounds the smartest, which often is determined by how eloquently you can speak and not the validity of your ideas. The contestants are merely debating in favor of convincing an audience of their ideas. This does not speak to the veracity of what they are arguing in favor of. It's analogous to arguing in a court of law, only less valuable, because at least in a court of law, a judge or jury make an authoritative ruling which has material consequences. In these debates, nothing happens after they're over. Also, just to mention, some conspiracists actually cite the opinions of dimwitted judges and jurors as evidence of vaccines being harmful.
It's a spectacle. It's public entertainment. A real debate is two or more experts in a field holding long-form, civil discussion with one another, like by corresponding via mail, or holding a series of meetings. That's where you find the real answers. That's the sort of debate that produces actual changes in the world, by influencing how people study and practice scientific fields.
You make it seem as though two random people having an argument over a certain subject is the be all end all of that subject. That's nonsense. It isn't. Scientific discourse is where it counts, not two public figures chattering on a podcast, one of them having been hijacked by a worm, all while some CTE-blunted ex-kickboxer acts as the judge. What a joke.
This next section brings to mind the callousness of many conspiracists, in how they are unable to reckon with the logical conclusions of their ideas, such as the white genocide hoax. These ideas they promulgate end up encouraging people to take violent action against innocents. By acknowledging the reality of an atrocity of that kind, they are implicitly acknowledging that their ideas do promote violence, because there are countless other atrocities linked to their ideas that will have predated that one. There will be a pattern of behavior to be seen amongst them and their rhetoric. As a result, all they can do is deny the reality of these atrocities in order to attempt to shield themselves from the truth of what they are and what they support. Collective groups do not want to think of themselves as fundamentally bad people.
In all fairness, they themselves are not the only ones responsible in causing things like the white genocide hoax to result in mass murders. The government is also complicit in this, by not addressing the material concerns people have which cause them to rationalize their plight in society with conspiracies such as white genocide. The American government, in its current form, is never going to fully interrogate this matter, which will leave these hanging mysteries, which can be elucidated with lies such as white genocide, which in turn will cause some to commit mass murder. The government does not care, because it is merely a vessel for capitalist tyrants to extract wealth from the masses.
If you can't refute, dismiss, or devalue it in any way - just pretend it doesn't exist. This has actually been done for a very long time, but went up to eleven during corona. I will show you a simple example right now. Here are the Google (Startpage lifts Google results) and Bing (Qwant lifts Bing results) search results, side-by-side for the query "Christchurch shooting was faked":
Let's analyze the Google results one by one:
>EU vs Disinfo. Just the name already sets us up for what's coming. From their About page: "Using data analysis and media monitoring services in 15 languages, EUvsDisinfo identifies, compiles, and exposes disinformation cases originating in pro-Kremlin media that are spread across the EU and Eastern Partnership countries." [...] "Our team is also heavily involved in public and government outreach. We brief and train EU institutions, Member State governments, journalists, and civil society organisations, and regularly speak at international conferences". So, it's a website dedicated to hunting down the so-called "Russian disinformation" and training governments to do the same. Of course - as the anti-"disinformation" site - it dismisses the notion that the Christchurch shooting was faked. All we have learned about the alternative views is that they are "disinformation".
The Sydney Morning Herald. From Encyclopedia Britannica: "The Sydney Morning Herald, daily newspaper published in Sydney, Australia's oldest and one of its most influential papers". We wouldn't expect this mainstream paper to challenge mainstream narratives, and of course it doesn't. In fact, the entire piece is focused on mocking and dismissing conspiracy theories, and uses many of the tricks listed here (couldn't pass the chance to execute the standard flat Earth / Qanon smear). We still haven't learned what the conspiracy theorists actually think.
The Independent. Whining about the white genocide theory and salivating over more censorship for "racists". The so-called "Independent" refuses to do an independent investigation into anything. Next.
Combating Terrorism Center. It should be obvious we're not going to find what we want there from the name alone, and that's exactly what happens. Ctrl+f for "faked" or "staged" brings 0 results. I did not want to read another shady piece whining about "conspiracy theorists" and trying desperately to associate them with terrorism. I wanted to learn whether the Christchurch shooting was faked (my exact query!), and I couldn't find that out at the anti-terrorism center. Actually, the article isn't even about this specific attack at all, but some other - so Google totally ignored the user's wishes here in order to push a general narrative.
Buzzfeed News. Heh, this one is really funny. Check this quote: "and even the reliably vocal conspiracy theorists aren’t touting the usual “this shooting was staged by the government” fake". Actually, we are :D. Obviously, there is no analysis of that theory here.
Now, I am not here to tell you what happened or didn't happen at Christchurch, nor what the implications are, etc. I am not convinced of any particular version myself (though I realize the official story is full of holes). That's something you will have to investigate for yourself. The point is, Bing lets you do that, and Google does not.
If you do not have an opinion on the Christchurch mass shooting or its implications then you shouldn't be weighing in on whether or not search engines ought to be listing bizarre conspiracy theories which deny the reality of the shooting. A white supremacist stormed a mosque and Islamic center, murdering 51 innocent people, the initial attack being livestreamed, recordings of which are easily discoverable online — as if you needed any more proof that it happened.
You essentially feel that these platforms should have a near absolutist philosophy when it comes to the freedom of information.
You feel that all ideas should be considered equally. But not all ideas are equal. Treating them as such can be harmful to society. In this case, it would be by delegitimizing the very real threat of right-wing extremism, which will simply allow right-wing terrorists to run rampant. And this has been the consequence. They are only becoming more and more emboldened. Now, the Trump government, a right-wing fascist regime, has simply decided to delete the statistics proving right wingers to be exceptionally violent. Do you go writing about this on your website, an actual conspiracy to suppress information? No. Of course not. Because the real problems get sidelined in favor of the fake ones. Because all of this stuff is really just a game to you. Real conspiracies make a passing mention on your website, much like with conspiracy theorists in general.
One reason why conspiracy theorists don't focus on real conspiracies is because they perceive them as being oversaturated. Conspiracy theorists tend to be contrarians and hipsters. They want to focus on the truth that nobody else knows or cares about. Other conspiracies are studied by historians and journalists, or people operating as historians/journalists who didn't necessarily obtain some degree or certification in those fields. They are focused upon and researched by hundreds, thousands, even tens of thousands of individuals, and the stories frequently receive the attention of millions. They tend to have some degree of publishing in the mainstream, through some specific media organizations. The conspiracies are quite well understood, but people do still uncover new information as time goes on. They become a body of work that people contribute to, even decades later. This repulses the conspiracist. They can't be the special guy who has uncovered the truth that nobody else has caught onto yet. They're just a contributor in a body of work, like most scientists are. Every once in a while you might have a significant, general contributor, but they're rare, and perhaps the conspiracists don't have what it takes to be like that.
As I said, they wish to be the lone genius. In this particular community, it in part explains the worship of figures like Ted Kaczynski and Terry Davis to me.
To address the Winston Wu article on the Moon landing...
Winston Wu's article that you linked which "debunks" the Moon landing is rife with flawed logic and false information. The first and "strongest" argument, as you view it, is a solid example
Let's now see how the shills handle moon landing conspiracy theories. First of all, what's the strongest argument for the moon landing being a hoax? From Debunking Skeptics:
>1. NASA's inability to send men to the moon today means they could not have in 1969
>The strongest argument here is that if NASA can't go to the moon today after 40 years of technological advancements, then it certainly couldn't have in 1969, plain and simple.
Boom. Easy, and kills the entire moon myth in one sentence (but please read the entire argument).
This is not a sound logical argument. A logical leap is being made. Just because NASA cannot send humans to the Moon today (they actually are working on another manned mission to the Moon called Artemis III, though I doubt it'll manifest in this political environment) but did decades ago does not mean that they never went. No consideration is being made as to why they may not have sent humans again. That is illogical. As an example: Say that I went on a trip to Tibet five years ago, but now I say that I cannot go. Does this mean that I never went to Tibet? All of the photographs I took while I was there are fake? No, not necessarily. Maybe I don't have enough money to go back to Tibet right now. Maybe I do not feel the need to return. And then we can consider the plausibility of that.
In the case of NASA, it is freely admitted that they stopped sending missions to the Moon because it was becoming too expensive. The whole series of missions cost hundreds of billions of dollars — a fact that is mentioned in your article. The White House did not want to fund it any longer, as there were material concerns back on earth that the money could address. This is an easily discoverable explanation. Simply searching "why did nasa stop going to the moon" yields countless results.[26][27][28][29][35]
If they've already sent six manned missions to the Moon and gathered all of these materials from the Moon, why send more manned missions? When they are capable of sending robots instead, which is safer and cheaper, why not do that? Well, there is no reason to not do that. It is merely a conceited, childish enthusiasm you have, a romantic idea of humans colonizing the Moon, that humans simply must continue traveling to and from the Moon, that it can't just be robots. Sending humans regularly is prohibitively expensive. It's simply not realistic. It may never be realistic for humans to colonize space. We'll see. Either way, we have bigger fish to fry here on earth. Every year tens of millions of people in the developing world die of preventable causes due to the economic policies of the West. That's something to start with.
Real engineers worked on real projects, like designing the lunar module, or spacesuits, or the rockets themselves. Real in the sense that they worked on an actual spacecraft, or an actual spacesuit that was physically created and existed. These real projects that they worked on were developed with use of data which had to come from somewhere. Assuming that NASA truly had sent prior spacecraft into space, then the data they received (which they used to design future spacecraft) was real and came from outer-space. If they never went to space, then it was made up. In which case, the spacecraft they made would likely malfunction or break apart. For the conspirators, as long as their clueless puppets, the engineers, did not witness the spacecraft break apart, then there would be no issues I guess. But people monitored their flight. So, where exactly did they pull their con?
Then comes the question of why and how they would fake the data. Who even is "they"? Some secret group within NASA, deceiving the rest of the workers at NASA? Rockets were sent into space. People watched it happen. Manned and unmanned missions were sent to the Moon and back, without landing there, in order to retrieve data. Photographs were taken. Measurements were made. These missions either were faked and that was kept a complete secret, or they happened. Somehow this has all been kept a secret until this very day.
Or those events were real. But if they were real, then why fake the Moon landing? Why do that if you have demonstrably sent things to space and to the Moon? It becomes illogical.
Hundreds of billions of dollars were spent on the Moon landing. Hundreds of thousands of people worked on the lunar missions. Enough blueprints and documents to fill up entire buildings had to be created during the process of developing the spacecraft. All of these computers and human calculators were needed. People watched the astronauts get into the spacecraft. The spacecraft was launched in a public display that was highly televised. A million people physically watched the Apollo 11 rocket launch off into space. People, including journalists, had watched the astronauts walk into the rocket-ship. Bystanders in certain parts of the globe could literally see it in the atmosphere. Bystanders were able to verify radio transmissions as coming from space. Some of the Moon missions were actually recorded by the astronauts from inside the rocket. You can watch the videos in a documentary called "For All of Mankind", which is a documentary made from real footage from the Moon missions. In the documentary you can watch astronauts swallowing floating blobs of liquid and tossing flashlights back and forth to one another at zero gravity. All of that footage had to have been staged in an era when that was probably not possible using special effects.
To this very day, nuclear-armed superpowers like India and China, sovereign from the United States Government, have independently confirmed the existence of the Moon landings with robots they've sent to the Moon. South Korea and Japan have also verified the landings. Although they are allies to America, they further increase the scope of the conspiracy.[36][37][38]
Radio observatories independently surveyed the lunar missions, such as the Bochum Radio Observatory,[39] and the Arcetri Observatory which surveyed the Apollo 11 mission.[40]
These webpages catalog several independent astronomical observations of lunar missions, in Spain, France, America, Canada, Britain, New Zealand, and Ireland. There is also eyewitness testimony, such as from pilots in the Pacific Ocean who saw spacecraft exiting and entering earth.[41][42]
These reports affirm that crewed-spacecraft were sent into space, and telemetered data from the Moon.
Some guy named Larry Bassinger from Kentucky also surveyed the Apollo 11 mission.[43]
Hundreds of kilograms of Moon rocks were taken during the Apollo missions. These rocks have a unique a geochemistry and isotopic signatures that do not match those of Earth or bodies like meteorites. These rocks have been studied by many international scientists over the decades. Everyone who has studied them has to have somehow been deceived or must be a conspirator themself.
Notably, in 1971 the Soviet Union was given Moon soil from the Apollo 11 and 12 missions to examine.[44] Of anyone in the world, they probably had the greatest incentive to prove that the Moon landings were a hoax.
Retroreflectors placed on the lunar surface by Apollo are still used for laser-ranging experiments by independent labs, demonstrating objects to on the Moon where they are claimed to be. This also has to be fake, or, instead, they were placed there, but not by humans, meaning you're entertaining the possibility of humans being able to send spacecraft to the Moon.
You have to address these serious holes in your narrative. You are asserting that countless people are conspiring in an intergenerational, international conspiracy to hoax the Moon landings. At this point, hundreds of thousands of people could be directly involved, not just indirectly involved by working on something like a spacesuit or lunar module.
If all of the work to send men to the Moon was put in, then why not go there? Physics-related scientists do not look back upon the schematics of the Moon landing and realize, thanks to some new information they have from our more recent spacecraft, that the Moon landings were physically impossible. It is not as though some new information has become known to us in this modern era that would demonstrate that the Moon landings could not have possibly happened. Everything has held up, because the work that was put in was based in reality. Given that fact, it simply makes no sense to fake the Moon landing at that point.
Do you not believe that they ever made anything? Do you believe that hundreds of thousands of people secretly sat around and twiddled their thumbs? To what degree do you believe that the Moon landings were faked?
Comparing the Moon landings to conspiracies that were revealed to the masses is a non-starter. We'll get into that later.
Let's begin with Wu's article now.
"The bigger the lie, the easier it will be believed." - Adolf Hitler
This isn't a real quote, by the way. But, it sets the tone for an idiotic conspiracy article from the 2000s written by a dumb American.
1. NASA?s inability to send men to the moon today means they could not have in 1969
Let?s start with the strongest argument. First, here are some shocking facts that will leave you scratching your head:
Every major technological accomplishment in history has been repeated well under forty years, all except one. Within forty years of Christopher Columbus setting foot in America in 1492, thousands of other Europeans had done the same. Within forty years of the Wright Brothers flight across the Atlantic Ocean in 1903, thousands of other people had done the same. Within forty years of Sir Edmond Hillary reaching the summit of Mount Everest in 1953, thousands of other explorers had done the same. And within forty years of Yuri Gagarin?s orbit of the earth in 1961, many others had done the same. Yet forty years after 12 men allegedly set foot on the moon in 1969-72, not a single person or country has done it, nor attempted to do so (including the Russians who were ahead of us in the space race). Does this not seem highly strange and illogical?
It does not seem strange or "illogical" to me. Wu isn't thinking of the sheer scale of what is being done here, nor is he considering the context of these situations. It took the most powerful government on earth years of painstaking work to put people on the Moon. It cost hundreds of billions of dollars, years of time, and required countless people, and required grueling training for the astronauts.
If you want to sail across the ocean, comparatively speaking, it's not nearly as hard. As long as you know how to navigate the seas, which people back then knew, you build a ship, load up your provisions, and sail away. Then once you've got a route that you've charted, you repeat the journey. The only expense is in building ships and getting provisions, which isn't nearly as complicated or costly as designing and launching spacecraft.
It shouldn't be a surprise that there were hundreds to thousands of Europeans in the Americas within decades of Columbus reaching the Americas. The Americas are not the Moon. Nor is the ocean outer space, or the Moon. There are fish in the ocean, which you can eat. You can collect water while on the ocean to drink. In the Americas, there's food and water. It's earth. There's an atmosphere. There's not cosmic radiation. There's not low gravity, which causes muscle atrophy and bone decay. There's not high-velocity dust which can damage structures, depressurize them, and result in immediate death.
Sailing a ship is also quite different from launching a man in a rocket to the Moon, if you could imagine that. Your ship isn't just going to suddenly explode as soon as you try to set sail. If it does begin to sink, you won't just die immediately, you can bail, with smaller boats. It's quite different, if you could believe that. The same is true for going to Everest and for flying planes. Something to bear in mind though is that all of these processes, with sailing the world, and using aircraft, did take time to advance. For ships, it took generations. Planes advanced quicker than ships.
The analogy with Everest is not even historically accurate. Humans had been exploring Everest for over a century. It took until the 1950s for people to summit Everest successfully. It wasn't just 40 years. Attempts dedicated to summiting began in the 1910s. Once people got to the top, travel to and from normalized, but again, Everest is not the Moon.
And when it came to traversing the Atlantic Ocean, Spain was economically prepared to commit to regular travel to and from India for trade. Humans were not prepared to be traveling to and from the Moon with regularity or colonizing it. Humans were prepared for a series of missions. They would weigh the benefits of them against the cost. Eventually, it became too costly to continue justifying.
The Moon landings were what they were: landings. A first step in the mission to colonize space. We're far from being able to colonize space at this time, and frankly, it seems like a gratuitous effort considering all of the problems here on earth that we could focus our attention on.
These situations are not comparable in the slightest. This is an argument from incredulity that says nothing about an objective reality. It's simply absurd, and anyone who finds this compelling may sadly be too delusional and uneducated to reason with. Let's hope not.
? FACT: Since the Apollo Moon Missions in 1969-72, which sent astronauts 240,000 miles to the moon and back six times, no one has ever gone higher than 400 miles above the Earth. Even the Space Shuttle missions have gone below that, remaining well under 400 miles.
Well, what is there to send people towards in between these two increments? It's a bunch of dead space. Why would you send an astronaut 10,000 miles out into dead space, as opposed to a couple hundred, which is much closer to earth.
Either way, this is no longer true. The Polaris Dawn mission launched in 2024 reached an apogee of 1,400 kilometers or about 870 miles. There haven't been crewed missions since Apollo and Polaris Dawn which have done this, that's true. And it's because they would be pointless — much like Polaris Dawn was. There were a bunch of crewed missions before then which went very high. Those were intended to collect data. By the time of the missions, they had their data.
? FACT: So far, 14 astronauts have died in Space Shuttle missions that went 200 miles above the Earth, yet during the Apollo program NASA allegedly sent astronauts 240,000 miles to the moon and back six times, with no loss of life at all? In other words: 200 miles = 14 casualties, 240,000 miles = 0 casualties. Does that seem odd? Would you buy that? Can you fathom the enormous difference between 200 and 240,000 and how big of a stretch that is?
This claim of 14 astronauts having died in missions that went 200 miles above earth is not sourced. I looked into it.
It is true that 14 people have died in space shuttle missions. The Challenger in 1986 killed 7 people, and Columbia in 2003 killed 7. The Challenger only made it 14 kilometers high.[46]
Columbia did make it to space, the highest they went was 177 miles. They died on re-entry when the shuttle broke apart. It was because a piece of the spacecraft broke off during the initial launch and struck a section of the aircraft, compromising it. The compromise later caused the craft to break apart during re-entry.[47]
How many people have actually died in missions that went 200 miles above the earth? An article from Sky at Night Magazine explores this question.[48]
>If we take the question in its most literal sense, and assume 'space' to begin at the Kármán line, 80-100km (50-60 miles) above Earth’s surface, then the only three deaths ever recorded were those of Russian cosmonauts Georgy Dobrovolsky, Victor Patsayev and Vladislav Volkov.
>On 30 June 1971, the three-person crew of Soyuz 11 were returning to Earth after successfully completing a 22-day sojourn on Salyut 1, the world’s first space station, when a faulty valve caused their descent module to depressurise shortly before re-entry.
>The capsule touched back down to Earth in Kazakhstan as planned, but when it was opened all three cosmonauts were found dead.
>But many more astronauts have died during spaceflight.
>The first was Russian cosmonaut Valdimir Komarov, who died on 24 April 1967 during the first crewed test flight of the Soyuz 1 rocket, when the parachute on his descent module failed.
>November that same year would see the death of US pilot Michael J Adams.
>He was conducting a test flight of an X-15 space plane (a joint NASA/USAF mission) when the craft went into an uncontrolled spin and disintegrated at an altitude of 19.8km (65,000 ft).
>Perhaps the most well-known space-related deaths, however, occurred on 28 January 1986, when the space shuttle Challenger disintegrated shortly after takeoff, following the failure of a booster rocket.
>The seven crew members onboard – Gregory Jarvis, Christa McAuliffe, Ronald McNair, Ellison Onizuka, Judith Resnik, Michael J Smith and Dick Scobee – were all killed instantly.
>Almost exactly 17 years later, on 1 February 2003, disaster would strike the Space Shuttle programme once more, when the Shuttle Columbia disintegrated on reentry, again killing all those onboard.
>The crewmembers were Rick D Husband, William C McCool, Michael P Anderson, David M Brown, Kalpana Chawla, Laurel Clark and Ilan Ramon. >That makes 22 people who’ve perished during flights that traversed the Kármán line at some point (or were meant to), regardless of their altitude at the time.
>If you include astronauts who perished during test flights, dry runs, training exercises and so on, then the list would have to include: >• Soviet cosmonaut Valentin Bondarenko, who perished when fire broke out in a low-pressure altitude chamber in 1961;
>• NASA’s Theodore Freeman (1964), Elliot See and Charles Bassett (1966), Clifton C Williams (1967) and Robert Henry Lawrence Jr (also 1967), and Roscosmos’s Sergei Vozovkikov (1993), all of whom died in plane crashes during astronaut training;
>• Michael Alsbury, who was killed during a test flight of Virgin Galactic’s SpaceShipTwo space plane on 31 October 2014;
>and of course most famously of all
>• Virgil ‘Gus’ Grissom, Ed White and Roger B Chafee, the three-man crew of NASA’s Apollo 1 mission, who died of asphyxiation on the launchpad at Cape Kennedy, after a fire broke out in the cabin during a launch rehearsal on 27 January 1967.
>Not including Michael J Adams, 21 in-flight fatalities is the figure generally quoted by NASA when the question of how many people have died in space crops up.
>As of 2025, around 680 people have travelled into space (according to the Fédération Aéronautique Internationale (FAI)’s definition), and 21 of them died as a result.
>That means a fatality rate of around 3%, or one death for every 33 flights.
So 21 people have died, but all of them died below 200 miles.
This is also listed under Wikipedia: [49]
>As of January 2025, 19 people have died during spaceflights that crossed, or were intended to cross, the boundary of space as defined by the United States (50 miles above sea level
>As of January 2025, there have been five incidents in which a spacecraft in flight suffered crew fatalities, killing a total of 15 astronauts and 4 cosmonauts
>As of December 2023, a total of 676 people have flown into space and 19 of them have died. This sets the current statistical fatality rate at 2.8 percent
>Spaceflight fatalities above the Kármán line
>Georgy Dobrovolsky
>Viktor Patsayev
>Vladislav Volkov
>Spaceflight fatalities below the Kármán line
>Vladimir Komarov
>Gregory Jarvis
>Christa McAuliffe
>Ronald McNair
>Ellison Onizuka
>Judith Resnik
>Michael J. Smith
>Dick Scobee
>Rick D. Husband
>William C. McCool
>Michael P. Anderson
>David M. Brown
>Kalpana Chawla
>Laurel Clark
>Ilan Ramon
>During training or testing
>Virgil "Gus" Grissom
>Ed White
>Roger B. Chaffee
This is 21 people.
Given this fact, Wu's claim isn't even true to begin with. Everyone who died had ascended less than 200 miles, not more than 200 miles.
? FACT: So far, 14 astronauts have died in Space Shuttle missions that went 200 miles above the Earth, yet during the Apollo program NASA allegedly sent astronauts 240,000 miles to the moon and back six times, with no loss of life at all? In other words: 200 miles = 14 casualties, 240,000 miles = 0 casualties. Does that seem odd? Would you buy that? Can you fathom the enormous difference between 200 and 240,000 and how big of a stretch that is?
When he says this, he doesn't factor into account just how many people have been into space in the first place. There have been 680 people as of the writing of the article I cited (there's been more now, and no fatalities), and only 21 died. 3% of them died. So, you have a 3% chance of death to begin with. That's not very high. If he had said that the overall rate of death was 3%, it wouldn't seem that significant to the reader.
But, one may rightfully ask, "How many people had been to space from 1961 to 2003? Surely that will change the probability of death to a meaningful degree?" Well, going off of this list from Wikipedia, from 1961 to 2003 there were 432 people who went to space.[50] Only 21 people destined to go to space (some made it to space, some did not) died. That's 4.86%. This is not even considering the fact that some of these space-travelers, including some who died, had been to space more than once. If you count multiple missions, which I can't be bothered to do because it's a waste of my time, the percentage can only decrease. The bulk of those people died in two incidents where there were shuttles with large amounts of people, that being 7 people each. This skews the results.
This chart from OWID lists 433 people from 1961-2003. So, the list on Wikipedia could be missing one person. This only works in my favor, of course.[51]
Since counting individual deaths does not give us an accurate idea of mortality, because there have been several missions where more than one person died, let's just count fatal missions.
Off of Wikipedia, if you count the individual missions leading up to Yang Liwei (the 432nd person, he came after the Columbia mission), there are seemingly 217 missions.
Now count the fatal missions. There are 5.
5/217 = 2.3%
So we have a 2.3% rate of fatality. This is even lower than the already low rate of fatality for individual persons.
If you count non-fatal missions that had to be aborted or failed, there will probably be a higher error rate. It depends on your definition of a failure. The thing is that the rate of error is going to be determined in part by the level of focus on the mission. A crude statistical value gives no qualitative insight into individual missions. These Moon landing missions had incredible amounts of focus dedicated to them, which would naturally lower the rate of failure. One of the Apollo missions, Apollo 13, failed and had to be aborted, which gives the overall missions a less than spotless record, and shows that they did have a rate of error.
I'm not going to steelman Winston Wu, so we'll move on.
Wu then argues from incredulity:
Can you fathom the enormous difference between 200 and 240,000 and how big of a stretch that is?
There are more hazards one may encounter during the first 200 miles of departing from earth than the remaining 240k miles to the Moon. Most of the journey to the Moon is going to be dead space, whereas the first 200 miles out of earth will entail launching successfully, not having a mid-air explosion or a crash, breaching the atmosphere, navigating radiation belts, and potential objects in earth's orbit, of which there are more objects one will encounter near to Earth than throughout the journey to the Moon.
Wu is also not considering the context of the missions. What were the people who died doing in space compared to the people who went to the Moon? Surely if they have different missions then they will perform different tasks under different circumstances and so may be facing different risks? Surely those people who died didn't have nearly as much focus put upon their missions as the moon landing missions, creating a greater risk of overlooked dangers? What were the dates of the incidents? Where were the dead astronauts from? What differences in technology were there? Wu doesn't consider any of this in his article. I have considered these things, having quoted them. These missions did not have the same levels of focus as the Apollo missions to send men to the moon.
The fact of the matter is that the contextual differences between those fatal missions and the lunar missions can explain why those men made it to the Moon and back alive. They had an incomprehensibly larger amount of resources and focus devoted to their missions than those other instances of death. There was absolutely a risk of death, but it wasn't that high to begin with. The true risk of death is not something one can quantify anyway.
If these don?tleave you scratching your head, then nothing will. What all this means is that inexplicably, NASA was able to send men 600 times farther in 1969 than it can today! How believable is that? Have you ever heard of technology going backward by such an extreme magnitude?! It?s totally illogical and nonsensical.
This whole talk of scale is meaningless when you aren't considering the actual environments. Exiting earth is much more dangerous than the remaining journey to the moon. I won't waste more space quoting the rest. He just gives more meaningless analogies.
He compounds this argument with the following claims:
Look at the implications here: Today, NASA does not have the technology to go higher than 400 miles above Earth, and has indirectly admitted it by their actions (in not doing so) and words. In a press release, NASA stated that the Van Allen Radiation Belts that surround the Earth are too dangerous to send humans through and is trying to figure out how to solve this problem. See here:
In a TV interview with journalist Sheena McDonald in 1994, NASA Administrator Dan Golden openly admitted that mankind cannot venture beyond Earth orbit until they can overcome the dangers of cosmic radiation. He managed to say this without any mention of the Apollo missions 25 years prior, which supposedly went 240,000 miles outside Earth orbit. This doesn?tmake any sense given that none of the astronauts on the six Apollo missions allegedly passed the radiation belts with no problem and no sickness.
Obviously, by this admission NASA has shot itself in the foot. Logic would ask, if they can't figure that out, then how did they get astronauts through it six times in 1969-1972 without any casualties or sickness from radiation?! It's a huge discrepancy - one of those obvious things right under your nose that you don't notice unless someone points it out to you. Yet amazingly most Americans are too gullible to notice when NASA shoots itself in the foot. This can only testify to how deeply ingrained the brainwashing of Americans must be.
Okay, so his claims are:
*NASA has implicitly stated (via their actions) that they do not have the technology to go 400 miles above the earth
This is false. NASA has sent robots more than 400 miles above earth since the Moon landings, demonstrating their possession of technology to go 400 miles above the earth. They also demonstrated their capacity to send humans beyond 400 miles by going to the Moon six times. Wu has yet to prove that this didn't happen.
*The Van Allen belts would have killed the crew
This is false. The particles in the Van Allen belt, protons, electrons, and alpha particles, can be adequately shielded against with several centimeters of metals like aluminium. Shielding was present in the aircraft. Additionally, only one Apollo crew ever passed through the inner belts, the rest of them missed the inner belts and passed through only the outer belts, and they did so at high speeds in order to minimize exposure.
The radiation from the belts is harmful, but it's not acutely harmful. You're not going to die immediately. The crews spent less than 2 hours passing through the belts. It's not healthy, but it won't kill you.
Animals were sent to space, some into the belts. They survived.
Fruit flies were sent to space, and have been until more recent times. They don't instantly die from the radiation. They survive.[52][53]
Mice were sent to space. They lived.[53][54]
Dogs were sent to space. They lived.[53][54]
Monkeys were sent to space. They also lived.[53][54]
Some of these animals were sent for the express purpose of studying the effects of radiation from the Van Allen belts, such as the Kosmos 110 mission by the Soviet Union launched in February of 1966, which sent dogs into the belts.[53][55]
I've frequently seen physicists online say that the dose of radiation from the Van Allen belts would be miniscule.[56]
>A satellite shielded by 3mm of aluminium in an elliptic orbit (200 by 20,000 miles (320 by 32,190km)) passing the radiation belts will receive about 2,500 rem (25Sv) per year. Almost all radiation will be received while passing the inner belt
So that's 25 Sieverts cumulatively, over the course of a whole year. One hour of this year-long exposure would amount to 2.86 milisieverts. For human exposure to radiation, the LD50 is 5 Sieverts of exposure in a short period of time. The astronauts were well below this threshold.
Let's look elsewhere for calculations of radiation doses. What better than Van Allen's own publications?[57][58]
>Observation of High Intensity Radiation by Satellites 1958 Alpha and Gamma
>The radiation intensity necessary just to blank the geiger tube is equivalent to 60 mr/hr. In this connection the recommended permissible dose for human beings is 0.3 r/week. The present radiation dose is 0.3 r in 5 hr or less.
This would be equal to 3 mSv, if I'm not mistaken. I'm not a physicist, I just looked it up and apparently it's 3mSv. That's a far cry from a lethal dose.
Let's see a later publication from Van Allen.[59]
>Our measurements show that the maximum radiation level as of 1958 is equivalent to between 10 and 100 roentgens per hour, depending on the still-undetermined proportion of protons to electrons. Since a human being exposed for two days to even 10 roentgens would have only an even chance of survival, the radiation belts obviously present an obstacle to space flight. Unless some practical way can be found to shield space-travlers against the effects of the radiation, manned space rockets can best take off through the radiation-free zone over the poles. 1 roentgen is 10 mSv. 100 roentgens is 1,000 mSv.
These values are not immediately lethal, but they also are outdated. Van Allen did not have a comprehensive knowledge of the belts at the time, nor did he pretend to. They hadn't yet considered the depth of the belt, the different fields of the belts and their respective levels of radiation. The results he had would be a warning of the high radiation levels, and prompted further study. They hadn't thoroughly experimented with shielding against the radiation yet. Quote:
>We are now planning a satellite flight that will test the efficacy of various methods of shielding
Let's look at a subsequent publication.[60][61]
In this paper, precise figures are not presented. I'm not a physicist. I can't and frankly am not willing to try and deduce a rough estimated dose by myself. From what I see online, it should be a couple dozen mSv per hour. Bear in mind, this is without the shielding that the astronauts had.
Here's another later paper.[62] Again, I'm not a physicist, so I can't make any authoritative statements here. From what I looked up online, supposedly this will amount to a couple dozen mSv per hour of absorbed radiation. This is without the shielding that the astronauts had.
None of this is lethal. They would have escaped the belts while having absorbed a dose of radiation far below the LD50.
Here was the cumulative dose the astronauts received during their entire missions: [63]
>TABLE I. - AVERAGE RADIATION DOSES O F THE FLIGHT CREWS FOR THE APOLLO MISSIONS
>Apollo mission Skin dose, rads
>7 0.16
>8 0.16
>9 0.20
>10 0.48
>11 0.18
>12 0.58
>13 0.24
>14 1.14
>15 0.30
The missions listed here lasted an average of 9 days.
Missions 11 to 15 lasted an average of 8.6 or so days.
Missions 11 to 15 saw an average cumulative dose of 0.488 rads.
1 rad = 10 mSv (millisieverts). So, this is 4.88 mSv, spread over the course of a week.
A dose of radiation lethal to absorb in a single day is usually 4-5 Sv (sieverts). What they absorbed over the course of a week was magnitudes lower than the amount of radiation that would be lethal to absorb in one day. Bear in mind, this is a skin dose. The amount of radiation they truly absorbed could be lower than the reported values.
The combined dose of all of the missions listed is equal to 34.4 mSv, which is still hundreds of times below the lethal dose of radiation.
This being said, the Van Allen belts aren't lethally radioactive. They do have dangerous levels when you consider long-term health and the development of cancers, but in the short-term, it's fine.
Let's look at the Reuters article that Wu cited: [64]
First off, the Van Allen belts aren't mentioned once in this article, and the article has nothing to do with the Moon. Here's the name of the article:
>What's keeping us from Mars? Space rays, say expertsWhat the interviewee, James van Hoften, says in the article is that with current technology it would take three years to reach Mars, and the radiation people would be exposed to during that time would be too much radiation; it would be harmful, and could kill them.
>Any mission to Mars using current technology would take three years, van Hoften said. That long in space would subject astronauts to too much radiation.
>"You can put on very thick walls and they just won't protect you from that," van Hoften said. "The younger you are the worse it is," he added, because as with many types of radiation, it can take years for the damage to cause disease.Bear in mind, James van Hoften is talking from experience. He himself went to space, and mentions that in relation to his experiences with cosmic radiation in the article. Cosmic radiation went through his skull, making him see a flash of light.
The dose makes the poison. In the case of radiation, that dose is measured by the strength of the radiation and the duration of exposure to the radiation. The Moon landings were a whole lot shorter than 3 years. The crews sent to the Moon would receive a far lower dose than people going to Mars. This article fails to prove that the Van Allen belts, or space radiation in general, would've killed the Apollo crews, since it wasn't intended to do this. Winston Wu has blatantly misrepresented this source of information to make it say something that it never said.
His final point is this:
*A guy at NASA who was on a TV show said the Van Allen belts would kill astronauts. (Footage of this statement is not present)
I looked for the footage of this supposed incident myself to no avail. Instead, what I found were forum posts from Moon landing-disbelievers ranting about this supposed incident. So this is hearsay. Another fallacious argument. Regardless of its veracity, assuming that this alleged incident even happened, the man could simply be wrong. Have you considered that? It's an appeal to authority. Winston Wu seems to love clutching his list of fallacies, much like every dumb conspiracy theorist ever e.g flat earthers, did he forget this one?
So if you buy the Apollo story, you'd have to buy that the Apollo Moon Landings were the first and only historical event in which technology actually went BACKWARD by an extreme magnitude! In history, when technological feats are accomplished, they get better, faster and more efficient in subsequent years. For example, when the Wright Brothers invented the airplane, every year after that planes got better and better. When Charles Lindberg made the first transatlantic flight in 1927, it was soon repeated afterward. And when cell phones came into the market, they got better and better thereon.
Wu is framing the issue in a dishonest manner. He is acting as though technology went backward regarding the Moon landings just because we didn't keep going there until this very day. There were _six_ missions to the Moon. Not one, not two. Six. They went to the Moon six times and they improved their practices each time, until they ran out of money.
The only caveat is that humanity was not able to pull together the means to send missions to and from the Moon without serious economic tolls. It's honestly quite a ridiculous expectation that Wu seems to have here, that America should've kept going to the moon. This is the root of his argument. According to Wu, if they didn't keep going to the Moon, if they chose to not do something prohibitively expensive, and gratuitously so, then it couldn't possibly have happened.
Not to mention that there have been robotic missions sent out into space, including towards the moon, since then. Is that not more technologically sophisticated? I mean, they literally sent a self-sufficient robot to Mars.[65] They have sent robots as far as Pluto.[66] They've been by every planet with robots. They've visited asteroids, and even tested a system for repelling asteroids, of which video footage exists.[67] This is very silly. Obviously, technology has advanced. Wu is lying to his ignorant, sheeple readers.
However, after the Apollo missions from 1969-72, it all went backward. We never went back again and neither did any other country. Nor did anyone even try to. It was very strange. At least the Soviets should have followed soon after, especially since their space technology was ahead of ours. Yet none have even tried. And NASA itself has nothing but excuses now when it comes to going back to the moon. What does that tell you? As they say, actions speak louder than words.
The USSR being beaten to the Moon caused them to reallocate their funding elsewhere. Why go to the Moon when other people have already been there? To simply prove that they could do it too? That's gratuitous. The USSR was still a developing country. Its populace had needs beyond going to the Moon, as did America, which is why they too stopped their programs.
Scientific data collected during the missions was shared, evidence collected has been studied internationally. The findings of the missions were shared with the world. There wasn't a need to be going on one's own as a country. The only reason would be to claim the fame of reaching the Moon first, but that opportunity was lost.
The space race might not have been some purely humanist, universalist project from an external perspective, regarding the politics of it, but that's irrelevant, because the whole space race paradigm died when America beat Russia to the moon. Why bother focusing on that aspect anymore, as a country? You already lost anyway. There's nothing to be done about it.
The only thing to do would be to prove that the missions were faked. But, this didn't happen, did it? This to me is only further evidence that they did happen. The KGB had quite deeply infiltrated America. They were arguably more effective at espionage than the Americans. They likely would have found something, given the scope of the missions.
The Soviet Union had infiltrated the Manhattan Project, which was an explicitly secretive program, with high levels of security, smaller than the Apollo programs, designed to create a weapon powerful enough to threaten the extinction of humans. If this doesn't speak to their ability to infiltrate big, secretive government programs, I don't know what would.[68][69][70][71][72][73]
Here?s my question: Why isn?t Wu skeptical of the fact that there?s a bunch of dead bodies on Mount Everest? After all, we?re _ALLEGEDLY_ so sophisticated, or so _they_ say. Why can?t we manage to get the dead bodies off Everest? Why can?t we manage to retrieve the corpses of the Titanic and other deep-sea shipwrecks either? Is it because technology went backwards? Is Green Boots merely a hoax to con the sheeple masses into believing in the myth of gravity? After all, actions speak louder than words.
Maybe it's just due to logistics and Wu is making logical leaps left and right.
2. Shadow anomalies indicate secondary artificial light sources
The shadows diverge and converge in many of the moon landing photos. Some of them even converge at perpendicular 90 degree angles. This cannot be if there is only one light source, the sun, as NASA alleges. Under the sun, shadows run parallel to each other. They do not converge or intersect. Thus, there must have been a second light source, such as fill lights used on a movie studio stage to balance out the lighting, since officially, the astronauts did not bring any other light sources with them.
Really, shadows do not converge or intersect? This is patently false. Go outside. Shadows do converge and intersect sometimes. It depends upon perspective. This is something you can freely observe here on Earth.
Apollo defenders try to cop out of this by claiming that the slant of the surface, angle of the sun and perspective of the viewer can cause shadows to converge or diverge. However, many of these shadows are on objects close to each other, and there is no indication that the sun is at an extreme angle. Most of the shadow anomalies were on fairly level surfaces, and even on those that weren?t, the slight slant was not enough to account for the distorted shadows.
If you've ever been in a room with more than one source of light, you may recall shadows from objects being cast in multiple directions. What Wu is saying here makes no sense. If there were multiple sources of light, then why does each object only have one shadow being cast in a particular direction? Make it make sense.
Then he shows a bunch of photos of shadows being cast in different directions and the US flag not having a shadow. He makes no effort to explain how this should be possible.
The Moon's surface is enveloped with dust called "lunar regolith". These are crystalline, electrostatically charged particles, often coated with glass. They're the product of meteoroid impacts and radiation from the Sun and from space. These particles are quite reflective, and can scatter light in many different directions. The uneven surface of this regolith will contribute to seemingly unnaturally-shaped shadows. The Moon is not like the earth. Comparing our subjective experiences with light here on earth gets us nowhere. [74]
3. Astronauts lit up in shadows by multiple light sources
In many Apollo photos of the alleged moon walks, the astronauts are seen standing in shadows while being clearly lit up and illuminated. This can only be possible if there was a second light source other than the sun. But officially, the astronauts did not bring any light devices with them, not even flashlights. This means that artificial lighting must have been used, such as on a movie set.
No, that's not the only possible conclusion. For one, they were wearing white which is the most reflective color. Secondly, the spacesuits were designed to reflect radiation, which will bolster their reflectivity. Thirdly, light would be bouncing off of the surface of the Moon and traveling over its surface, including traveling underneath and around the spacecraft. Additionally, the spacecraft itself can reflect radiation. If there was a second source of light shining on him from another angle, you'd notice the effect it would have on the shadow cast by the spacecraft. The shadow would be diminished, yet it isn't. Because they're not in a film set with a second light source.
Apollo defenders (such as Phil Plait, Jay Windley and the Mythbusters) claim that the astronauts are lit up due to the luminosity (albedo) of the moon's surface reflecting light onto them. However, this cannot be the explanation because:
>1) The moon's average albedo (luminosity) is only between 7 - 12 percent, which is comparable to that of asphalt (used in cement freeways) on Earth. Thus it could not illuminate someone standing in a shadow from the ground up like a light bulb would.
>See the albedo of various types of cement pavements here: http://www.pavement.com/Downloads/RT/RT3.05.pdf
>Documented info on the moon?s average 7 - 12 percent albedo:
>http://en.wikipedia.org/wiki/Albedo
>http://www.universetoday.com/19981/moon-albedo/
There's a few issues here.
For one, the Moon's surface is not made of asphalt. As I said before, the surface is lunar regolith. Crystalline, jagged particles coated with glass. The product of meteoroid impacts and radiation from the Sun and from space. This is not nearly the same as asphalt. Asphalt is made of crude oil and mineral aggregate. This formulates a black, matte, relatively smooth (compared to regolith) surface. The particles are bound together. It's not a loose surface of jagged, glass-coated particles, clumped together. Light is not going to behave the same way when it strikes asphalt. It can scatter, but it won't scatter in multiple directions as much as lunar regolith, as it has a lower roughness, and is a solid surface, not made up of loose particles. Light will also strike asphalt on the surface of the earth at a different angle than it will the Moon, which changes the dynamic of how it will spread across the surface. The surface of the regolith won't be smooth like a parking lot, it would probably be closer to being like a beach. There's also the fact that the Moon's surface is solely lunar regolith, whereas the earth's surface is not solely asphalt. Asphalt is localized to small areas. As I said, our subjective experiences here on earth give little insight into what it's like on the Moon.
Quoting digdeeper's oracle, NASA: [74]
>When NASA’s Apollo astronauts first stepped foot on the Moon, they left famous footprints in what scientists call lunar regolith. This surface layer on the Moon is fragmented, sharp rock material.
>Just like the Earth has soil, the Moon has lunar regolith. But an important difference is that soil is made of organic materials, whereas regolith is the result of the impact of meteoroids as well as charged particles from the Sun and stars.
>While the Earth’s soil is exposed to wind and water, which wear down the edges of the particles, the rock material of lunar regolith remains very sharp with fresh fractured surfaces. This makes the regolith potentially dangerous; it can quickly wear down space suits and equipment and be hazardous to astronaut health.
An article from West Texas A&M University gives further information on the Moon's reflectiveness.[75]
>There are two main types of reflectivity: specular reflectivity and diffuse reflectivity. Specular reflectivity measures how much of the incoming light gets reflected by the object in the direction given by the mirror angle. In contrast, diffuse reflectivity measures how much light gets reflected in all directions. A mirror has high specular reflectivity and low diffuse reflectivity. In contrast, sand has low specular reflectivity and high diffuse reflectivity
>Many objects display significant amounts of both specular reflectivity and diffuse reflectivity. For instance, a red polished sports car looks red from all angles because of its diffuse reflectivity, while at the same time displays bright spots of glare because of its specular reflectivity. In general, roughening a surface tends to increase its diffuse reflectivity and decrease its specular reflectivity. This is true because a rough surface has many little reflecting planes all oriented differently which scatter light in many different directions. In fact, the easiest way to turn a strong specular reflector into a strong diffuse reflector is to roughen it up. For instance, take a smooth sheet of ice and scratch it up. You turn a surface that is bright only in the mirror direction of the light source into a surface that bright in all directions.
>When it comes to planets and moons, the surface roughness is quite high. For this reason, their overall brightness is best described by their diffuse reflectivity. There are several ways to define and measure the diffuse reflectivity. In the context of planets and moons, the common and perhaps most useful way is to define it in terms of "bond albedo". The bond albedo is the average amount of total light scattered by the body in any direction, relative to the total amount of light that is incident. A bond albedo of 0% represents a perfectly black object and a bond albedo of 100% represents an object that scatters all of the light. The earth has a bond albedo of 31%. In contrast, the moon has a bond albedo of 12%. To bring this closer to home, the moon has the same bond albedo as old asphalt, such as is found in roads and parking lots.
From the wiki article cited by Wu: [76]
>The overall albedo of the Moon is measured to be around 0.14,[71] but it is strongly directional and non-Lambertian, displaying also a strong opposition effect.[72] Although such reflectance properties are different from those of any terrestrial terrains, they are typical of the regolith surfaces of airless Solar System bodies.
Here's the source cited as [72] which ironically disproves Wu's assertion that the moon couldn't possibly illuminate the astronaut because it has the luminosity of blacktop: [77]
>A lot of confusing statements are made about the albedo of the moon. The moon is, according to various accounts, "darker than blacktop" or "darker than a black sheet of construction paper." These are oversimplifications - neither blacktop or construction paper have the special characteristics of the moon. Besides, both materials can be found in colors that actually range from light gray to nearly black, so unless you specify a brand of construction paper, or a particular mile of highway, the assertion is next to meaningless even if it weren't untrue.
>Albedo is given in a variety of definitions, and the blacktop analogy is the result of the unwitting abuse of a couple of such definitions. Without knowing the definition that is used, its impossible to be sure you are comparing apples to apples. The simplest version of albedo is the Lambert albedo. A Lambert surface is one which scatters light isotropically - in other words, an equal intensity of light is scattered in all directions; it doesn't matter whether you measure it from directly above the surface or off to the side. The photometer will give you the same reading.
>For a lambert planetary surface, the illumination effects are entirely geometric. The brightest illumination is directly below the sun, and the amount of light reflected diminishes the farther you get from this point, simply because the sunlight is played along a greater arc of the surface. The illumination isophotes will be round. Unfortunately, the moon is not a Lambert surface.
>For one thing, the subsolar point does not provide the brightest reflection - the limb does. And the phase curve has a sharp peak in brightness during full moon - the moon is extra reflective at full compared to first quarter. Attempts were once made to explain this in terms of a Lambert surface with various kinds of topography, but this does not work out.
>It is now known that this departure from a Lambert surface is caused by the very porous first few millimeters of the lunar regolith. Sunlight can penetrate the surface and illuminate subsurface grains, the scattered light from which can make its way back out in any direction. At full phase, all such grains cover their own shadows; the dark shadows being covered by bright grains, the surface is brighter than normal.
>The picture is further complicated by the fact that the perfectly full moon is never visible from Earth (at such times, the moon is eclipsed). From the Apollo missions, we know that the exact subsolar point - in effect, the fullest possible moon - is some 30% brighter than the fullest moon seen from earth. It is thought that this is caused by glass beads formed by impact in the lunar regolith, which tend to reflect light in the direction from which it comes. This light is therefore reflected back toward the sun, bypassing earth.
>The original definition of albedo, proposed by Bond, is the ratio of total solar radiation scattered from a body to the radiation incident upon it. The Bond albedo of the moon is 11%. But limiting this figure to V-band radiation produces quite a different value. The average visual Bond albedo of the earth-facing side of the moon is 7.2%.
>This is what has led to the often repeated statement that the moon is blacker than even very black terrestrial materials. Flocked paper, often used in light traps and as telescope darkening material, has an albedo of about 6%, for example. But the low Bond albedo of 7.2% is the result of the porous upper layers, which cast shadows over a substantial percentage of the visible surface. No common terrestrial material has a similar layer, so it isn't useful for comparison purposes. So the black construction paper theory and the asphalt theory simply have to be abandoned.
>Another definition is the visual geometric albedo, which is the proportion of visible light received from an illuminated body at zero phase angle to that which would be received by a Lambert surface in the same position. For the moon, the full moon problem again intrudes. The visual geometric albedo of the full moon is 12.5%, but much less at other phases.
>Because it is very difficult to measure this value, the visual geometric albedo at 5% phase angle is often used instead. That should be self-explanatory; the value for the moon is about 8.4%. But it can't be used to compare with terrestrial materials for the same reason the Bond albedo cannot.
>Yet another definition - and by far the most useful for observers - is the visual normal albedo. This is the ratio between the brightness of a given area of an illuminated body at zero phase angle and oriented normal to the incident light, to that of a plane white Lambert surface similarly oriented. But normal incidence is never seen from earth (remember, the moon would be eclipsed), so they've introduced the "normal albedo at 5% phase angle" instead - which is a contradiction in terms, but I suppose we know what it is supposed to mean.
>The following is a list of the "visual normal albedo at 5% phase angle" of various lunar features. These numbers can be used to directly compare to terrestrial surfaces (reference cited below):
Then the author gives references to the brightness of some parts of the Moon, some of which are much higher than Wu's 12%, although the astronauts didn't travel to most of them. To continue quoting:
>These values are, as you can see, considerably higher than the other lunar albedos given. For comparison, the albedo of a green golf course is about 13%, roughly the same as that of the Cayley Formation which covers the floor of Ptolemaeus. So you see, the moon is not quite as dark as is often claimed - something about in the middle range of lunar brightnesses is just as bright as a grassy yard at noon.
So, the Moon can be highly reflective, much more so than Wu leads the reader to believe. His comparisons with the asphalt are simply nonsensical, as the astronauts were not standing on asphalt, they were standing on lugar regolith, which has vastly different properties from asphalt. They had the sun shining down upon them as well. To expect the astronauts to be cloaked in darkness when they stand behind the spacecraft is silly. They definitely could've been illuminated.
Onto the next assertion made by Wu:
This Universe Today article above even acknowledges that the moon?s surface is not very bright.
>so, how does the Moon albedo compare to other objects in the Solar System? As bright as the Moon looks from our perspective here on Earth, the Moon?s albedo is actually pretty low. The object with the highest albedo in the Solar System is Saturn?s moon Enceladus, which has an albedo of 0.99, which means that it?s covered with very reflective snow and ice. The Moon is much more similar to a very dark object, like an asteroid. The darkest asteroids in the Solar System have an albedo of 0.06. That?s pretty close to 0.?
He didn't quote the rest of the article: [78]
>The brightness of the Moon changes as its phases change. During the first and last quarters, the visible Moon is illuminated 50% by the Sun, but it only has about 8% of the brightness of a full Moon. This is because the sunlight is hitting the Moon at an angle and deflecting away from us. When the Moon is full, sunlight is hitting the Moon and then bouncing directly back. This is why the Moon is so much brighter during a full Moon
It shouldn't be a surprise that a surface covered in ice and snow is going to be more reflective than the Moon. Ever been out in the snow? Ever heard of snow _BLINDNESS_? Relatively speaking, compared to a super reflective, bright body of brutal ice and snow, the Moon is closer to a darker body like an asteroid. That does not mean it is exactly like a super dark asteroid, especially given the Moon's mass and shape and position in space. We're sinking into semantics now. Wu's poor reading comprehension has no bearing on the veracity of the Moon landing.
4. Buzz Aldrin spotlight photo a smoking gun blunder
Smoking gun blunder, or more optics that Wu doesn't understand?
The famous photo of Buzz Aldrin standing in the spotlight is a giveaway in that he is being lit up in a spotlight from alleged sunlight while the ground around him is shrouded in darkness! How can the sun put a spotlight around a particular person like a stagehand pointing a spotlight on an actor or singer on stage?! This was obviously a major screw up, and NASA was reckless for thinking that no one would notice or that they could get away with it. In fact, it was such a blunder that NASA even tried to cover it up by brightening the rest of the surface in subsequent versions of it. Why would they do that if they had nothing to hide?
Winston Wu got the images mixed up. The image he presents as the "original" is in fact edited. They changed the contrast to accentuate the shadows. The "edited" version is in fact the original. Also note that the "edited" image, which is actually the original, only highlights the peculiarity of the shadows because of how bright it is. I don't know why he'd point to this as evidence of a coverup. The edited version looks more natural and is easier on the eyes, thanks to the increased contrast.
I must ask, why is there a shadow on the bottom front-right of Aldrin slanting upward to the left diagonally? That shadow should probably not be there given the position of the supposed spotlight. Wu doesn't think of this though.
The explanation is that the lunar regolith is scattering light in various directions.
5. Indications of artificial backdrops used in Apollo images
In many moon photos, you can see a distinct line between the foreground and backdrop, which consists of different textures on each side. This indicates that the background is ARTIFICIAL, as in a movie set. Here is a clear example from a famous Apollo photo of an astronaut saluting next to an American flag. Notice that the backdrop also looks like a wall that is just behind the astronaut, rather than actual scenery in the distance. And notice the distinct line between the dirt and the white layer behind it.
They look pretty three-dimensional to me. There might just be a tiny hill/mound/elevation there or something. Either way, just because you _think_ something _appears_ fake does not mean that it is. So Wu then tries to prove that it's fake.
A technique known as ?stereoscopic parallax? also reveals that the backdrop used in the Apollo images is stationary and at close proximity to the astronauts, rather than far in the distance. For an indepth analysis using this technique with examples from Apollo images, see this page on AULIS Online: http://www.aulis.com/stereoparallax.htm
I read through the article, and there's a glaring flaw with it that completely destroy the point it seeks to make. To conduct stereoscopic parallax, the sample photos must be taken in positions exactly parallel to each other. This did not happen on the Moon. The astronauts were using chest-mounted cameras and were blindly snapping pictures. Wu himself states that the astronauts used chest-mounted cameras, meaning he does not fully comprehend the evidence he's discussing in his own article. The ground the astronauts stood on was uneven. They did not stand in the exact same body positions either. They were bumbling around blindly snapping photos. The precise positions of the cameras at each photograph were not recorded. These combined reasons mean that stereoscopic parallax using the photos cannot prove anything. The shape of the landscape looks different due to the perspective of the camera. The guy who made that paper may have a PhD but his technical skills are moot if the material he's working with is fundamentally flawed, which it is. The author himself explains how stereoscopic parallax works in the article. Does the author not know that chest-mounted cameras were used? Did Wu even read the article? Does the author even hold a PhD? I can't seem to find any trace of him beyond this article. Further research into aulis.com brought up claims that the guy who runs the website falsifies evidence by creating fake, seemingly credible, often-Slavic identities, to publish false evidence. So many questions.
6. Identical backdrops with different foregrounds and vanishing LEM
They must've been at a different position when shooting. The photos alone do not give any precise insight into the camera's perspective. Look at all that stuff on the ground which looks like gravel. These are clearly different positions.
7. Scotchlite glass screen visible in moon images after adjustment of gamma and contrast
In fact, the scotchlite glass background screen used in front screen projection is visible in many moon photos when you adjust the gamma and contrast. (I guess the hoaxers in the 60?s didn?t count on people today having the technology to examine such photos) You can see some examples here: http://www.assassinationscience.com/HowKubrickFakedtheMoonLandings-1.pdf??
Meaning you are committing to the idea that this was staged in a film studio, supposedly by Stanley Kubrick. Which means you're committed to the idea that he can somehow cast shadows in different directions, which is probably not possible in the context of how they supposedly staged the landings. Also, why would he cast shadows in different directions? If we hadn't gone to the Moon, why do that? There would not be a context for that phenomenon of light. They would be creating this peculiarity of shadows, which would needlessly draw suspicion from the public. They could've instead just had the shadows all cast in one direction.
Digdeeper in his own article mentions how "Nobody even believes the Stanley Kubrick angle". Really? Then why is the article that you're citing as some magnum opus bringing this up as a serious point? Did digdeeper read the article? Does he not consider Wu's article to be all that serious? Who knows.
Let's look at Wu's source, assassinationscience.[79]
Most of this document is just him arbitrarily drawing lines and saying that it's the cutoff between the set and the fake landscape. This isn't proof.
Now quoting from the document:
From page 20
>This is a processed photograph of astronaut Ed Mitchell on the surface of the moon taken during the Apollo 14 mission. Of course all of the stuff in the sky, as seen in this processed Apollo image from Hoagland, is impossible if it was taken on the lunar surface. There is no atmosphere on the moon. Therefore there can be nothing in the sky. Yet when Hoagland processed much of the Apollo lunar surface imagery he discovered, over and over again, all of this 'crud' in the sky above the astronauts
There are particles up in the space above the surface of the Moon. As the particles of the lunar regolith lose their negative charge from radiation cast off by the sun, they can be repelled off the surface of the Moon up into the space above the Moon's surface, until falling back down. They can go several kilometers high.[80][81]
Quoting from the document:
>No one in NASA even attempts to answer Hoagland, or anyone else, about the strange stuff that he, and others, is finding in the skies above the astronauts
I already knew the explanation after having read about lunar regolith, but, just to be fair to this guy, I also searched for an explanation from an authoritative source like NASA, and found one from NASA in a minute. You're just willfully ignorant. All conspiracists who whine about nobody wanting to answer their questions appear to do this: They make no effort to learn, and then make it everyone else's problem, in conspiratorial fashion, hinting at some sort of persecution by a cabal. It's a display of their entitlement.
Having genuine, somewhat complicated questions is one thing. I can understand that. But this is not a complicated question. It takes minutes of research to get an answer.
>Richard Hoagland theorizes that this is photographic evidence of huge, abandoned “glass cities” on the surface of the moon. He says that what we are seeing in the above processed image are huge glass towers that only show up on the images after they have been processed through graphics software.
End of quoting from the document.
Well, there could be actual glass in the air. Definitely not glass towers. The Moon is uninhabited. I mean, I don't think it would be feasible to make a tower out of glass anyway, not even on the Moon. The fact that this person is seriously suggesting the existence of glass towers implies that they're delusional. Probably not a person to rely upon.
That being said, this document doesn't refute anything. Most of it is just lines drawn arbitrarily across photographs. As for the "analysis" of the photos. This guy isn't working with the original film, he's digitally processing digitized images of the photos. Artifacts will appear on the screen, irrespective of the dust above the ground that he's unaware is dust because he's poorly-researched. Flat earthers do the same thing.
8. Sun image on moon turns out to be light bulb in enhanced image
DIGITALLY enhanced. It's important to clarify that. To which I ask, why must it be a giant lightbulb? Has he taken photos with a giant lightbulb in a film set comparable to the one he thinks was used to fake the Moon landings, photographed them with the exact same camera used by the astronauts, developed the photos in the same way NASA did, digitized the photos in the same way they did, digitally analyzed them, and discovered that they will look like what he claims to have discovered in the Apollo photos? Of course not. So this proves nothing at all. There's no parity. It's just artifacts appearing on the screen from the photo being excessively processed, as well as actual sunlight being accentuated. This is flat earther-tier evidence.
9. Lunar rover with no tire tracks on either side
There's several reasons why the tracks may not be present. Sometimes the crew may have walked over the tracks. In the photo shown by Wu you can literally see boot prints all over the place. It's ridiculous. The photos shown by Wu are also very low resolution. In higher resolution photos you can better see the boot prints and faint tire tracks.
And this is important to note: Winston Wu uses high resolution photos when it suits him, but when it does not suit him, he conveniently only has low resolution photos. Coincidence? Maybe. Another thing to note is the tires weren't your typical rubber tires. They were an open metallic mesh. Moon soil would pass through the mesh as the tires rolled over the ground at low gravity under no atmosphere. This would not leave deep impressions. There are also photos where you can see tire tracks. Here's one I found at a debunk website.[82]
If you watch "For All Mankind" you can watch the crew riding over old tire tracks in the rover. Although I don't know off the top of my head which specific mission that footage was from.
Additionally, the notion that the Moon landing fakers would somehow forget to add tire tracks is absurd. This is like with the shadows being cast in different directions, only far more absurd. To inject a detail such as this into the narrative, the concept of faint tire tracks, is gratuitous and only draws suspicion if you've never been to the Moon and as a result lack knowledge of what it's really like there. This is more likely to be the product of people not understanding physics.
10. Fake looking moon from orbit with giant shadow from command module
In this orbital photo of the moon that NASA claims was taken 95km above the moon?s surface
It's not a shadow, it's the silhouette of the nozzle of one of the reaction control system engines on the lunar module. Again, the notion that the hoaxers could overlook this is absurd. Not to mention why they would even have taken the photograph of a model of the Moon from inside of a shuttle suspended by wires in a film set. Why not just point a camera at the model of the Moon? Nobody is going to see the shuttle anyway. It's completely absurd.
11. Wires visible above Apollo astronauts in NASA footage
Or perhaps they're antennae or light reflecting off of antennae, or some artifacts. Watch actual footage instead of looking at cherrypicked 144p stills, you won't see any wires.
12. Bootprints cannot be made in dirt or dust without moisture
The photos of the astronaut bootprints on the moon dirt should not be possible. Boot prints are only possible when there is moisture in the sand or dirt. But on the moon, there is no moisture. When one steps on dry sand - such as on sand dunes - no footprint is left and no ridges from the shoe or boot soles are embedded. All that?s left is small dent in the sand. So this is a curious anomaly.
Well the Moon isn't made of sand so this goes out the window. Lunar regolith is very different from dry sand on earth. Its particles are sharp, angular, electrostatically charged, and often coated with glass. Its consistency causes grains to interlock and stick together. The Moon’s low gravity also makes the regolith's interparticle cohesive forces comparatively stronger than they otherwise would be on earth. Downward force applied to the surface will leave impressions. Comparing the earth to the Moon is a non-starter.
13. American flag fluttering on moon with no air or atmosphere
In a number of Apollo videos, the American flag can be seen waving on the moon, which cannot be possible since the moon has no atmosphere and therefore no air. This is very simple. Apollo defenders try to dismiss it by saying that the flag only waves when the astronauts are twisting it while trying to plant it. They claim that the act of twisting the pole is what?s causing the flag to flutter. But that?s not completely true, which is evident from the Apollo video clips. In several clips, you can clearly see the flag fluttering even with little or no movement of the pole by astronauts. Here is an example from a gif clip:
It's clearly not fluttering, it is bending with the movements of the astronaut holding it as he drives it into the ground. Why doesn't Wu link people to a longer clip instead of showing a short gif?
When held upright the flag is rigid, at full mast, and isn't billowing. It's at full mast because a rod was put in the flag to hold the flag at full mast. If you watch the footage, you can see the rod at the top of the flag (above the stars symbolizing the states of America). Anyway, all of this alone doesn't explain the rigidity of the flag. If they were on earth, the flag would not jitter mechanically as though it were made of metal. The flag only moves when acted upon by the astronaut. After he touches it, it shakes very slightly. The mechanics of the flag make no sense on earth.
Here's a longer clip that took me a minute to find: [32]
Here's another clip. In this one the astronauts comment on the flag waving.[83]
14. No blast crater under lunar landers
Under where the Lunar Lander (or LEM) landed there should have been a blast crater. But none of the Apollo photos show any craters under the LEM at all. Example image:
That is explained in the Wikipedia article on Moon landing conspiracy theories. It's hard to not come across the explanation.[84]
>1. The Lunar Modules made no blast craters or any sign of dust scatter.[102]
>No crater should be expected. The 10,000 lb (4,500 kg) thrust Descent Propulsion System was throttled down very far during the final landing.[103] The Lunar Module was no longer quickly decelerating, so the descent engine only had to support the lander's own weight, which was lessened by the Moon's gravity and by the near exhaustion of the descent propellants. At landing, the engine thrust divided by the nozzle exit area is only about 1.5 psi (10 kPa).
>Beyond the engine nozzle, the plume spreads, and the pressure drops very quickly. Rocket exhaust gasses expand much more quickly after leaving the engine nozzle in a vacuum than in an atmosphere. The effect of an atmosphere on rocket plumes can be easily seen in launches from Earth; as the rocket rises through the thinning atmosphere, the exhaust plumes broaden very noticeably. To lessen this, rocket engines made for vacuums have longer bells than those made for use on Earth, but they still cannot stop this spreading. The lander's exhaust gases, therefore, expanded quickly well beyond the landing site. The descent engines did scatter a lot of very fine surface dust as seen in 16mm movies of each landing, and many mission commanders spoke of its effect on visibility. The landers were generally moving horizontally as well as vertically, and photos do show scouring of the surface along the final descent path. Finally, the lunar regolith is very compact below its surface dust layer, making it impossible for the descent engine to blast out a crater.[106] A blast crater was measured under the Apollo 11 lander using shadow lengths of the descent engine bell and estimates of the amount that the landing gear had compressed and how deep the lander footpads had pressed into the lunar surface, and it was found that the engine had eroded between 100 and 150 mm (4 and 6 in) of regolith out from underneath the engine bell during the final descent and landing.
End of quotation.
But the LEM needs to fire its thrusters as it descends, or else it will crash or tip over and be damaged, which would big trouble. Apollo defenders dismiss this by arguing that either the LEM turned off its engine and glided down without thrusters
This is not true. It was turned down. It was still propelling upward somewhat to cover the weight of the module.
However, these explanations are nonsensical. If the LEM could just glide down like a parachute, then why did it have thrusters?
He's fighting ghosts right now.
Why did NASA?s own technical drawings show blast craters beneath the LEM?
Because the artist intuitively thought that there should be blast craters, just like you. This undermines your case, as it conveys the idea that the Moon is contrary to human intuition.
Here's a Harrier jet hovering around an airfield over grass. Its thruster has a velocity considerably higher than the lunar module's, yet there's no crater, nor burns.[85]
In the Apollo 11 landing footage, you can hear Armstrong saying that he turned off the engine after landing, not during the descent.Yeah, this corroborates the fact that the engines weren't off.
15. Slow motion movements and low jumps in 1/6 Earth gravity
Here is another discrepancy that is right under your nose that you never realized. The Moon's gravity is 1/6 that of the Earth's. What this means is that if you were on the moon, you could move faster and jump higher. But in the moon landing footage, the astronauts are actually moving SLOWER than they would the Earth! (oops, must be a major screw up there by the producers, or else they were not able to simulate low gravity in the studio?) Go figure.
The suits are designed in a way that will make it hard to move in a non-awkward manner. They're highly pressurized; the joints bend awkwardly. They were stiff.
The astronauts also had to move cautiously in order to prevent falling and rupturing their suits. Several dangerous falls were recorded while they were bunny-hopping around for fun. These could've caused fatal accidents.
The suits had a large mass and were very heavy on Earth. They would weigh less on the Moon, but their weight does not exclusively determine the force necessary to move the suits. The mass of the suits is the operative factor in the force needed to move them. On earth the suits weighed 82-90 kilograms. On the Moon they weighed about 30-33 kilograms, which is still quite a lot to be wearing anyway, enough that you probably won't be racing around.
Additionally, the lack of an atmosphere makes moving peculiar when contrasted against earth. The lunar regolith is also a peculiar surface to be walking on.
It's very obvious in argument #15 that Winston Wu doesn't know physics. That's not an inherently bad thing, not everyone should study physics. But if you're uneducated and use your lack of knowledge to claim there's a conspiracy afoot to an audience of equally gullible people, well, I don't think that's very good. If you're uneducated and ask questions, then you might find answers, like for why the lowered gravity is not a discrepancy in regards to their slow movements. This is 9th grade level physics.
The following arguments will further reveal the fact that Winston Wu doesn't know physics. I guess he didn't learn this stuff in high school, or forgot it. Such are the failings of the American education system.
16. Van Allen Radiation Belts and solar flares would have been lethal to astronauts
We've already been over this...
This guy Jarrah White is being intellectually dishonest. He writes:
>Even after Van Allen shielded his Geiger counters with lead, the results were still equivalent to 10-100rad/hr. He concluded that effective shielding of astronauts was beyond engineering feasibility available at the time, that even a rapid transit through the belts would be hazardous, and that for these reasons the two belts must be classed as an uninhabitable region of space that all manned space flight must steer clear of.
James Van Allen as far as I'm aware never spoke of the feasibility of engineering against cosmic radiation, and even if he did, he is not the arbiter of engineering shielding against cosmic radiation. It's not entirely false that the estimated absorbed radiation was 10-100 rad/hr, but this is the equivalent of a couple dozen to hundred mSv, which is nowhere near the lethal dose of 5 Sv. There is even less radiation in space than in the belts themselves. There's people in space right now, who have been there for months. This is nonsense. Shielding will lower the dose significantly, and it evidently did.
>Even if we discount the Van Allen belt, there are still other dangers to consider. The sun constantly bombards the earth-moon system with solar flares. Regardless of whether these flares deliver x-rays or protons, or are minor or major, both are a hazard to humans. A major flare delivers in excess of 100rad/hr, a minor flare can deliver 25rad/hr depending on how many centimetres of water shielding is used. The minor flares of May 10th and July 15th 1958 for example, would have required 31gm/cm2 of water just to bring their dose rates down to 25rad/hr [Fig-3]. The Apollo capsule, with its aluminum honeycomb hull and outer epoxy resin ablator, was rated at 3gm/cm2 on the walls and 8gm/cm2 on the aft heatshield. The thicker portion of the spacecraft walls would bring the dose rate of such flares down to around 1,000rem/hr. The records show that 1400 of these minor flares occurred over all nine moon flights (Tables 1 & 2). NOAA?s Comprehensive Flare Index for Major flares, also reveals that thirty of the major ones took place during the Apollo missions. By any definition, these astronauts should have been as dead as spam in a can.?
He mentions solar flares, which are undoubtedly a danger. The thing is that there weren't any major solar events during the Apollo missions to the Moon. They were planned to occur when there would not be such solar activity.
You can cite how many solar flares occur, and their average level of frequency, but this does not give any qualitative insight into the level of exposure to radiation people will experience.
You also need to mention the fact that there will probably not be a steady, unchanging dose of radiation like 100rad/hr. The levels usually fluctuate and decrease as the storm passes. Presenting the dosage as a constant, unwavering level, inflates its severity.
By all accounts, there weren't any major solar events during the missions. In 1972, there was a series of massive solar flares which could've lined up with the astronauts' missions, but they didn't.
Need I repeat that there are astronauts in space right now, who have been living there for months. Astronauts who go to the ISS usually live there for several months to a year. Astronauts have been doing this for years now. These astronauts also have to deal with solar flares, including major solar events. But they're alive. Their cumulative doses should be far higher than those of the Apollo astronauts, yet they're somehow living. It's as if cosmic radiation isn't as dangerous as Jarrah White has made it out to be.
Not to mention the various animals sent to space, which weren't killed by the — according to Jarrah White — ceaseless solar flares of death, in spite of some of them being in space for weeks.
This study estimates how much radiation astronauts could've received during the August 1972. The doses wouldn't have been immediately fatal, but could've caused serious radiation poisoning.[86] So, even a legitimately dangerous solar flare probably wouldn't have killed them.
The radiation from the Van Allen belts is dangerous for long-term health, but it is not acutely dangerous. They are not so radioactive that you will die after a short duration of exposure.
And to repeat what I stated earlier, only one crew passed through both the inner and outer belts. The rest passed through only the outer belts. They passed through the thinnest part of the belts at high speeds in order to minimize their exposure. The spacecrafts were also shielded, in order to mitigate their exposure.
17. Smoking gun footage of Apollo astronauts faking a shot of being halfway to the moon
Initially, I didn't want to bother with this point because of how infantile it is, and how infantile it makes Wu out to be, but I guess that's kind of the point of this refutation.
In Bart Sibrel's documentary "A Funny Thing Happened on the Way to the Moon" (available on YouTube) unedited video footage is shown of the Apollo 11 astronauts faking a shot of the Earth from low orbit, while radioing to NASA that they were 130,000 miles from Earth, halfway to the moon. In it, you can hear the astronauts saying that the video camera was put up against the window. Yet something blocks the view of the alleged distant Earth, and a light structure can be seen moving in the corner as well, which isn't possible if the camera were situated against the window. And when the lights go on, we see the blue light outside, which means they were either in low earth orbit, or in the daylight blue skies of Earth. In fact, the blue light can be seen from two separate windows in the command module!
Wu's description was so incoherent that I had to waste 46 minutes sitting through some shitty "documentary" in order to figure out what actually happened here.
This "documentary" is so disingenuous.
Sibrel, around the 34 minute mark, presents a clip that supposedly shows the astronauts of Apollo 11 creating the illusion of a full Earth from a distance. Sibrel also claims that the astronauts are discussing how they will fake the shot. Sibrel presents the footage as never before seen, and totally unique.
It's a complete lie.
The radio transmissions were broadcast live to the world. The footage was broadcast live to the workers at Goldstone, where they could record it, and play it back later. The discussion they are having is about configuring the broadcast, it's a completely miscellaneous discussion, nothing like what Sibrel presents it as.
These webpages contain the transcripts and audio transmissions, with links to the footage.[87][88] Here is the raw footage pertinent to the documentary.[89][90]
The idea that they would have been orchestrating how they are going to fake the shot of Earth while on a live radio broadcast that thousands of people are listening to ridiculous. There's no privacy to be had. Why wouldn't they have orchestrated how they would fake it _beforehand_? Well, that's probably what they would do.
Understand too that only about 20 seconds of this raw footage was ever broadcast to the public, and these conversations discussing their deception were believed to be private... until now.
says the British narrator lady that dumb-fuck Sibrel hired because he perceives British accents to sound "smart" (why do shitty conspiracy documentaries made by stupid Americans always use British narrators?). That is such a bold-faced lie, it's incredible. I found plenty of footage on YouTube unlinked to this "documentary". Here's more footage.[91][92]
This "documentary" is not revealing any new footage, Bart Sibrel is just a lying scumbag.
The broadcasts were recorded and then played back for the public. The radio transmissions themselves were live and could be heard by whoever was listening, which included journalists present at NASA.
Mechanistically the explanation is also nonsensical. Sibrel says that it's a zoomed-in shot of the earth. If that were true, we would see clouds moving over the surface of the Earth rapidly, which we do not see. The clouds are relatively unchanging, and the earth spins slowly. Furthermore, you can literally make out continents. I think I see the Americas and Africa in one of them. The astronauts also describe continental landforms in the recordings.
Here's footage from relatively low earth orbits.[93][94][95][96] It looks nothing like the footage presented by Sibrel, of course.
Earth is much too large for a shot like this to be pulled off from low earth orbit. You need to have zero spatial reasoning skills to be fooled by this.
Sibrel also claims that the spacecraft had circular windows. There weren't circular windows. Just a small thing to mention.
This is a huge SMOKING GUN in the Moon Hoax debate. Other moon hoax films such as "What Happened on the Moon?" and "Apollo Zero" also analyze this smoking gun footage. So you have to ask, why would they fake a shot of the Earth being far away if they didn't have to?They didn't fake it, so there's no problem here.
Further, during Sibrel's interview with Buzz Aldrin (the Apollo 11 astronaut) when he showed Aldrin this "smoking gun" footage, which Aldrin himself took, Aldrin indirectly admitted that he was right. He replied, "This is going to make you famous isn't it?" Now, why would it make him famous unless it was true? This occurred just before Aldrin punched him outside, which became an infamous event that made headlines in the moon research community. You can see this interview and Aldrin?s punch on Sibrel's film "Astronauts Gone Wild" (available on YouTube and MoonMovie.com) or on any shorter clips on YouTube by searching for ?Buzz Aldrin punch? or ?Bart Sibrel punch?.
Winston Wu doesn't understand social cues. He has also the naivete of a child, unable to identify Bart Sibrel, a scumbag "documentarian" who makes up lies about people, for what he is, and unable to understand why someone would dislike such a person. He deserved to be punched in the face.
18. Apollo space suits and cameras had no protective ability against extreme heat and cold
This is a lie. They did have protections. The suits were highly reflective and they had a liquid cooling system to regulate their body temperature. Wikipedia has an article on this, so you can't claim that this is some arcane knowledge.[97]
Due to there being no atmosphere on the moon to provide convection for heating and cooling, on the daylight side, which all Apollo missions landed on, temperatures are at 250 Fahrenheit and in the shade drop drastically to 250 below zero.
Notably, Wu does not mention that due to the lack of an atmosphere there also would not be many ways for heat to travel to the astronauts but through their feet or direct sunlight. Their feet were protected, and their suits were highly reflective, protecting them from the sun.
Like I said, Winston Wu doesn't know basic physics. As such, he should hold his tongue.
19. Discrepancies about seeing stars from lunar surface by Armstrong and Collins
During the Apollo 11 Post-Flight Press Conference (which you can see on YouTube), Neil Armstrong said that they were not able to see the stars with the naked eye from the surface of the moon, to which Michael Collins looked at him and said ?I don?tremember seeing any? (even though he was allegedly on the command module in orbit and not on the moon?s surface, which was strange). Oddly, in the Apollo 11 Press Conference transcript, Collins? statement was attributed to Buzz Aldrin, perhaps in an attempt to cover for his slip up?
This is not true. You are regurgitating some lies from the shitty "documentary" Bart Sibrel made. It's pathetic too because the almost-full context is in the "documentary" itself. At the timestamp 47:13, we have the following dialogue: [98]
Question: ... When you looked up at the sky, could you actually see the stars in the solar corona in spite of the glare?
Neil Armstrong: We were never able to see stars from the lunar surface or on the daylight side of the Moon by eye without looking through the optics. I don't recall ... during [the solar corona] what stars we could see.
Michael Collins: I don't remember seeing any.
And that's it. This discussion is specifically pertaining to the solar corona, when they were behind the Moon in the spacecraft. It's not a general question of whether they could see the stars or not.
They did see stars while out in space, the transcripts show this.[99]
>071:59:20 Armstrong: Houston, it's been a real change for us. Now we're able to see stars again and recognize constellations for the first time on the trip. It's - the sky is full of stars. Just like the night side of Earth. But all the way here, we've only been able to see stars occasionally and perhaps through the monocular, but not recognize any star patterns.
End quote.
However, any professional astronomer will tell you that one can see stars from the surface of the moon much more vividly than from the earth, due to the moon's lack of atmosphere. Even Phil Plait of BadAstronomy.com stated this in a radio debate with Joe Rogan about the moon hoax. This is a huge glaring discrepancy in direct contradiction to what the Apollo 11 astronauts claimed, and has never been resolved. Perhaps it was a huge cock up by Armstrong and Collins during the press conference. Even NASA's chief public defenders such as Phil Plait are at a loss to explain it.
Well Phil Plait is wrong, assuming he said what you say he said, and you're not misquoting him. I don't know who he is and frankly I don't give a fuck who he is. I can't be bothered to research this drama whatsoever. You wouldn't see stars on the surface of the Moon with the sun shining on you, the brightness of the sun blocks them out. You don't see the stars on earth during the daytime either.
What?s more, Michael Collins later contradicted himself about not seeing the stars in his book ?Carrying the Fire?. On page 221, he wrote:
>"My God, the stars are everywhere: above me on all sides, even below me somewhat, down there next to that obscure horizon. The stars are bright and they are steady. Of course I know that a star's twinkle is created by the atmosphere, and I have seen twinkle-less stars before in a planetarium, but this is different, this is no simulation, this is the best view of the universe that a human ever had." - Michael Collins, Carrying the Fire, pg. 221
Unfortunately for you, I downloaded the book on libgen and read the chapter of his book containing the page you're quoting from for the full context. That quote comes from him recounting when they began to orbit the Earth, after exiting Earth, and he was doing an EVA as they were on the dark side of the Earth. Completely different context. This proves absolutely nothing whatsoever. He was in the shadow of the Earth and could see stars in space, this is absolutely possible. If he was on the dayside, he couldn't see them, and that's how he describes it, he only saw stars once it became nighttime for him. They had been on the dayside, and then they passed over to the dark side, and there was this dramatic change that he described.
It would seem that the astronauts cannot make up their minds about whether they saw stars from the moon or not. Very suspicious, no doubt.
You're unfathomably stupid, if not an outright liar, deliberately building a false case. Anyone who listens to you is even dumber.
20. Live video footage from Apollo contained cuts, jumps and edits
The live video footage of the Apollo astronauts could not have been live, as alleged by NASA. The videos that were broadcast showed jumps and discontinuities in the footage which could only have occurred through editing. One can see this by ordering the Apollo footage from Spacecraft Films, which claims to contain the unedited footage that was broadcast live to the world during the Apollo missions. This means that the scenes were pre-shot BEFORE the moon missions took place, which means that they were staged. So again, why would NASA stage the footage if it didn?t have to?
To see evidence and examples of this, see Jarrah White?s documentary ?Flagging the Gems? on YouTube. Jarrah?s Moonfaker website FAQ goes into this in more detail:
He then cites Jarrah White's webshite.[100]
>?The second smoking gun is the fact that the Apollo 10 telecasts were proven to have been pre-filmed and edited together. After every space mission, NASA releases a ground-to-air communications transcript covering everything the crew and capsule communicators (Capcoms) said during the flight. The company Spacecraft Films sells what they claim is complete and unedited television transmissions and 16mm reels from the Apollo missions. Jarrah purchased the Apollo 10 DVD set and compared the in-flight videos with the transcript. To his astonishment, Jarrah found numerous occasions in which the views of earth and even interior shots would cut from one angle to another and yet the audio would remain perfectly synchronized to the video with no signs of interruption when the video cut. So we know that the astronauts didn?t simply cut the camera and then begin rolling moments later.
>The Apollo astronauts had only the one television camera hooked up to the S-band antenna, so these broadcasts should be one continuous shot with no edits - as per the false claims made by propagandists. Because these edits only take place during post production, not whilst the video is being recorded, it would not have been possible to cut and paste LIVE video. The only logical conclusion is that the views of earth were pre-filmed, edited together, and then sandwiched between the interior shots with the ground-to-air communications dubbing the video regardless of the edits. Transitions from these fake views of earth videos to interior scenes were pulled off by conveniently cutting the camera or blacking the scene from interior to exterior and vice versa, in one circumstance Eugene Cernan went as far as putting a piece of paper in front of the camera lens during this switch from exterior to interior!
>By comparing the videos with the transcript, Jarrah also discovered that there were sections of video missing from the ?complete? Spacecraft Films DVD set. Jarrah knows these missing pieces of video exist, because in the transcript the Capcom confirms that the MSFN was ?receiving? them. For reasons unknown, Spacecraft Films omitted minutes of footage from Apollo 10 and then sold their DVD set to the world as ?complete & unedited.?
>After Jarrah released his video covering this, ironically titled ?Flagging The Gems?, Mark Gray of Spacecraft Films flagged it for copyright infringement and had the video pulled along with Jarrah?s entire Youtube account. Gray?s copyright claims are fraudulent and thus he is guilty of perjury, because NASA?s in flight telecasts are PUBLIC DOMAIN. They are not copyrighted.?
Key words: "what they claim". This is pathetic, I swear, these people are like children with how easily deceived they are. The company probably ripped that guy off. Instead of realizing they got scammed, they assume the Moon landing was a hoax. What's more likely? (1) International multi-generational, decades-long conspiracy implicating at minimum tens of thousands of people; (2) Company lying to people for money.
21. Implausibility of docking with command module moving at 4000mph in orbit
Ever heard of conservation of momentum before, you fucking idiot? People like him are idiots, and it's not for being uneducated, it's for being willfully ignorant. He could so easily learn some basic physics concepts. People like him make these assertions while not knowing what they're talking about. Obviously they aren't going to try to dock an object moving at 4000mph in relation to them. They'll accelerate to a similar velocity first. This is just absurd.
I shouldn't even continue this review, this should be my cue to stop. I'll continue anyway.
22. Nothing new in technology works right the first time
Anyone involved in engineering, computer programming, or technology development can tell you that nothing new in technology works right on the first try. Sending humans 240,000 miles to the moon and back safely is a harder task than you can imagine, rifled with unsolvable problems even today. So what are the odds that it all went right the first time without casualties?
The Moon landing was not "new" in "technology" in the same sense as a computer program. Sending people to the Moon and back is not the same as coding a computer program, compiling it, and discovering an error, or running it, and discovering an error.
There were several missions into space in order to gather data and develop spacecraft. Then they had missions to the Moon without actually landing and walking around. Then, eventually, they landed on the Moon. They eased into it, they didn't just go there in one shot. There's a reason it was called Apollo 11. "11". That number means something, I'll let you guess.
One of the Moon missions, Apollo 13, actually had this problem where something in the ship burst and the spacecraft leaked its cryogenic oxygen supply, which forced the crew to bail the ship and return back to earth via the LEM. That right there is a failure.
Bill Kaysing, author of "We Never Went to the Moon" was an engineer at Rocketdyne, the company that built NASA?s rockets, and remarked that he was told that the chances of going to the moon and back safely was close to zero percent. There were way too many obstacles that could not be overcome back then, and even today.
Huh, what do you know, some random asshole said something, so it must be true. It completely debunks the whole narrative. What a joke.
This guy isn't just some random asshole though, he's the progenitor of Moon landing conspiracies. Thanks to him, we have to deal with idiots like Winston Wu.
Thus, it makes sense that rather than send three men to their deaths in space for the world to see, which would have been disastrous for them, it was better for them to fake
How did they fake it, that's the main thing you're avoiding. You have to (well, if you want to be taken seriously, you don't _"have"_ to do anything) actually go over the narrative leading up to the Moon landing, establish what you believe to be true and false, until you've reached the Moon landings themselves, and the time after the landings. It's not possible in this context to simply "disprove" them having happened by not understanding conservation of momentum.
27. Apollo 11 astronauts looked guilty, sad and reluctant during Post-Flight Press Conference
This is one still from a press conference that's over an hour long. I sat through the whole thing. There was laughter and emotion. They were also kind of spaced-out though. Probably because they had been in quarantine for weeks after returning from space, and aren't public figures trained for television. Some of the conference is quite dry, with them explaining technical stuff. It's not all conducive to humor, but there were humorous moments. I'm not gonna timestamp every moment. There's one around the 4th minute, another around the 39th minute.[101]
That's about the end of his physics related suspicions One can logically question the probability of the Moon landing, by factoring the seemingly absent tire tracks, or the mechanics of the light on the Moon, but there's an issue here. Such a person would be applying their own subjective experiences on earth to an extraterrestrial body with properties totally different from earth. Your logic in scrutinizing an event like this is only as good as the information it is based upon. In the case of Wu's logic, it is based completely in ignorance. He's making a sort of meta-observation — an observation of an observation. In this case, it is observations made by an uneducated person of observations made by educated people who went to the Moon. You can incredulously question how probable it is for things to behave in a certain manner on the Moon, but your incredulity is completely meaningless when you haven't been to the Moon and made the observations people there have made and also do not understand physics. There isn't anything he's proposed that hasn't been refuted a million times over. Everything recorded throughout the Moon missions is 100% physically possible. A lot of Moon landing conspiracy arguments are often called PRATTs (points refuted a thousand times) because they've been refuted countless times but willfully-ignorant people who hate actual learning and who've only learned about the Moon landing through conspiracy websites keep bringing them up. No. This is all being argued without basis. The project was so large that countless people had sensitive knowledge of the operations involved in it. Countless people were in the control rooms, monitoring the rockets (this was filmed in the documentary I sent). These people all had to be in on it. People were not on a need to know basis in the same sense as the Manhattan Project, where you had people refining nuclear materials, while being totally oblivious to what they were doing, and the purpose of their job. There was a high degree of coordination. Tracking stations, observatories, and radio enthusiasts all around the world monitored the Apollo missions' transmissions and trajectories. India and China, both nuclear armed countries who aren't allies with America, have independently verified the landing sites. They have to be in on it. Retroreflectors placed on the lunar surface by Apollo are still used for laser-ranging experiments by independent labs, demonstrating objects are where they're claimed to be. All of the people involved in these experiments must be in on it. You can claim that they were put there by something else, but you're just conceding that we can send things to the Moon, which opens the possibility of sending humans there. Hundreds of thousands of people worked on the missions, developing the equipment for it. This all had to be for nothing. For these people to not realize they were being conned, they would need to be working off of real-world data, which causes you to concede that spacecraft were sent into space to make measurements. How is it possible that there is an ongoing conspiracy involving countless people, which is being passed down to new generations, to this very day while remaining utterly undetected? Such a conspiracy would be harder to pull off than the Moon landings themselves. Like I said before, people made real technology with real data. Why was that? Because it was all real, that's why. One commonality these conspiracies all share is that they became known to the public. It's the common link between every known conspiracy. So this here is just a non-starter. History proves that large groups of people can't keep secrets of this nature for more than a couple years. The Manhattan Project was infiltrated by the KGB, so it was not a perfectly-kept secret. The people with intimate knowledge of the program were sworn to secrecy by severe punishment. There was also somewhat of an incentive in not leaking the program, like giving the Russians the bomb first. A lot of people could be intimidated by the notion of the Russians winning. It was more of an existential threat than being beaten to the Moon. The project also had an end goal, which would result in the Atomic Bomb becoming known to the whole world. It only lasted 3 or so years until it became public knowledge. The Moon landing is a conspiracy intended to be kept secret for an undefined duration of time. The people who launched the rocket are known to the public. There were a ton of people who had to monitor the status of the rocket and the crewmembers, how were they all fooled? Countless people to this day confirm the reality of the Moon landings. Are they also all being fooled, or are they in on it? Wu doesn't even bother to explain this. He's not offering any alternatives to the Moon landing, he's just nitpicking the Moon landing narrative because of things he does not understand. It wasn't a secret because outsiders knew it existed. Maybe some internal details were secret but that's beside the point. The blueprints of many fighter jets are classified, but we know they exist, because we see them flying around. These agencies specifically select for people that will keep quiet, and regularly subject agents to tests like polygraphs (even though polygraphs are pseudoscience). Nonetheless, we have plenty of books outlining conspiracies the CIA has been involved in and we have whistleblowers like Edward Snowden (he, like many other whistleblowers and spies passed his polygraph tests). We have ideas of the kinds of stuff these agencies do. Horrible conspiracies they're involved in become known to the public. Victims of CIA torture that are alive and tell their stories. While the conspiracies are unfolding there is evidence of their existence. There isn't some indefinite retention of the truth like the alleged Moon landing hoax. It eventually comes out. Yet this hasn't happened with the Moon landing. Why is that? Because it happened, that's why. Hell, even Edward Snowden said he found no evidence of a conspiracy. But, as we all know, Snowden was merely dispatched by the NWO to distract the sheeple from Miles Mathis' profound truths, just when Mathis was beginning to catch on and become popular. That's not true. In university you learn material through falsification. You perform experiments to test so-called established scientific fact and by doing so you build your knowledge base by determing that what has been established is true. Science is itself a process of falsification by which discoveries are made. The opposite of what Wu's saying is true, and Wu is relying on the uneducated readers' lack of insight into scientific study in order to fool them. He may be doing this unintentionally, I think Winston Wu is just that ignorant and inculcated with propaganda from grifters. Wu's reasoning for the government's motivation to fake the Moon landing is circular. This is nothing like stealing a million dollars. Stealing a million dollars is stealing a million dollars, and having it for yourself. What this is, is ordering a company to build you a tower, costing said company a total of a million dollars, only for you to blow up the tower. You do not gain anything, because you destroyed the thing that all of the money went into. What's the reason for it? To concoct bigger lies? Well, that assumes that this event was a lie. I don't believe that it was a lie after picking apart this article, which leaves the primary motivation for doing the hoax without a base. The government does lie in order to control people, but the lies it tells do not relate in any way to moronic conspiracies of this sort. The lies are told for the sake of getting the masses to permit the government to do some monstrous act in order to obtain wealth and power, usually for the capitalist class. An easy example is WMDs in Iraq, and the link between Saddam Hussein and al Qaeda. The US Government didn't need to fake the Moon landings to get people to accept such lies. All they needed was mass terror, nationalist fervor, racism and Islamophobia. Eventually, the lies were exposed, and the spineless American citizenry did nothing to hold the monstrous Bush regime warmongers or Military Industrial Complex warmongers and corporations accountable, much like they never do anything to hold their government accountable for anything it does, which the government and capitalist class surely is aware of. The Coronavirus has done more to combat American imperialism than American citizens ever have.[103] Back to digdeeper's article No. The Moon landings happened, and neither you, nor Wu, ever established any basis for why the Moon landings had to have been faked in order for the masses to accept actual conspiratorial lies e.g WMDs in Iraq. Look at the current fiasco with the Epstein files. We now know for a fact that a significant proportion of American politicians and the capitalist class are out and out pedophiles who rape children, and have had their victims murdered to keep them silent. We know that an even more significant proportion of American politicians and the capitalist class know that their compatriots are evil murderous pedophiles, do not care, and work alongside them to maintain their own interests. The emperor has no clothes on, we all see this and are not even pretending otherwise. We are merely doing absolutely nothing about it, because we as a collective are so ungodly privileged, lazy, and uncaring. In a country with a moral backbone, every last one of these people would be lying dead in the streets, but not in America, because Americans are demonic cattle. It was a harmful disease that killed many people after spreading across the globe. Resistance to the measures proposed by health officials contributed to the death toll and prolonged the pandemic. You have legitimate gripes with capitalism, GMOs, the legal system, the school system, corporations and the government, but you've gotten them intertwined with nonsense and are wasting your time obsessing over said nonsense instead of things that actually matter. You perceive a coordinated conspiracy to keep wars going, when it could simply be that its in the best interest of all of the governments (and companies) involved in said wars to keep them running. Some of your beliefs around the Moon landing and 9/11 are harmless. Your views on COVID on the other hand could have been a harm to yourself and others. It is deeply ironic that you view technology like vaccines or historical events like the Moon landing as oppressive things intended to keep us from progessing. You should always ask yourself "How do I know this is true?" You should try to hold your sources of information to equal standards. You shouldn't favor certain sources of information because they pander to biases that you may possess. You should seriously scrutinize each bit of information, no matter where it comes from. Only then will you reach something close to the truth. Or you can remain meaningfully-biased (everyone's biased, some to the extent they cannot accurately analyze information), but you may as well forgo the veneer of rational skepticism. The Moon landing is a good reason for digdeeper to not hate on public education. Posturing as someone who seeks advancement, positive progress, while simultaneously campaigning against institutions for learning what allows you to visit places like the Moon. Let's move now to your COVID article This will be the second article of yours I look at. To summarize my stance: To summarize these points I've brought up: Event 201 concerned a SARS-like coronavirus. You latched onto this, questioning why they didn't select some random viral or parasitic diseases to be the cause of a global pandemic in their simulation. They did not select such diseases because those diseases do not have the characteristics needed to cause a pandemic. Coronaviruses had a historical precedent for causing massive outbreaks, which was why they chose one. It was logical to choose one. The simulation predicted around 65 million people dead, which is almost double the upper-estimate of global COVID deaths, and they simulated these deaths as having occurred in half of the time that COVID killed all of its victims. Essentially, their simulation didn't align with reality whatsoever. In their simulation, they made several vague predictions that anyone with a rudimentary understanding of geopolitics could make. These were not meaningful. But, you erroneously perceived them as being meaningful, much like you perceived their decision to choose a coronavirus as being significantly meaningful. The lab-leak hypothesis depends almost entirely upon circumstantial evidence once its direct, empirical evidence is refuted. You stated that a natural origin for the virus hasn't been found, stating that the hypothesized pangolins were ruled out. This is irrelevant. Few diseases have had their origins definitively linked to a given source. They are hypothesized, evidence is compiled, and people determine the most likely origin. This is what has happened with COVID. The search initially honed in on markets in Wuhan, China, and has remained there, as other locations have been ruled out. You said that COVID's furin cleavage site had a rare arrangement of genes, 1 in 36. But evolution is not like rolling dice. Natural selection would select for what is decent, if not what is best (this usually isn't the case), leaving you with such an arrangement. The sequence was actually not optimal, but it was functional. You said that the furin cleavage site contains a genetic sequence found in Moderna patents, with a 1 in 3 trillion chance to occur naturally. The 1 in 3 trillion figure was the conjecture of the authors who reported this finding, not a legitimate metric of any sort. As it turned out, the sequence did not lead to a furin cleavage site, meaning it wouldn't contribute to enhanced infectivity. The sequence is in Moderna patents, but it has also been found in a variety of organisms, demonstrating that it can in fact occur naturally. This nullified the significance of the genetic sequence. The conspiracy itself appears implausible. Only around 5 million dollars of foreign aid reached the Wuhan lab, spread across 2014-2019. Biological weapons programs have historically cost far more than this (hundreds of millions to billions). Professors of microbiology, viral genomics, and immunology that I've cited have stated that five years would not be enough time for COVID to have become sufficiently distinct from RaTG13. We can take the timeline farther back to 2007 when the Bush government approved $2million dollars in funding for various research centers in China, which could have theoretically included the Wuhan lab, though I haven't seen any actual indication of this. Even still, 12 years is probably not enough time. The conspiracy would be spread across two to three different presidencies. An unknown amount of people would be involved. Presumably, the conspirators would need to experiment upon animals, and possibly humans, in order to test their virus. This would create a lot of evidence, of which none has been reported. In your commentary on the Pfizer trial, you judged an individual's overall risk of getting COVID off of how many people studied in the Pfizer trial got COVID. This is erroneous. The infection rates in the study could give insight into the demographics studied, in the context of the regions where the trials were carried out, but certainly not an entire country, nor the entire world. Case rates and deaths pertinent to one's region would be more reliable for determining one's personal risk, though I know you believe these to be fraudulent, which we'll go over. You also sowed doubt as to how many subjects in the study truly had COVID, postulating that people could have potentially been deemed COVID cases by having a positive test, in addition to muscle soreness from a vaccine. That is true only if you completely ignore temporality and the ability of people running the study to assess subjects on a qualitative basis. The trials recorded data on injection-site painfulness (a detail you omit from your article). This single point completely nullifies your hypothesis. It's just nonsensical to make an argument like this. Furthermore, few people will have soreness a week or more after an injection, and when mentioning soreness as a symptom, people will almost certainly specify it to be where they were injected, and if not, the person assessing them will ask. Many other studies beyond the Pfizer trials establish their effectiveness. These will be cited later on. The Qatari study is one sole study. The hazard ratios suggested natural immunity to more reliably prevent reinfection than vaccines, but not death. The results themselves could be skewed, as the populations most vulnerable to COVID will be less likely to have natural immunity, and more likely to die upon initial infection. You didn't even consider the risk to people's lives posed by COVID, becoming suspicious when the study's authors supported the utility of COVID vaccines in preventing COVID infection and death among the populace at large. This is because you don't care about people over the age of 50, or people who have conditions that increase their risk of dying of COVID. The study you cited about COVID vaccines and male fertility did not come close to meeting the burden of proof necessary to demonstrate that the vaccines harm male fertility. It was a single, small study, with if I recall correctly less than forty men. The confidence intervals and p values in the study suggested the vaccine to temporarily lower male fertility, but they did not establish the vaccines to have continued to worsen male fertility. You very clearly did not understand the utility of confidence intervals and p values, which are essential for establishing the veracity of a given hypothesis in studies of this sort, seeing as you never touched upon the very high levels of uncertainty, and even cropped the p values out of the screenshot displayed in the section. Because of your lack of understanding of the utility of p values and confidence intervals, you became very suspicious when the authors ultimately claimed that the vaccines didn't meaningfully harm male fertility, and supported vaccination. You cited some in vitro studies that suggested some herbal remedies to potentially treat COVID. A rational takeaway from these studies would be that these herbal remedies could treat COVID, not that they do. To establish whether they do or do not, clinical studies are necessary. But, I couldn't find any clinical studies. There are several reasons why in vitro studies of this sort do not prove a given thing to treat a given disease. Often, the primary reason is that the doses used in the in vitro study are not something an individual can feasibly obtain through dietary consumption. This was a potential issue with the herbal remedies you cited. You've also cited false information, which you've used to compound the false narratives that you've cast by misinterpreting information. Your section on the vaccines containing nanomachines is an outstanding example of this, though there's several smaller examples peppered about your article e.g Schiffman lying about kids dying from masks. The two individuals who conducted the study into vaccines and nanomachines were highly biased against vaccines, and were not qualified to conduct the study. This as a result put them in great risk of producing inaccurate results with their study. To this, you stated something along the lines of, "What do you really need to conduct a study of this kind? Some analytical thinking and microscopes is all it takes." which is so very far from the truth. If you have no idea what it is that you do and do not know, then you're not going to obtain accurate results from a study of this sort. Trained professionals will know what they do know, and what they do not know. These people weren't trained professionals. One of them was a linguist, the other was a physician. Both of them are linked to anti-vaccine institutions that publish pseudoscience. There is no chance that the vaccines contain self-assembling nanotechnology. If this were the case, we would have evidence outside of fringe studies conducted by anti-vaxxers. Every year, there are countless samples of biological materials extracted from humans, living and dead, which are examined under microscopes. This happens at hospitals and forensic sciences laboratories, among other places. If there was this epidemic of nanomachines within people's bodies, the evidence would be overwhelming, as countless people worldwide would report seeing them. This has of course not happened. The conspiracy is far too large to remain under control. Much of the false arguments you made likely came about through ad-hoc reasoning. You became, for whatever reason, convinced of some particular narrative, and began to seek evidence validating it. The fact that you've cited articles containing information which undermines your case, without addressing the conflicting information in said articles, suggests this. Once your arguments in favor of the pandemic being manufactured by a globe-spanning conspiracy are nullified, the misgivings of governments, corporations, and the media, lose the appearance of unusual malice. These institutions no doubt committed malicious acts for the sake of money and power, but this is a chronic, systemic issue. I won't be going over every single point you made in the article, much like I didn't with Wu's article that touched upon the Moon landings, because it would take forever and is unnecessary. I've opted to go over what I thought were the most significant points. This should be enough to dismantle the thesis of the article. I decided that it would be best to lump the evidence pertaining to vaccines up front, as they're one of the most significant aspects of the pandemic. Digdeeper then cites a news article from an Iraeli outlet.[103] For one, that's still more non-vaccinated being infected than vaccinated, implying that they did lower infectivity. This also does not consider how ill the vaccinated are. From a very surface-level analysis, it seems pointless. But if you consider the effect of vaccination on the severity of illness, things may change. He then cites a study from Qatari scientists.[104] It's an interesting finding as it goes against the common belief that the vaccines are ultimately better. However, it does not immediately mean that the vaccines are less effective. There could be some other factors contributing to the findings of their study. It may suggest that in their region, natural immunity was associated with better outcomes. It does not then nullify the findings of studies in completely different regions. As for what caused their findings to be different, I alone am not capable of determining that. You say "yet another", and yet, this is only the second of two morsels of evidence you've presented. Quoting the study: Look at the confidence intervals for reinfection (0·45–0·48, 0·49–0·54) versus severe, critical, or fatal COVID-19 cases (0·08–0·72, 0·05–1·19). The confidence intervals for reinfection are narrow, but for bad outcomes they are very broad. They do support the idea that natural infection can more reliably prevent COVID reinfection, perhaps more reliably than vaccination. They don't necessarily support the idea that those who have gotten COVID vaccines, when reinfected, have worse outcomes. The calculated risk was based on, in the authors' own words, a The authors deferred to vaccination being the optimal route of acquiring immunity in part due to the fact that: The findings of the study support the vaccines having a broad protective effect. There is much more consistent evidence to suggest that vaccines are superior to natural infection, which is part of the reason why the authors still supported the idea that vaccines are superior. One or two studies saying a particular thing are not definitive scientific evidence that something is absolutely one particular way. Here are various studies on the COVID vaccines which cover their safety, efficacy (in preventing infection, hospitalization, death) Full vaccination with moderna or pfizer vaccine was 88-96% effective in preventing COVID, partial vaccination was at least 77% effective.[105] The proportion of participants who had severe symptoms or were hospitalized was higher among unvaccinated case participants than among partially or completely vaccinated case participants. 83% effectiveness in preventing covid from 14-42 days, 62% effectiveness after 112-139 days. Effectiveness in prevention of hospitalization and mortality was 92% and 91% respectively at baseline, and reduced to 79% at 224-251 days for hospitalizations, and 86% at 168-195 days for mortality.[106] Two doses of moderna or pfizer vaccine 94-95% effective in preventing COVID 2 months after first dose, 66.6% and 80% after 7 months.[107] Vaccine effectiveness in preventing hospitalization and death at least 90% for all vaxes; in the prevention of infection, vaccination at least 83% effective (with the exclusion of CoronaVac which had lower effectiveness).[108] Notably, the analysis didn't identify a bunch of people who took the vaccine dying, out of the hundreds of thousands of people in the studies they analyzed.[109] Moderna vaccine 94.1% effective at preventing covid, including severe disease. No safety concerns identified out of over ten thousand people.[112] Vaccine had 66.9% effectiveness in preventing onset of moderate to severe covid at least 14 days after injection, 66.1% effective at least 28 days after injection, in prevention of severe-critical covid 76.7% effective for at least 14 days, 85.4% effective for at least 28 days.[113] 3 deaths were seen in the vaccine group in the study. 16 deaths were seen in the placebo group. All deaths were ruled unrelated to trial interventions by investigators. One subject had a transverse sinus thrombosis with cerebral hemorrhage, unknown if they died. One subject got Guillain–Barré syndrome.
Confidence intervals for severe disease are fairly broad given the rarity of such cases. Pfizer vaccine 91% effective in prevention of covid up to 6 months. efficacy against severe disease was 96.7%. no reported deaths, out of tens of thousands of recipients.[114] Efficacy in preventing severe disease 98.2%, in preventing asymptomatic infection 14 days after second injection 63% effective. no reports of mass death among vax recipient out of 15k people.[115] This study identified signals relating to Gullaine Barre syndrome, transverse myelitis, among other things. Notably, it didn't find people dropping like flies from vaccines, despite observing 99 million people.[119] My main takeaways from these studies:
How could so many people be in on a moon hoax conspiracy?
First, not a lot of people needed to be in on it, only a few at the top. Most people working for any large organization do not know all the agendas and secrets that are going on. The whole project was very compartmentalized. Everyone was on a need to know basis, and assigned to do a specialized task. The parts and pieces they were working on could have been used for any classified project beyond their knowing. Only the few at the top would see the big picture and be privy to what's going on.
Second, large numbers of people can keep a secret. For example, the Manhattan Project that developed the Atomic Bomb involved over 100,000 people who all kept it a secret before it was publicized. And the Secret Soviet Space program, which has now been declassified, involved thousands of people who all kept it a secret as well. And as you might know, the CIA and NSA contain thousands of operatives and staff who all keep their agency's activities a secret. Large numbers of people can be controlled by fear of imprisonment, death, and guilt for betraying their associates. History has proven this, so it is possible.
The Manhattan Project
Secret Soviet Space program
CIA and NSA contain thousands of operatives and staff who all keep their agency's activities a secret
First, most people (including scientists) don't question things that they are told by their establishment
If you steal a million dollars and get away with it, what will happen next time? You will steal another million dollars or maybe more right? Well that?s the case with our government. They lied about going to the moon, and if they get away with it, they will continue to concoct bigger lies. But if the moon hoax is exposed, then they cannot get away with such grandiose lies anymore. People will begin holding their government accountable. That?s when real reform will occur. And that?s why exposing this moon hoax is so important.?
NASA faked the moon landing, stealing over a hundred billions dollars from the taxpayers and proving to themselves that scams on that level are viable.
COVID showed that the conspiracy goes quite deep, and can involve all kinds of institutions. I think the elites became somewhat overconfident here, and received a level of resistance they didn't expect.
Coronavirus scare and the blueprint for slavery
You've misinterpreted information, taking away from it false conclusions, and applying these conclusions towards a conspiratorial narrative, which had you accurately interpreted the information would not be arrived at. This can be seen with many scientific studies you cited, such as studies relating to COVID originating from a lab; the Pfizer trial study; the Qatari study pertaining to natural immunity and vaccination; the study pertaining to the impact of COVID vaccines on male fertility; in vitro studies concerning the ability of herbal remedies to treat COVID, among many other things that will be mentioned in the remainder of the article (e.g vitamins/micronutrient deficiencies and diseases like sepsis and HIV, vaccine effectiveness being what determines a vaccine to be a vaccine, impoverished countries and Belarus not being ravaged by COVID, etc). You misinterpreted a large amount of news articles and reporting as well. A fundamental instance of this is with Event 201, which is an event that effectively predicates the entire conspiratorial lens through which you analyze the pandemic.
Natural immunity versus the vaccine
Natural immunity is almost 7 times stronger than vaccine-induced immunity - so if you've already had COVID, it seems pointless to take the vaccine.
>According to a report by Israel's Channel 13, Health Ministry data on the wave of COVID outbreaks which began this May show that Israelis with immunity from natural infection were far less likely to become infected again in comparison to Israelis who only had immunity via vaccination.
>More than 7,700 new cases of the virus have been detected during the most recent wave starting in May, but just 72 of the confirmed cases were reported in people who were known to have been infected previously – that is, less than 1% of the new cases.
>With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
>By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.
UPDATE January 2023: hey, we have yet another study showing natural immunity is stronger:
>Methods
>We conducted two matched retrospective cohort studies that emulated target trials. Data were obtained from the national federated databases for COVID-19 vaccination, SARS-CoV-2 testing, and COVID-19-related hospitalisation and death between Feb 28, 2020 (pandemic onset in Qatar) and May 12, 2022. We matched individuals with a documented primary infection and no vaccination record (natural infection cohort) with individuals who had received two doses (primary series) of the same vaccine (BNT162b2-vaccinated or mRNA-1273-vaccinated cohorts) at the start of follow-up (90 days after the primary infection). Individuals were exact matched (1:1) by sex, 10-year age group, nationality, comorbidity count, and timing of primary infection or first-dose vaccination. Incidence of SARS-CoV-2 infection and COVID-19-related hospitalisation and death in the natural infection cohorts was compared with incidence in the vaccinated cohorts, using Cox proportional hazards regression models with adjustment for matching factors.>Findings
>Between Jan 5, 2021 (date of second-dose vaccine roll-out) and May 12, 2022, 104 500 individuals vaccinated with BNT162b2 and 61 955 individuals vaccinated with mRNA-1273 were matched to unvaccinated individuals with a documented primary infection. During follow-up, 7123 SARS-CoV-2 infections were recorded in the BNT162b2-vaccinated cohort and 3583 reinfections were recorded in the matched natural infection cohort. 4282 SARS-CoV-2 infections were recorded in the mRNA-1273-vaccinated cohort and 2301 reinfections were recorded in the matched natural infection cohort. The overall adjusted hazard ratio (HR) for SARS-CoV-2 infection was 0·47 (95% CI 0·45–0·48) after previous natural infection versus BNT162b2 vaccination, and 0·51 (0·49–0·54) after previous natural infection versus mRNA-1273 vaccination. The overall adjusted HR for severe (acute care hospitalisations), critical (intensive care unit hospitalisations), or fatal COVID-19 cases was 0·24 (0·08–0·72) after previous natural infection versus BNT162b2 vaccination, and 0·24 (0·05–1·19) after previous natural infection versus mRNA-1273 vaccination. Severe, critical, or fatal COVID-19 was rare in both the natural infection and vaccinated cohorts.>Interpretation
>Previous natural infection was associated with lower incidence of SARS-CoV-2 infection, regardless of the variant, than mRNA primary-series vaccination. Vaccination remains the safest and most optimal tool for protecting against infection and COVID-19-related hospitalisation and death, irrespective of previous infection status.>Implications of all the available evidence
>Although natural infection was associated with stronger protection against SARS-CoV-2 infection and COVID-19 disease than primary-series mRNA vaccination, vaccination remains the safest and most optimal tool for protection against infection and COVID-19-related hospitalisation and death. Natural infection can lead to COVID-19-related hospitalisation and death at the time of primary infection, and long COVID-19 after the infection, which are risks not present with vaccination. The rapid waning of protection of primary-series vaccination supports the need for scaling up of booster vaccination and development of more potent vaccines to mitigate the effect of emerging variants.rare
amount of people with severe COVID in both vaccinated and unvaccinated cohorts. This is what created these broad confidence intervals.Natural infection can lead to COVID-19-related hospitalisation and death at the time of primary infection, and long COVID-19 after the infection, which are risks not present with vaccination.
Covid vaccines lowering risk of hospitalization and death
>Effectiveness of mRNA Covid-19 Vaccine among U.S. Health Care Personnel
>Methods
>We conducted a test-negative case–control study involving health care personnel across 25 U.S. states. Cases were defined on the basis of a positive polymerase-chain-reaction (PCR) or antigen-based test for SARS-CoV-2 and at least one Covid-19–like symptom. Controls were defined on the basis of a negative PCR test for SARS-CoV-2, regardless of symptoms, and were matched to cases according to the week of the test date and site. Using conditional logistic regression with adjustment for age, race and ethnic group, underlying conditions, and exposures to persons with Covid-19, we estimated vaccine effectiveness for partial vaccination (assessed 14 days after receipt of the first dose through 6 days after receipt of the second dose) and complete vaccination (assessed ≥7 days after receipt of the second dose).
>Results
>The study included 1482 case participants and 3449 control participants. Vaccine effectiveness for partial vaccination was 77.6% (95% confidence interval [CI], 70.9 to 82.7) with the BNT162b2 vaccine (Pfizer–BioNTech) and 88.9% (95% CI, 78.7 to 94.2) with the mRNA-1273 vaccine (Moderna); for complete vaccination, vaccine effectiveness was 88.8% (95% CI, 84.6 to 91.8) and 96.3% (95% CI, 91.3 to 98.4), respectively. Vaccine effectiveness was similar in subgroups defined according to age (<50 years or ≥50 years), race and ethnic group, presence of underlying conditions, and level of patient contact. Estimates of vaccine effectiveness were lower during weeks 9 through 14 than during weeks 3 through 8 after receipt of the second dose, but confidence intervals overlapped widely.
>Conclusions
>The BNT162b2 and mRNA-1273 vaccines were highly effective under real-world conditions in preventing symptomatic Covid-19 in health care personnel, including those at risk for severe Covid-19 and those in racial and ethnic groups that have been disproportionately affected by the pandemic. (Funded by the Centers for Disease Control and Prevention.)
>Our study population included health care personnel who had been tested for SARS-CoV-2. Participants were enrolled from December 28, 2020 (2 weeks after the introduction of a Covid-19 vaccine), through May 19, 2021, at 33 sites across 25 U.S. states, representing more than 500,000 health care personnel (Table S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org). The majority (68%) of the participating facilities were acute care hospitals (with or without affiliated outpatient and urgent care clinics), and 32% were long-term care facilities. Covid-19 vaccines were introduced at the participating facilities in December 2020, and the vaccine coverage among health care personnel at these facilities reached 55 to 98% for the receipt of at least one dose of vaccine and 51 to 94% for the receipt of two vaccine doses during the study period.
>Information on the participants’ demographic characteristics, symptoms of Covid-19–like illness, underlying conditions and risk factors associated with severe Covid-19,15 and medical care received was collected by means of interviews or participant-completed surveys. The interviews and surveys also included information on potential confounders related to workplace and community behaviors. Medical records were reviewed in order to collect information about the SARS-CoV-2 test, including the date, test type, and result, and about the medical care sought during the Covid-19–like illness. Information on Covid-19 vaccination dates and products received was obtained from occupational health clinics, vaccine cards, state registries, or medical records.
>In the final model, we adjusted for age, race and ethnic group, presence of at least one underlying condition or risk factor for severe Covid-19, and close contact with patients with Covid-19 in the workplace or with persons with Covid-19 outside the workplace. We evaluated vaccine effectiveness according to vaccine product and in subgroups defined according to participants’ age (<50 years or ≥50 years), race and ethnic group, presence of underlying conditions, health care job categories, and clinical case definitions that were consistent with those used in the clinical trials. We examined the adjusted vaccine effectiveness according to 2-week intervals of follow-up after receipt of the second dose (as compared with unvaccinated participants) to assess for waning of vaccine effect. All the statistical analyses were conducted with the use of SAS software, version 9.4 (SAS Institute).
>During the study period of December 28, 2020, through May 19, 2021, a total of 109,865 health care personnel were tested across the participating sites; of these persons, 8365 (7.6%) tested positive for SARS-CoV-2. A total of 1482 participants with a positive test and at least one Covid-19–like symptom (cases) and 3449 with a negative test (controls) were enrolled. Among the enrolled health care personnel, 69% worked at acute care hospitals (including emergency departments), 31% in outpatient or specialty clinics, 1% in urgent care clinics, and 1% in long-term care facilities.
>The characteristics of the enrolled participants are shown in Table 1 and Table 2. More than three quarters of the participants (76% of the cases and 75% of the controls) reported having at least one underlying condition associated with an increased risk of severe Covid-19, and no differences were noted in the distribution of individual conditions or risk factors between cases and controls, with the exception of obesity (more common among case participants) and asthma (more common among control participants) (Table S2). We identified 62 cases among pregnant women; the median gestational age at the time of the index test date was 23 weeks (range, 3 to 41). The most common underlying conditions were obesity (in 36% of the case participants and in 31% of the control participants), overweight (in 29% and 28%, respectively), asthma (in 14% and 18%), and hypertension (in 15% and 14%). Only 2% of case participants were hospitalized during their illness; 1% of control participants were hospitalized during a non–Covid-19–related illness. No deaths were reported among the participants included in this study.
>We identified 167 cases among completely vaccinated participants and 140 cases among partially vaccinated participants
Covid vaccines lowering risk of hospitalization and death
>Long-term effectiveness of COVID-19 vaccines against infections, hospitalisations, and mortality in adults: findings from a rapid living systematic evidence synthesis and meta-analysis up to December, 2022
>Methods
>In this rapid living systematic evidence synthesis and meta-analysis, we searched EMBASE and the US National Institutes of Health's iSearch COVID-19 Portfolio, supplemented by manual searches of COVID-19-specific sources, until Dec 1, 2022, for studies that reported vaccine effectiveness immediately and at least 112 days after a primary vaccine series or at least 84 days after a booster dose. Single reviewers assessed titles, abstracts, and full-text articles, and extracted data, with a second reviewer verifying included studies. The primary outcomes were vaccine effectiveness against SARS-CoV-2 infections, hospitalisations, and mortality, which were assessed using three-level meta-analytic models. This study is registered with the National Collaborating Centre for Methods and Tools, review 473.
>Findings
>We screened 16 696 records at the title and abstract level, appraised 832 (5·0%) full texts, and initially included 73 (0·4%) studies. Of these, we excluded five (7%) studies because of critical risk of bias, leaving 68 (93%) studies that were extracted for analysis. For infections caused by any SARS-CoV-2 strain, vaccine effectiveness for the primary series reduced from 83% (95% CI 80–86) at baseline (14–42 days) to 62% (53–69) by 112–139 days. Vaccine effectiveness at baseline was 92% (88–94) for hospitalisations and 91% (85–95) for mortality, and reduced to 79% (65–87) at 224–251 days for hospitalisations and 86% (73–93) at 168–195 days for mortality. Estimated vaccine effectiveness was lower for the omicron variant for infections, hospitalisations, and mortality at baseline compared with that of other variants, but subsequent reductions occurred at a similar rate across variants. For booster doses, which covered mostly omicron studies, vaccine effectiveness at baseline was 70% (56–80) against infections and 89% (82–93) against hospitalisations, and reduced to 43% (14–62) against infections and 71% (51–83) against hospitalisations at 112 days or later. Not enough studies were available to report on booster vaccine effectiveness against mortality.
...
>We found that the vaccine effectiveness of the primary vaccine series against SARS-CoV-2 infections begins at an adequate level, as defined by WHO, of 83% at 14–42 days after series completion; however, vaccine effectiveness decreased significantly by 112 days after vaccination, reaching 47% by 280 days after vaccination, well below an adequate level. For COVID-19 hospitalisations and mortality, vaccine effectiveness levels were also adequate at baseline (>90%), but similarly reduced 112 days after vaccination; although, vaccine effectiveness remained high over time (>75%). When looking at omicron-only data, we found similar waning patterns, except that baseline levels of vaccine effectiveness did not reach adequate levels for infections or hospitalisations. What might be driving these omicron patterns is unclear—eg, whether a degradation in immunogenicity, changes in public health measures, variations in case numbers and general transmission, or a combination of all these. Although boosters might be promising at re-establishing some protection, our results found that the vaccine effectiveness of boosters at baseline (7–28 days after receiving the booster) were still, albeit by a small margin, below the WHO's recommended levels and in the long term, these numbers reduced further. Our booster-dose estimates predominately represent mRNA vaccines against omicron, which reflects the situation in many countries. Collectively, these data suggest that vaccines are providing reasonably stable protection against hospitalisations and mortality over the long term, but that protection against infections is more modest.
Covid vaccines lowering risk of hospitalization and death
>Effectiveness of Covid-19 Vaccines over a 9-Month Period in North Carolina
>Methods
>We extracted data regarding Covid-19–related vaccination and outcomes during a 9-month period (December 11, 2020, to September 8, 2021) for approximately 10.6 million North Carolina residents by linking data from the North Carolina Covid-19 Surveillance System and the Covid-19 Vaccine Management System. We used a Cox regression model to estimate the effectiveness of the BNT162b2 (Pfizer–BioNTech), mRNA-1273 (Moderna), and Ad26.COV2.S (Johnson & Johnson–Janssen) vaccines in reducing the current risks of Covid-19, hospitalization, and death, as a function of time elapsed since vaccination.
>Results
>For the two-dose regimens of messenger RNA (mRNA) vaccines BNT162b2 (30 μg per dose) and mRNA-1273 (100 μg per dose), vaccine effectiveness against Covid-19 was 94.5% (95% confidence interval [CI], 94.1 to 94.9) and 95.9% (95% CI, 95.5 to 96.2), respectively, at 2 months after the first dose and decreased to 66.6% (95% CI, 65.2 to 67.8) and 80.3% (95% CI, 79.3 to 81.2), respectively, at 7 months. Among early recipients of BNT162b2 and mRNA-1273, effectiveness decreased by approximately 15 and 10 percentage points, respectively, from mid-June to mid-July, when the delta variant became dominant. For the one-dose regimen of Ad26.COV2.S (5×1010 viral particles), effectiveness against Covid-19 was 74.8% (95% CI, 72.5 to 76.9) at 1 month and decreased to 59.4% (95% CI, 57.2 to 61.5) at 5 months. All three vaccines maintained better effectiveness in preventing hospitalization and death than in preventing infection over time, although the two mRNA vaccines provided higher levels of protection than Ad26.COV2.S.
>Conclusions
>All three Covid-19 vaccines had durable effectiveness in reducing the risks of hospitalization and death. Waning protection against infection over time was due to both declining immunity and the emergence of the delta variant. (Funded by a Dennis Gillings Distinguished Professorship and the National Institutes of Health.)
Covid vaccines lowering risk of hospitalization and death
>Real-world effectiveness of COVID-19 vaccines: a literature review and meta-analysis
>Objective
>To estimate the coronavirus disease 2019 (COVID-19) vaccine effectiveness (VE) against concerned outcomes in real-world settings.
>Methods
>Studies reporting COVID-19 VE from August 6, 2020 to October 6, 2021 were included. The summary VE (with 95% confidence intervals (95% CI)) against disease related to COVID-19 was estimated. The results were presented in forest plots. Predefined subgroup analyses and sensitivity analyses were also performed.
>Results
>... In fully vaccinated populations, the VE against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, COVID-19-related hospitalization, admission to the intensive care unit, and death was 89.1% (95% CI 85.6–92.6%), 97.2% (95% CI 96.1–98.3%), 97.4% (95% CI 96.0–98.8%), and 99.0% (95% CI 98.5–99.6%), respectively. The VE against infection in the general population aged ≥16 years, the elderly, and healthcare workers was 86.1% (95% CI 77.8–94.4%), 83.8% (95% CI 77.1–90.6%), and 95.3% (95% CI 92.0–98.6%), respectively. For those fully vaccinated against infection, the observed effectiveness of the Pfizer-BioNTech vaccine was 91.2% and of the Moderna vaccine was 98.1%, while the effectiveness of the CoronaVac vaccine was found to be 65.7%.
Safety and immunogenicity
>Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis
>This study analyzed the efficacy of COVID-19 vaccines. Published phase I, phase II, and phase III trials analyzing safety and immunogenicity and phase III randomized clinical trials evaluating the efficacy of COVID-19 vaccines were included. We searched MEDLINE, Scopus, and The Lancet for published articles evaluating the relative reduction in COVID-19 risk after vaccination. Selected literatures were published between December 15, 2019 and May 15, 2021 on the safety, efficacy, and immunogenicity of COVID-19 vaccines. This meta-analysis included studies that confirmed cases of COVID-19 using reverse transcriptase polymerase chain reaction. This study detected 8,926 eligible research articles published on COVID-19 vaccines. Of these, 25 studies fulfilled the inclusion criteria. Among the selected articles, 19 randomized clinical trials, 2 non-randomized clinical trials, and 3 observational studies were analyzed. Seven (28%) studies were included in the meta-analysis. The efficacy of the adenovirus vector vaccine was 73% (95% CI = 69–77) and that of the messenger RNA (mRNA) vaccine was 85% (95% CI = 82–88) in participants aged ≥18 years. There are no reports of clinical trials in participants aged under 16 years. The production of neutralizing antibodies against receptor-binding domains (RBDs) of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in >90% of the vaccinated samples was reported within 0–30 days of the first or the second dose of the vaccine. Pain at the injection site was the most common local symptom in people receiving mRNA vaccines (29%–85% of participants). Fever (0.2%–95%) was the most prevalent in people receiving adenovirus vector vaccines, and fatigue (8.4%–55%) was the most common side effect in people receiving the mRNA vaccines. Studies suggest that mRNA vaccines and adenovirus vector vaccines can provide moderate to high protection against COVID-19 infection in people over 18 years. Evidence of the long-term protection of the vaccines in people aged under 16 years against the multiple variants of COVID-19 are limited. This study will provide an integrated evaluation on the efficacy, safety, and immunogenicity of the COVID-19 vaccines.
Immunogenicity of the COVID-19 Vaccines
>Following the inclusion criteria, 12 published studies on the immunogenicity of COVID-19 vaccines were included in this systematic review article. These studies reported successful production of antibodies against the RBDs of SARS-CoV-2 in about >90% of vaccinated study participants. The ability of the COVID-19 vaccines to induce T-cell-mediated immunity among participants was also assessed ( Table 3 ). The COVID-19 vaccines, including the non-replicating adenovirus type 5 (Ad5)-vectored vaccine, BNT162b1, Gam-COVID-Vac, mRNA-1273, and NVX-CoV2373, had the capability to induce the immune system to producing from 102 to ≤103 T cells per 1 × 105 peripheral blood mononuclear cells (PBMCs) in the vaccinated population in the first 28 days after vaccination. The safe and effective dose concentrations differed depending on the vaccine type. Among 12 studies, four (33.3%) were on the adenovirus vector vaccine, four (33.3%) were on the mRNA vaccine, two (16.7%) were on the inactivated vaccine, and two studies (16.7%) were on the subunit vaccine. The time it took for vaccine recipients to achieve effective seroconversion varied depending on the vaccine type and the dose concentrations ( Table 3 ). Studies on the adenovirus vector vaccine reported that about 1010–1011 virus particles successfully stimulated the production of neutralizing antibody against RBDs within 0–28 days after vaccination (16–20). Furthermore, studies on the mRNA vaccines found that 25–30 μg doses were able to induce neutralizing antibody production in individuals within 0–28 days after vaccination (21, 23, 26, 36). One study on the subunit vaccine in Australia reported that about 99% (67 of 68) of participants receiving two doses developed neutralizing antibodies within 57 days (29). Another study on the recombinant spike protein nanoparticle vaccine (NVX-CoV2373) also reported that the vaccine was able to induce anti-spike immunoglobulin G (IgG) and neutralization response in vaccinated participants within 28 days after vaccination (22).
Safety of COVID-19 Vaccines
>Among the studies on the safety of the COVID-19 vaccines, five were on the adenovirus vector vaccine, six were on the mRNA vaccine, two were on the subunit vaccine, and three studies were on the inactivated vaccine ( Table 4 ). Local effects including pain, redness, and swelling at the vaccination site and systemic effects such as fever, fatigue, headache, chill, vomiting, diarrhea, nausea, and arthralgia were reported as the side effects of COVID-19 vaccination (16–20, 23, 28, 37). Pain at the injection site was the most common local symptom in the mRNA (29%–85% of participants) and adenovirus vector (0.2%–78% participants) vaccines. Fever (0.2%–95%), fatigue (1%–55%), and headache (0.7%–68%) were the most commonly reported symptoms among those who received adenovirus vector vaccines, whereas fatigue (8.4%–55%) was the most common in those who received mRNA vaccines. Fatigue (30%–40%) and headache (15%–40%) were the most common symptoms among those who received subunit vaccines (21, 22, 24, 27–29, 33–35, 40, 42). According to one adenovirus vector vaccine research, 8% (20 of 253) of those who received the immunization had grade 3 fever (19). Four percent (5,994 of 14,985) of participants in a study had grade 3 pain at the injection site, while 8% (11,988 of 14,985) of participants in a trial reported grade 3 fatigue after receiving the mRNA vaccine (40). In these studies, no deaths associated with COVID-19 vaccines were documented. Furthermore, the published works reported very low frequency of grade 3 and grade 4 local and systematic symptoms in vaccinated participants (21, 22, 24, 27–29, 33–35, 40, 43).
Covid vaccines halved the risk of severe covid, and reinfection, compared to natural immunity [110]
>COVID-19 vaccines reduce the risk of SARS-CoV-2 reinfection and hospitalization: Meta-analysis
>This meta-analysis, which included the data of more than 18 million previously infected and recovered subjects, has two main findings. First, as compared to natural immunity alone, the addition of vaccination approximately halved the odds of severe COVID-19, and the degree of protection was similar after a single or multiple doses. Second, the likelihood of reinfection was also reduced by approximately 50% among the vaccinated, and this finding was consistent in all stratified analyses, either extracting estimates adjusted for potential confounders or unadjusted, with follow-ups shorter or longer than 6 months, adopting different reinfection definitions, in both case-control and cohort studies, in the general population and healthcare workers alone, after a single or multiple vaccine doses, and irrespective of the predominant strain.
>Preliminary evidence suggested that the protection conferred by hybrid immunity against reinfection was similar, or only marginally better, than the infection-induced or vaccine-induced immunity alone (5, 35). More recently, however, a proportion meta-analysis including 15 million previously infected and recovered individuals reported markedly lower rates of reinfection among vaccinated vs. unvaccinated subjects (0.32% vs. 0.74%), but these findings were based upon raw data and needed confirmation from adjusted estimates (2). The present meta-analysis expanded the previous and included 15 studies that adjusted the analyses for age, gender, comorbidities, and other potential confounders, providing solid evidence of a stronger protection of hybrid vs. natural immunity, which may persist during Omicron waves and up to 12 months.
>Indeed, concerning the waning of the immunity, a 20% decline in the effectiveness of vaccination against first infection after 6 months was first showed in a meta-analysis including studies up to December 2021 (36). Then, evidence of waning protection both with hybrid and natural immunity 4 months after immunization was reported in some large prospective studies, which showed corresponding upward trends in reinfection absolute rates during time (5, 8, 9). In the present meta-analysis, the reinfection rates of the cohort studies with follow-up longer than 6 months were not distinctly higher (0.17 and 0.65 × 100 individuals in vaccinated and unvaccinated subjects, respectively), as compared to those with short follow-up (0.39 and 0.50 × 100 individuals in vaccinated and unvaccinated subjects, respectively). Additionally, we did not observe a substantial reduction of the protection when the follow-up lasted 6–11 months: pooling the 12 datasets with a longer follow-up, the odds of reinfection were approximately 50% lower among the vaccinated. Inevitably, this information remains preliminary, as it is based upon studies in which the follow-up lasted up to 12 months, and the use of viral genomic sequencing was uneven.
Covid vaccines lowering risk of infection, severe disease, and death [111]
>Pfizer-BioNTech vaccine effectiveness against Sars-Cov-2 infection: Findings from a large observational study in Israel
>In this study of over 1.6 million participants, Pfizer-BioNTech VE for infection adjusted for gender, age, hypertension, diabetes and obesity and conditioned on GSA and calendar week was 93% (CI:92.6–93.4). Based on an average follow-up period of 63 days for the two-dose vaccinated population and 40 days for those not vaccinated, the infection rates found here are slightly lower than those reported in the original Pfizer RCT (95% (CI: 90.3–97.6) with an average of 2 months follow-up) (Polack et al., 2020) but comparable with those of Clalit, another HMO in Israel (92% (CI: 88–95) with a maximum 15 day follow-up) (Dagan et al., 2021) and national data (94.1%, CI: 93.4–94.7) (Haas et al., 2021).
>Adjusted VE for hospitalization in this study was 93.4% (CI:91.9%–94.7%). The Clalit study (Dagan et al., 2021) reported lower adjusted VE point estimates for hospitalization (87%, CI: 55%–100%). We suggest that the Clalit data under-estimate VE for hospitalization as a result of the small number of cases in the short time period available for analysis. National data (Haas et al., 2021), adjusted for age, gender and calendar week with a maximum follow-up period of 41 days reported a higher VE for hospitalization (96.2%, CI: 95.5–96.8) than the present study. We suggest that the inclusion of GSA in our model for adjustment of exposure, controlling for chronic illness conditions and the longer follow-up period, provides a more accurate estimate of VE for hospitalization.
>Adjusted VE for mortality in this study was 91.1% (CI: 86.5%–94.1%). The initial Pfizer RCT (Polack et al., 2020) reported six deaths (two in the intervention group and four in the control group) but deemed all deaths to be unrelated to the vaccine. We have been able to present here mortality data that is illness-specific that perhaps reflects a more realistic assessment of mortality risk. In the national study (Haas et al., 2021), VE rates reported for mortality were slightly higher (93.3%, CI: 91.5–94.8) than those reported here. Clalit reported adjusted VE for severe disease (defined as severe disease or death) as 92%(CI:75%–100%) (Dagan et al., 2021).
>The elderly population are at higher risk of morbidity and mortality from Sars-Cov-2 infection (Salzberger et al., 2021) and one of the greatest concerns regarding the vaccine is that it would be less effective in the elderly population (Soiza et al., 2021). We found that adjusted VE for infection was in fact lower in the 75+ age group (81%) than for those under age 75 (90 + %), with a VE for infection of 89% (CI: 83%–93%) for those aged 70 and over. Dagan et al., 20219 reported adjusted VE rates for infection of 95% (CI:87%–100%) for the 70+ age group. Their study excluded members from nursing homes, the homebound and those presenting to the healthcare system within three days. These groups were not excluded in this study. Inclusion of these population groups, and the longer follow-up period eight-plus days post- second vaccination may account for the lower VE for infection in this study.
>Hypertension (Tadic et al., 2020), diabetes (Peric and Stulnig, 2020) and obesity (Zhou et al., 2021) have all been established as risk factors for Sars-Cov-2 infection. Independent of age, we wished to determine if VE was lower for these conditions. It has been suggested that both Covid-19 infection and mRNA-based vaccines promote an ACE2 platelet receptor imbalance (Angeli et al., 2021) and poorer sero-conversion in these population groups (Watanabe et al., 2021). We found that presence of any of these conditions is accompanied by a lower adjusted VE for infection. Adjusted VE rates for infection for participants with these conditions in this study were consistently lower here than those reported by Dagan et al. (2021) (Dagan et al., 2021) (hypertension: 89.7% vs 93%, diabetes: 88.9% vs 91%, obesity: 89.7% vs 95%). Again, we suggest that our data reflect general population VE, given the minimal exclusion criteria.
Covid vaccines lowering risk of infection and severe disease
>Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine
>Methods
>This phase 3 randomized, observer-blinded, placebo-controlled trial was conducted at 99 centers across the United States. Persons at high risk for SARS-CoV-2 infection or its complications were randomly assigned in a 1:1 ratio to receive two intramuscular injections of mRNA-1273 (100 μg) or placebo 28 days apart. The primary end point was prevention of Covid-19 illness with onset at least 14 days after the second injection in participants who had not previously been infected with SARS-CoV-2.
>Results
>The trial enrolled 30,420 volunteers who were randomly assigned in a 1:1 ratio to receive either vaccine or placebo (15,210 participants in each group). More than 96% of participants received both injections, and 2.2% had evidence (serologic, virologic, or both) of SARS-CoV-2 infection at baseline. Symptomatic Covid-19 illness was confirmed in 185 participants in the placebo group (56.5 per 1000 person-years; 95% confidence interval [CI], 48.7 to 65.3) and in 11 participants in the mRNA-1273 group (3.3 per 1000 person-years; 95% CI, 1.7 to 6.0); vaccine efficacy was 94.1% (95% CI, 89.3 to 96.8%; P<0.001). Efficacy was similar across key secondary analyses, including assessment 14 days after the first dose, analyses that included participants who had evidence of SARS-CoV-2 infection at baseline, and analyses in participants 65 years of age or older. Severe Covid-19 occurred in 30 participants, with one fatality; all 30 were in the placebo group. Moderate, transient reactogenicity after vaccination occurred more frequently in the mRNA-1273 group. Serious adverse events were rare, and the incidence was similar in the two groups.
>Conclusions
>The mRNA-1273 vaccine showed 94.1% efficacy at preventing Covid-19 illness, including severe disease. Aside from transient local and systemic reactions, no safety concerns were identified. (Funded by the Biomedical Advanced Research and Development Authority and the National Institute of Allergy and Infectious Diseases; COVE ClinicalTrials.gov number, NCT04470427.)
Covid vaccines lowering risk of infection and severe disease
>Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19
>Methods
>In an international, randomized, double-blind, placebo-controlled, phase 3 trial, we randomly assigned adult participants in a 1:1 ratio to receive a single dose of Ad26.COV2.S (5×1010 viral particles) or placebo. The primary end points were vaccine efficacy against moderate to severe–critical coronavirus disease 2019 (Covid-19) with an onset at least 14 days and at least 28 days after administration among participants in the per-protocol population who had tested negative for SARS-CoV-2. Safety was also assessed.
>Results
>The per-protocol population included 19,630 SARS-CoV-2–negative participants who received Ad26.COV2.S and 19,691 who received placebo. Ad26.COV2.S protected against moderate to severe–critical Covid-19 with onset at least 14 days after administration (116 cases in the vaccine group vs. 348 in the placebo group; efficacy, 66.9%; adjusted 95% confidence interval [CI], 59.0 to 73.4) and at least 28 days after administration (66 vs. 193 cases; efficacy, 66.1%; adjusted 95% CI, 55.0 to 74.8). Vaccine efficacy was higher against severe–critical Covid-19 (76.7% [adjusted 95% CI, 54.6 to 89.1] for onset at ≥14 days and 85.4% [adjusted 95% CI, 54.2 to 96.9] for onset at ≥28 days). Despite 86 of 91 cases (94.5%) in South Africa with sequenced virus having the 20H/501Y.V2 variant, vaccine efficacy was 52.0% and 64.0% against moderate to severe–critical Covid-19 with onset at least 14 days and at least 28 days after administration, respectively, and efficacy against severe–critical Covid-19 was 73.1% and 81.7%, respectively. Reactogenicity was higher with Ad26.COV2.S than with placebo but was generally mild to moderate and transient. The incidence of serious adverse events was balanced between the two groups. Three deaths occurred in the vaccine group (none were Covid-19–related), and 16 in the placebo group (5 were Covid-19–related).
>Conclusions
>A single dose of Ad26.COV2.S protected against symptomatic Covid-19 and asymptomatic SARS-CoV-2 infection and was effective against severe–critical disease, including hospitalization and death. Safety appeared to be similar to that in other phase 3 trials of Covid-19 vaccines. (Funded by Janssen Research and Development and others; ENSEMBLE ClinicalTrials.gov number, NCT04505722.)
Covid vaccines lowering risk of infection
>Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months
>Methods
>In an ongoing, placebo-controlled, observer-blinded, multinational, pivotal efficacy trial, we randomly assigned 44,165 participants 16 years of age or older and 2264 participants 12 to 15 years of age to receive two 30-μg doses, at 21 days apart, of BNT162b2 or placebo. The trial end points were vaccine efficacy against laboratory-confirmed Covid-19 and safety, which were both evaluated through 6 months after vaccination.
>Results
>BNT162b2 continued to be safe and have an acceptable adverse-event profile. Few participants had adverse events leading to withdrawal from the trial. Vaccine efficacy against Covid-19 was 91.3% (95% confidence interval [CI], 89.0 to 93.2) through 6 months of follow-up among the participants without evidence of previous SARS-CoV-2 infection who could be evaluated. There was a gradual decline in vaccine efficacy. Vaccine efficacy of 86 to 100% was seen across countries and in populations with diverse ages, sexes, race or ethnic groups, and risk factors for Covid-19 among participants without evidence of previous infection with SARS-CoV-2. Vaccine efficacy against severe disease was 96.7% (95% CI, 80.3 to 99.9). In South Africa, where the SARS-CoV-2 variant of concern B.1.351 (or beta) was predominant, a vaccine efficacy of 100% (95% CI, 53.5 to 100) was observed.
Covid vaccines lowering risk of infection and severe disease
>Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase
>Methods
>We enrolled volunteers who were at high risk for Covid-19 or its complications; participants were randomly assigned in a 1:1 ratio to receive two intramuscular injections of mRNA-1273 (100 μg) or placebo, 28 days apart, at 99 centers across the United States. The primary end point was prevention of Covid-19 illness with onset at least 14 days after the second injection in participants who had not previously been infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The data cutoff date was March 26, 2021.
>Results
>The trial enrolled 30,415 participants; 15,209 were assigned to receive the mRNA-1273 vaccine, and 15,206 to receive placebo. More than 96% of participants received both injections, 2.3% had evidence of SARS-CoV-2 infection at baseline, and the median follow-up was 5.3 months in the blinded phase. Vaccine efficacy in preventing Covid-19 illness was 93.2% (95% confidence interval [CI], 91.0 to 94.8), with 55 confirmed cases in the mRNA-1273 group (9.6 per 1000 person-years; 95% CI, 7.2 to 12.5) and 744 in the placebo group (136.6 per 1000 person-years; 95% CI, 127.0 to 146.8). The efficacy in preventing severe disease was 98.2% (95% CI, 92.8 to 99.6), with 2 cases in the mRNA-1273 group and 106 in the placebo group, and the efficacy in preventing asymptomatic infection starting 14 days after the second injection was 63.0% (95% CI, 56.6 to 68.5), with 214 cases in the mRNA-1273 group and 498 in the placebo group. Vaccine efficacy was consistent across ethnic and racial groups, age groups, and participants with coexisting conditions. No safety concerns were identified.
>Conclusions
>The mRNA-1273 vaccine continued to be efficacious in preventing Covid-19 illness and severe disease at more than 5 months, with an acceptable safety profile, and protection against asymptomatic infection was observed. (Funded by the Biomedical Advanced Research and Development Authority and the National Institute of Allergy and Infectious Diseases; COVE ClinicalTrials.gov number, NCT04470427.)
Covid vaccines lowering risk of infection[116]
>Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine
>Methods
>In an ongoing multinational, placebo-controlled, observer-blinded, pivotal efficacy trial, we randomly assigned persons 16 years of age or older in a 1:1 ratio to receive two doses, 21 days apart, of either placebo or the BNT162b2 vaccine candidate (30 μg per dose). BNT162b2 is a lipid nanoparticle–formulated, nucleoside-modified RNA vaccine that encodes a prefusion stabilized, membrane-anchored SARS-CoV-2 full-length spike protein. The primary end points were efficacy of the vaccine against laboratory-confirmed Covid-19 and safety.
>Results
>A total of 43,548 participants underwent randomization, of whom 43,448 received injections: 21,720 with BNT162b2 and 21,728 with placebo. There were 8 cases of Covid-19 with onset at least 7 days after the second dose among participants assigned to receive BNT162b2 and 162 cases among those assigned to placebo; BNT162b2 was 95% effective in preventing Covid-19 (95% credible interval, 90.3 to 97.6). Similar vaccine efficacy (generally 90 to 100%) was observed across subgroups defined by age, sex, race, ethnicity, baseline body-mass index, and the presence of coexisting conditions. Among 10 cases of severe Covid-19 with onset after the first dose, 9 occurred in placebo recipients and 1 in a BNT162b2 recipient. The safety profile of BNT162b2 was characterized by short-term, mild-to-moderate pain at the injection site, fatigue, and headache. The incidence of serious adverse events was low and was similar in the vaccine and placebo groups.
>Conclusions
>A two-dose regimen of BNT162b2 conferred 95% protection against Covid-19 in persons 16 years of age or older. Safety over a median of 2 months was similar to that of other viral vaccines. (Funded by BioNTech and Pfizer; ClinicalTrials.gov number, NCT04368728.)
Unvaccinated patients 2.46 times more likely to die from COVID than vaccinated [117]
>Unveiling the Impact of COVID-19 Vaccines: A Meta-Analysis of Survival Rates Among Patients in the United States Based on Vaccination Status
>The COVID-19 pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in a significant number of cases and deaths worldwide. Vaccination is the most effective preventive measure against the disease. This study aimed to assess the mortality rates of COVID-19 patients in the United States and the effectiveness of Pfizer (Pfizer, NY, USA), Moderna (Moderna, MA, USA), and Janssen (Johnson & Johnson, NJ, USA) vaccines in preventing mortality.
>A systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA-2020) guidelines. Eligible studies reporting on the effectiveness of COVID-19 vaccines on patient outcomes were included. The search was performed in PubMed, Cochrane, and Google Scholar databases. The data were extracted, and risk ratios (RR) were calculated for mortality outcomes. The analysis was performed using Review Manager software, and bias assessments were conducted using the Joanna Briggs Institute (JBI) Meta-Analysis tools.
>A total of seven studies with 21,618,297 COVID-19 patients were included in the meta-analysis. The odds ratio (OR) for mortality among unvaccinated patients compared to vaccinated patients was 2.46 (95% CI: 1.71-3.53), indicating that unvaccinated patients were 2.46 times more likely to die from COVID-19.
>The findings of this study support the effectiveness of COVID-19 vaccination in reducing mortality among infected individuals. Unvaccinated patients had a significantly higher risk of mortality compared to vaccinated patients. Vaccination remains a crucial strategy to mitigate the severity of the disease and reduce mortality rates. Efforts should be made to address vaccine hesitancy and ensure widespread vaccine coverage.
Unvaccinated died at 14 times the rate of bivalent vaccinated, and 5 times the rate of monovalent vaccinated [118]
>On September 1, 2022, CDC recommended an updated (bivalent) COVID-19 vaccine booster to help restore waning protection conferred by previous vaccination and broaden protection against emerging variants for persons aged ≥12 years (subsequently extended to persons aged ≥6 months).* To assess the impact of original (monovalent) COVID-19 vaccines and bivalent boosters, case and mortality rate ratios (RRs) were estimated comparing unvaccinated and vaccinated persons aged ≥12 years by overall receipt of and by time since booster vaccination (monovalent or bivalent) during Delta variant and Omicron sublineage (BA.1, BA.2, early BA.4/BA.5, and late BA.4/BA.5) predominance.† During the late BA.4/BA.5 period, unvaccinated persons had higher COVID-19 mortality and infection rates than persons receiving bivalent doses (mortality RR = 14.1 and infection RR = 2.8) and to a lesser extent persons vaccinated with only monovalent doses (mortality RR = 5.4 and infection RR = 2.5). Among older adults, mortality rates among unvaccinated persons were significantly higher than among those who had received a bivalent booster (65–79 years; RR = 23.7 and ≥80 years; 10.3) or a monovalent booster (65–79 years; 8.3 and ≥80 years; 4.2). In a second analysis stratified by time since booster vaccination, there was a progressive decline from the Delta period (RR = 50.7) to the early BA.4/BA.5 period (7.4) in relative COVID-19 mortality rates among unvaccinated persons compared with persons receiving who had received a monovalent booster within 2 weeks–2 months. During the early BA.4/BA.5 period, declines in relative mortality rates were observed at 6–8 (RR = 4.6), 9–11 (4.5), and ≥12 (2.5) months after receiving a monovalent booster. In contrast, bivalent boosters received during the preceding 2 weeks–2 months improved protection against death (RR = 15.2) during the late BA.4/BA.5 period. In both analyses, when compared with unvaccinated persons, persons who had received bivalent boosters were provided additional protection against death over monovalent doses or monovalent boosters. Restored protection was highest in older adults. All persons should stay up to date with COVID-19 vaccination, including receipt of a bivalent booster by eligible persons, to reduce the risk for severe COVID-19.
>COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals
I actually decided to see if there's been a determination made as to how many people probably died from the COVID vaccines, and research has been conducted into this. I'll go over this shortly.
Natural immunity can still suffice to prevent future infection, but it is not categorically superior to vaccine-induced immunity. Vaccination was shown to prevent future infection, hospitalization, and mortality with greater consistency than natural immunity. One must also take on the risks associated with infection in order to develop natural immunity. If one is vaccinated, they can lower their risk of infection in the future while taking on fewer health risks.
You may demand that the vaccines prevent COVID with 100% consistency in order to be deemed effective, but your demands are unrealistic and based in ignorance; we'll be going over this.
I was bored one evening and checked out statistics from the CDC pertaining to America. What I found will shock you to your core. My entire thesis had to be changed. If you're standing, you had best sit down ASAP.
I looked at deaths from diseases of the heart and cerebrovascular disease from 2010 to 2024. I stripped them down to their raw numbers for this display.
2010[120]
Diseases of heart 597,689
Cerebrovascular diseases 129,476
2011[121]
Diseases of heart 596,339
Cerebrovascular diseases 128,931
2012[121]
Diseases of heart 596,339
Cerebrovascular diseases 128,931
2013[122]
Diseases of heart 611,105
Cerebrovascular diseases 128,978
2014[123]
Diseases of heart 614,348
Cerebrovascular diseases 133,103
2015[124]
Diseases of heart 633,842
Cerebrovascular diseases 140,323
2016[125]
Diseases of heart 635,260
Cerebrovascular diseases 142,142
2017[126]
Diseases of heart 647,457
Cerebrovascular diseases 146,383
2018[127]
Diseases of heart 655,381
Cerebrovascular diseases 147,810
2019[128]
Diseases of heart 659,041
Cerebrovascular diseases 150,005
2020[129]
Diseases of heart 696,962
COVID-19 350,831
Cerebrovascular diseases 160,264
2021[130]
Diseases of heart 1 695,547
COVID-19 416,893
Cerebrovascular diseases 162,890
2022[131]
Diseases of heart 702,880
COVID-19 186,552
Cerebrovascular diseases 165,393
2023[132]
Diseases of heart 680,981
Cerebrovascular diseases 162,639
2024[133]
Heart disease: 683,037
Stroke: 166,783
Some thoughts I had:
4 year average in heart-related deaths from 2016-2019 = 649,284.75
4 year average in heart-related deaths from 2021-2024 = 690,611.25
The difference is 41,326.5
4 year average in cerebrovascular deaths from 2016-2019 = 146,585.0
4 year average in cerebrovascular deaths from 2021-2024 = 164,426.25
The difference is 17,841.25
That's not all that much of a difference pre and post vaccine. Certainly not the specter of a vaccine designed to induce fatal heart attacks and strokes. There is an increase, but I haven't bothered to factor in an aging populace, COVID causing an increased long-term risk of stroke and heart problems, strained hospitals, worsening socioeconomic conditions, and so forth.
Let's see 2010-2013, is there a meaningful difference?
heart-related average: 600368.0
cerebrovascular average: 129079.0
The difference from 2016-2019 is 48,916 for heart and 17,506 for stroke
This is comparable to the difference between the time immediately before and after COVID.
Let's do 2011-2014 to bring us closer to 2016, since some people may wish for this to be done.
heart-related difference from 2016 era: 44,752.0
cerebrovascular difference from 2016 era: 16,599.25
The difference is essentially the same for when I averaged 2010-2013.
It's official: Occupy Wall Street causes strokes and heart attacks. The difference CANNOT be explained by anything else. Notice the uptick beginning in 2013.
Only joking of course. But, this is literally the reasoning that COVID vaccine conspiracists use.
In all seriousness, after looking at these statistics, it would seem unlikely to me that the COVID vaccines have been causing mass death from heart disease or stroke. The increase is relatively small. The increase post-COVID is also not inherently suspicious, given the comparable increase from the early 2010s against the late 2010s. There aren't universal explanations for these increases, each multi-year era may have some of its own unique causes for increase, alongside many shared, long-term drivers of increase in these causes of death, socioeconomic conditions, for instance, which are always operative and worsening.
I'll now move onto your analysis of Pfizer's trial, since it pertains to vaccines.
Analyzing Pfizer's trial
So I was reading the Pfizer clinical trial to learn about the effectiveness of their vaccine. They've divided 36523 people into two roughly equally sized groups - one gets the vaccine, the other not. In the no-vaccine group, 162 people ended up getting COVID, while in vaccine group only 8. They portrayed it as a 95% effectiveness, but the way they've calculated it is 162 / 8 (results 20) then 100 / 20 (results 5). So the vaccine group had 5% of the amount of sick people as the no vaccine group. But these results are kind of meaningless without considering the actual amount people that got sick. In the no vaccine group, 0.88% of the test participants got COVID, compared to 0.04% in the vaccine group. The difference isn't so impressive now, is it? You have only less than 1% of a chance to contract COVID regardless of whether you took the vaccine or not. But how did they actually determine if you have COVID, anyway?
So all you needed to be considered "infected" was one symptom (even something like muscle pain, which could be from anything including the vaccine or the water injection) plus a positive "nucleic acid amplification-based" test (sounds like PCR, without mentioning the cycles used that would determine its accuracy). Doesn't seem very reliable, I'd make it at least three symptoms plus a PCR test with a relevant amount of cycles that is actually stated instead of hidden. I suspect the amount of actual COVID-19 cases is much less than displayed, because of the lax criteria. And since most of them are in the no-vaccine group, the biggest decrease would be there, and the vaccine's reported effectiveness would go down a lot.
The study explicitly tracked side effects like muscle soreness from the vaccines, so there's no chance that they would be attributing vaccine-induced soreness to COVID. Quoting from the study: [134]
The safety profile of BNT162b2 was characterized by short-term, mild-to-moderate pain at the injection site, fatigue, and headache.
In addition, the reactogenicity profile of BNT162b2 represented mainly short-term local (i.e., injection site) and systemic responses. These findings supported progression of the BNT162b2 vaccine candidate into phase 3.
Among BNT162b2 recipients, mild-to-moderate pain at the injection site within 7 days after an injection was the most commonly reported local reaction, with less than 1% of participants across all age groups reporting severe pain
The subjects are going to be assessed to exclude explanatory causes like vaccination or exercise anyway. These are symptoms indicative of illness that when combined with a positive test result all but confirm infection.
UPDATE November 2022: turns out the situation is worse than I thought. The trial was a total sham, not even being able to test all the participants for COVID:
https://www.bmj.com/content/375/bmj.n2635
>In her 25 September email to the FDA Jackson wrote that Ventavia had enrolled more than 1000 participants at three sites. The full trial (registered under NCT04368728) enrolled around 44 000 participants across 153 sites that included numerous commercial companies and academic centres. She then listed a dozen concerns she had witnessed, including:
This only contaminates a small proportion of the overall study group. This revelation was definitely serious and worthy of investigation, but it doesn't undermine the effectiveness of the vaccines, as there's plenty of other evidence demonstrating their effectiveness, which I've cited above. It is a far cry from making the entire trial a "total sham", that is just your own extreme characterization of it. This will be a repeated behavior of your's throughout the article.
Before moving on to the remainder of the article, there's still one more fundamental question I'd like to address:
It is a question central to the COVID pandemic regarding conspiracy theories.
Some studies have actually been conducted into the matter, like this one.[135]
>Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated?
>More than eight billion doses of COVID-19 vaccines have been administered globally so far and 44.29% of people are fully vaccinated. Pre-authorization clinical trials were carried out and the safety of vaccines is still continuously monitored through post-commercialization surveillance. However, some people are afraid of vaccine side effects, claiming they could lead to death, and hesitate to get vaccinated. Herein, a literature review of COVID-19-vaccine-related deaths has been carried out according to the PRISMA standards to understand if there is a causal relationship between vaccination and death and to highlight the real extent of such events. There have been 55 cases of death after COVID-19 vaccination reported and a causal relationship has been excluded in 17 cases. In the remaining cases, the causal link between the vaccine and the death was not specified (8) or considered possible (15), probable (1), or very probable/demonstrated (14). The causes of deaths among these cases were: vaccine-induced immune thrombotic thrombocytopenia (VITT) (32), myocarditis (3), ADEM (1), myocardial infarction (1), and rhabdomyolysis (1). In such cases, the demonstration of a causal relationship is not obvious, and more studies, especially with post-mortem investigations, are needed to deepen understanding of the possible pathophysiological mechanisms of fatal vaccine side effects. In any event, given the scarcity of fatal cases, the benefits of vaccination outweigh the risks and the scientific community needs to be cohesive in asserting that vaccination is fundamental to containing the spread of SARS-CoV-2.
>The present systematic review was carried out according to the Preferred Reporting Items for Systematic Review (PRISMA) standards [17]. A systematic literature search and a critical review of the collected studies were conducted. An electronic search of PubMed, Science Direct Scopus, Google Scholar, and Excerpta Medica Database (EMBASE) from database inception to November 2021 was performed. The search terms were “COVID-19”, “SARS-CoV-2”, “vaccine”, “vaccination”, “death”, and “autopsy” in the title, abstract, and keywords.
>The bibliographies of all located papers were examined and cross-referenced to further identify relevant literature. A methodological appraisal of each study was conducted according to the PRISMA standards, including an evaluation of bias. The data collection process included study selection and data extraction. Two researchers (AB and ACM) independently examined the papers with titles or abstracts that appeared to be relevant and selected those that concerned cases of death after COVID-19 vaccination. Papers regarding anaphylaxis deaths were excluded, as were preprints and non-English articles. Disagreements concerning eligibility among the researchers were resolved by consensus. Data extraction was performed by two investigators (AB and ACM) and verified by two other investigators (AM and MDP). Two investigators drafted the manuscript (AB and ACM) and other investigators (ET, PF, and VF) revised and finalized it. This study was exempt from institutional review board approval, as it did not involve human subjects.
>The sex and age of the subjects was not specified in all papers, therefore we used only papers in which these data were specified for the following calculations. The male/female ratio was close to one (1.04). The mean age was 52.74 years (range 22–91). The cases of death of people aged 50 years or younger were 21, while the cases of death of people older than 50 years were 26, with a ratio of 0.8. Considering the types of COVID-19 vaccines authorized by EMA (BNT162b2, Comirnaty®, BioNTech/Pfizer; mRNA1273, Spikevax®, Moderna; adenovirus type 26 vector COVID-19 Vaccine Janssen, Janssen®, Johnson&Johnson; recombinant chimpanzee adenoviral vector vaccine ChAdOx1 nCoV-19, Vaxzevria®, AstraZeneca), we found a total of 55 cases of death reported in the literature
The average age reported in this study is around 53. Let's use digdeeper's logic: Hey, it's mostly old people, so who cares. Young people are the minority of deaths. It's basically impossible for the vaccine to kill them.
>The causes of death were: vaccine-induced immune thrombotic thrombocytopenia (VITT) or, when VITT was not completely investigated, uncommonly located thrombosis associated with hemorrhages, in 32 cases (58.1%); myocardial infarction and/or some kind of pre-existing cardiac changes in ten cases (18.2%); myocarditis in three cases (5.4%); pulmonary artery embolism (PAE) in three cases (5.4%); acute disseminated encephalomyelitis (ADEM) in one case (1.8%); massive cerebral hemorrhage not associated with thrombosis or auto-antibodies in one case (1.8%); anaphylactic reaction to anesthetics associated with cerebral venous sinus thrombosis and anti-PF4 antibodies in one case (1.8%); hyperglycemic coma in one case (1.8%); hemorrhagic shock due to aortic dissection with rupture in one case (1.8%); complications of rhabdomyolysis in one case (1.8%).
>The distribution concerning the type of vaccine was as follows: 35 cases of death following the Vaxzevria® (63.6%), 9 cases following the Comirnaty® (16.4%), 6 cases following the Spikevax® (10.9%), and 5 cases following the Janssen® (9.1%). Figure 3 illustrates the distribution of the type of vaccine among the 55 cases.
The most harmful of them was Vaxzevria (Astrazeneca), which the minority of people took.
>The causal relationship between the death and the vaccine was not specified (meaning that the authors did not explicitly state if there was a causal relation or not) in eight cases (14.5%), not demonstrated or improbable in 17 cases (30.9%), possible in 15 cases (27.3%), probable in one case (1.8%), and demonstrated or very probable in 14 cases (25.4%).
>We found 55 cases of death temporally related to COVID-19 vaccine administration. The male/female ratio was close to one (1.04), showing no difference between sexes. The ratio between people aged 50 years or younger and older than 50 years was 0.8. So, it seems there is a slight predominance of older people among the cases. This is quite interesting, as we would have expected a more pronounced difference. Some possible reasons are that the death of a young person arouses greater interest, inducing the performance of investigations, and is more likely to be reported.
>As mentioned before, more than eight billion doses of COVID-19 vaccines have been administered worldwide. However, searching the literature, we found only 55 cases of death temporally correlated with vaccination, and in 17 of these a causal relationship has been excluded. Therefore, these 17 cases of death are only temporally, and not causally, related to the vaccine administrations. Among the remaining 38 cases, in eight the probability of a causal correlation between the vaccine and the death was not specified, in 16 the authors stated that it was possible or probable, while in 14 cases the causal relationship was very probable/confirmed.
>The ratio of deaths to the total number of administered vaccine doses (55 vs. millions of doses) clearly shows how rare fatal adverse events are, as has been found for other vaccines (for example, quadrivalent live attenuated and trivalent inactivated influenza vaccines)
In summation, this Italian study, which examined global reporting of COVID vaccine-related deaths, found 55 deaths temporally associated with the COVID vaccine. The study found that 17 deaths were determined not to have been from the vaccines, and found only 14 deaths that were very probable/confirmed to have been from the vaccines, out of the equivalent of millions of administered doses. This is a very low rate of mortality. At the time the study was conducted in 2022, millions had already died of COVID.
But, that's just one study, right?
Here's another from Finland: [136]
>COVID-19 vaccinations began globally at the end of 2020. By the end of 2021, 9.8 million doses were given in Finland. Regarding safety, most vaccine-related adverse reactions have been mild, but severe and lethal ones have also occurred. Autopsies in post vaccination deaths may give insight to the extent of fatal health conditions with potential COVID-19 vaccine etiology and provide new hypotheses of possible causalities between vaccination and severe health conditions. We searched the complete documentation on all medicolegal autopsies in Finland between December 2020 and December 2021 to assess how often the indication for autopsy was a suspected fatal adverse reaction to COVID-19 vaccination, and whether vaccination remained a potential etiology for any health condition determined as a cause of death after the autopsy. We linked register-based data on individual COVID-19 vaccination course and pre-existing health conditions. We found 428 autopsy cases with a mention of COVID-19 vaccination, and prior to autopsy, vaccination was suspected to play a part in 76 deaths. Post autopsy, a forensic pathologist considered vaccination to be potentially related to underlying cause of death in five and contributory cause of death in seven autopsy cases. These included seven thromboembolisms, two diabetic ketoacidoses, one myocarditis, one acute pancreatitis, and one eosinophilic granulomatosis with polyangiitis. In relation to the number of vaccinations within Finland, medicolegal autopsies were rarely performed because of a possible vaccine-related severe adverse reaction. Among the autopsies performed for such reasons, only a few considered a vaccine-related severe adverse reaction as a cause of death, although considerable doubt remains in the accuracy of individual considerations, and autopsy cannot definitively confirm causality between vaccination and death. Regarding vaccination safety, continuing evaluation of suspected vaccine-related deaths is essential, and autopsy should be considered in cases of death where vaccine etiology is possible.
>A total of 428 autopsy cases with a mention of having received COVID-19 vaccination were found, and their records were further investigated for the current report by a forensic pathologist (L.P.). A suspicion of vaccine etiology arose in 76 cases prior to autopsy (Fig. 1). After the autopsy and auxiliary investigations, 12 cases emerged, in which the forensic pathologist who wrote the death certificate considered the COVID-19 vaccination as a potential etiological factor for any cause of death: in five cases for the underlying cause of death, and in seven cases for a contributory cause of death (Table 3). Three of these cases had no pre-autopsy suspicion of vaccine etiology, and, thus, were not part of the 76 cases (Fig. 1).
This is 12 deaths, out of millions of vaccinated people. Note that three of the deaths weren't initially suspected to have been caused by the vaccine. This to me serves to undermine the notion of medical authorities failing to consider the harmfulness of COVID vaccines, when they were so honest as to discover and report something they didn't initially suspect. The fact that some deaths were initially suspected to have been caused by vaccines is also evidence undermining the notion of medical authorities failing or outright refusing to consider the harmfulness of the vaccines.
Most of the deaths are older and elderly people, digdeeper should take note of this, seeing how little he cares for their deaths.
Here's a study from Germany, which ran over the course of 3 months: [137]
>Postmortem investigation of fatalities following vaccination with COVID‑19 vaccines
>Thorough postmortem investigations of fatalities following vaccination with coronavirus disease 2019 (COVID-19) vaccines are of great social significance. From 11.03.2021 to 09.06.2021, postmortem investigations of 18 deceased persons who recently received a vaccination against COVID-19 were performed. Vaxzevria was vaccinated in nine, Comirnaty in five, Spikevax in three, and Janssen in one person. In all cases, full autopsies, histopathological examinations, and virological analyses for the severe acute respiratory syndrome coronavirus 2 were carried out. Depending on the case, additional laboratory tests (anaphylaxis diagnostics, VITT [vaccine-induced immune thrombotic thrombocytopenia] diagnostics, glucose metabolism diagnostics) and neuropathological examinations were conducted. In 13 deceased, the cause of death was attributed to preexisting diseases while postmortem investigations did not indicate a causal relationship to the vaccination. In one case after vaccination with Comirnaty, myocarditis was found to be the cause of death. A causal relationship to vaccination was considered possible, but could not be proven beyond doubt. VITT was found in three deceased persons following vaccination with Vaxzevria and one deceased following vaccination with Janssen. Of those four cases with VITT, only one was diagnosed before death. The synopsis of the anamnestic data, the autopsy results, laboratory diagnostic examinations, and histopathological and neuropathological examinations revealed that VITT was the very likely cause of death in only two of the four cases. In the other two cases, no neuropathological correlate of VITT explaining death was found, while possible causes of death emerged that were not necessarily attributable to VITT. The results of our study demonstrate the necessity of postmortem investigations on all fatalities following vaccination with COVID-19 vaccines. In order to identify a possible causal relationship between vaccination and death, in most cases an autopsy and histopathological examinations have to be combined with additional investigations, such as laboratory tests and neuropathological examinations
>As of June 30, 2021, a total of 74,871,502 vaccinations have been administered in Germany, including 54,898,640 with Comirnaty, 11,570,155 with Vaxzevria, 6,471,052 with Spikevax, and 1,931,655 with Janssen. A total of 30,986,128 people were fully vaccinated [48]. Due to the inherently limited number of people that were studied in the initial trials, it is necessary to further monitor adverse events after vaccination during population wide roll out of COVID-19 vaccines to detect also very rare adverse events.
>In Germany, the Paul Ehrlich Institute is responsible for the registration of adverse events after vaccination. The Paul Ehrlich Institute summarizes all reports it receives, irrespective of a causal relationship with vaccination, and regularly issues safety reports [48]. The Paul Ehrlich Institute received reports of 873 deaths with a temporal relation to COVID-19 vaccination by May 31, 2021.
Why are the evil medical authorities tracking vaccine safety? It's almost as if they're concerned with public safety, or something.
>Among the 873 reported deaths, 73 were related to the COVID-19 disease and not to adverse events. The vast majority of those who died had multiple comorbidities, such as carcinomas, renal failure, heart diseases, and atherosclerotic changes, which are potential causes of death. A total of 21 patients vaccinated with Vaxzevria died as a result of VITT.
>A total of 25 fatal hemorrhages, 24 of which were cerebral, were reported after vaccination with Vaxzevria. A total of 27 fatal hemorrhages occurred after Comirnaty vaccination, 18 of which were cerebral hemorrhages. A total of 2 fatal hemorrhages were reported after Spikevax vaccination.
>There were 5 deaths reported with myocarditis ranging from 1 to 50 days after vaccination with Corminaty. All 5 individuals had preexisting cardiovascular diseases that were potential causes of death. There was one patient who died 2 days after Vaxzevria vaccination from septic shock, acute renal failure, and myocarditis. Anaphylactic reactions were reported in 293 cases. Among these, 94 cases had the highest level of diagnostic safety. No fatal anaphylaxis was reported.
>In cases of deaths with a temporal relation to vaccinations, autopsies together with additional investigations can provide an important contribution for clarifying the causal relationship between vaccination and death. While numerous studies have been published on postmortem investigation of COVID-19 [3, 8, 19–21, 25, 32, 38, 60, 62], there are only a few publications on postmortem diagnostics of adverse events after vaccination [22, 29, 50]. In addition to clinical pathologists, forensic pathologists are also tasked with post-mortem investigations of fatalities following vaccination, making the topic of this article relevant to legal medicine. In the following, we report on the postmortem investigations of 18 fatalities after vaccination with COVID-19 vaccines.
>From 11.03.2021 to 09.06.2021, postmortem investigations of 18 persons who recently received a vaccination against COVID-19 were performed on behalf of the public prosecutor's offices in Bielefeld, Detmold, and Münster. The catchment area of these public prosecutor’s offices comprises around 3.24 million people, which accounts for about 4% of Germany’s population
18 of 3.24mil is 0.0005%, by the way.
>The mean age of the deceased was 62.6 years (age range: 32–91 years). Vaxzevria was vaccinated in nine, Comirnaty in five, Spikevax in three, and Janssen in one person. The time interval between the last vaccination and death ranged from a few minutes (case 17) up to 14 days (case 9). Case 17 involved a person who collapsed in a vaccination center immediately after vaccination; prompt resuscitation efforts were unsuccessful. A total of 12 deaths occurred at home, 4 deaths at a hospital, 1 death at a vaccination center, and 1 death at work.
>In 13 deceased, the cause of death was attributed to pre-existing diseases while postmortem investigations did not indicate a causal relationship to the vaccination. In one case (case 6), myocarditis was found to be the cause of death (Fig. 1). A causal relationship to vaccination is possible, but cannot be proven beyond doubt. A competing cause of death was found to be severe pre-existing cardiac changes. In four cases, there was evidence of VITT (cases 3, 12, 14, and 18). In case 14, the cause of death was established in hospital, being CVT and cerebral hemorrhage with hypoxic brain damage. The diagnosis was confirmed by postmortem investigations. A second patient who died in a hospital (case 12) suffered a severe anaphylactic shock during narcosis induction, resulting in hypoxic brain damage. This patient was vaccinated 12 days before she developed the shock symptomatic. She received unfractionated heparin after the adverse event. The serum-activated platelets were stronger in presence of PF4 than in presence of PF4/heparin complexes. This suggests that the patient had true VITT antibodies related to vaccination, rather than HIT antibodies related to later heparin therapy. The autopsy revealed multiple thrombi, including in the cerebral venous sinuses. Neuropathological examination found these to be fresh thrombi that must have formed after the onset of hypoxic brain damage (Fig. 2).
>As thrombosis or bleeding was not involved in this death, we consider the causal relationship between vaccination and death to be unlikely. Case 3 involved a 32-year-old woman who died at home; the autopsy revealed a cerebral mass hemorrhage without CVT. Laboratory tests for VITT were positive, so a causal relationship with vaccination and death is very likely. In case 18, a 69-year-old man who also died at home, the autopsy revealed CVT and the laboratory tests for VITT were positive. However, neuropathologic changes appropriate for causing death were not detected. Furthermore, a fresh thrombus of a coronary artery with severe atherosclerosis lesions and a fresh myocardial infarction was suitable to be the cause of death. Thus, a causal relationship between vaccination and death is possible, but cannot be proven beyond doubt. Of the four cases where postmortem investigations revealed a VITT, only one had been diagnosed before death.
In the scope of this study, 2 deaths were very likely to be due to the vaccine, and 2 were possibly caused by the vaccines. The rest had no evidence or weren't likely to be caused by them. As mentioned above, this study ran over the course of 3 months, from 11.03.2021 to 09.06.2021, in regions with a collective population of over 3 million people. If there were a bunch of deaths, we should've seen more than we did.
Here's another study from Germany: [138]
>Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination
>Cases of myocarditis, diagnosed clinically by laboratory tests and imaging have been described in the context of mRNA-based anti-SARS-CoV-2 vaccination. Autopsy-based description of detailed histological features of vaccine-induced myocarditis is lacking. We describe the autopsy findings and common characteristics of myocarditis in untreated persons who received anti-SARS-CoV-2 vaccination. Standardized autopsies were performed on 25 persons who had died unexpectedly and within 20 days after anti-SARS-CoV-2 vaccination. In four patients who received a mRNA vaccination, we identified acute (epi-)myocarditis without detection of another significant disease or health constellation that may have caused an unexpected death. Histology showed patchy interstitial myocardial T-lymphocytic infiltration, predominantly of the CD4 positive subset, associated with mild myocyte damage. Overall, autopsy findings indicated death due to acute arrhythmogenic cardiac failure. Thus, myocarditis can be a potentially lethal complication following mRNA-based anti-SARS-CoV-2 vaccination. Our findings may aid in adequately diagnosing unclear cases after vaccination and in establishing a timely diagnosis in vivo, thus, providing the framework for adequate monitoring and early treatment of severe clinical cases.
>Among the 35 cases of the University of Heidelberg, autopsies revealed other causes of death (due to pre-existing illnesses) in 10 patients (Supplementary Table 1). Hence, these were excluded from further analysis. Cardiac autopsy findings consistent with (epi-)myocarditis were found in five cases of the remaining 25 bodies found unexpectedly dead at home within 20 days following SARS-CoV-2 vaccination. Main characteristics of the five cases are presented in Table 2, while further autopsy findings are shown in Supplementary Table 2. Three of the deceased persons were women, two men. Median age at death was 58 years (range 46–75 years). Four persons died after the first vaccine jab, the remaining case after the second dose. All persons died within the first week following vaccination (mean 2.5 days, median 2 days). Clinical findings, blood tests, ECGs or imaging data were not available as deceased persons did not seek medical attention prior to death. Person 1 was found dead 12 h after the vaccination. A witness described a rattling breath shortly before discovering circulatory failure. Person 2 complained about nausea and was found dead soon thereafter. Resuscitation was started immediately but without success, respectively. The other persons were found dead at home without available information about terminal symptoms. According to the available information provided at the time of autopsies, none of the deceased persons had SARS-CoV-2 infection prior to vaccination and nasopharyngeal swabs were negative in all cases.
This study found 5 people who died of potentially vaccine-induced myocarditis. They were mostly older and elderly people, with comorbidities.
Here's a study from Qatar: [139]
>Evaluation of mortality attributable to SARS-CoV-2 vaccine administration using national level data from Qatar.
>Accurate determination of mortality attributable to SARS-CoV-2 vaccination is critical in allaying concerns about their safety. We reviewed every death in Qatar that occurred within 30 days of any SARS-CoV-2 vaccine administration between January 1, 2021 and June 12, 2022. Probability of association with SARS-CoV-2 vaccination was determined by four independent trained reviewers using a modified WHO algorithm. Among 6,928,359 doses administered, 138 deaths occurred within 30 days of vaccination; eight had a high probability (1.15/1,000,000 doses), 15 had intermediate probability (2.38/1,000,000 doses), and 112 had low probability or no association with vaccination. The death rate among those with high probability of relationship to SARS-CoV-2 vaccination was 0.34/100,000 unique vaccine recipients, while death rate among those with either high or intermediate probability of relationship to SARS-CoV-2 vaccination was 0.98/100,000 unique vaccine recipients. In conclusion, deaths attributable to SARS-CoV-2 vaccination are extremely rare and lower than the overall crude mortality rate in Qatar.
So, maybe 8 to 23 deaths in the country. And these aren't confirmed deaths, merely potential deaths. Even if you count all 138 deaths, that's still far less deaths than COVID caused. That's like a 0.002% chance of death for a random person.
Here's a study from Thailand: [140]
>Thailand began offering the coronavirus disease 2019 (COVID-19) vaccine nationwide in February 2021, with 1,885 deaths reported by the end of the year. Therefore, it is essential to assess the correlation between vaccination and cause of death from autopsy. This study included 34 autopsies of a deceased within 30 days after COVID-19 vaccination performed in Bangkok under the postmortem inquest service area of Bhumibol Adulyadej Hospital. The autopsies were performed by forensic pathologists. Moreover, detailed information about the deceased was collected, including age, sex, medical records, vaccination history, scene investigation reports, autopsy reports, cause of death, and a probable causal relationship between vaccination and cause of death. There were 24 males (70.59%), and the average age of the deceased was 52.76 years. Of all individuals, 28 (82.36%), 4 (11.76%), and 2 (5.88%) were vaccinated with AstraZeneca, Sinopharm, and SinoVac, respectively. The most common cause of death was ischemic heart disease (n = 17). None of the deceased patients had a causal relationship to the vaccine. Deaths were due to natural causes, as no definitive link between vaccination and cause of death was established in the study.
This study found no deaths definitively linked to the COVID vaccines at all, though I find it interesting that most deaths they selected were linked to AstraZeneca, which had been suspected in a study I cited earlier.
Here's a study from Singapore. It found nothing within 72 hours of vaccination: [141]
>Post COVID-19 vaccine deaths - Singapore’s early experience
>Singapore has been using mRNA vaccines developed by Pfizer-BioNTech and Moderna as part of the nation’s COVID vaccination program since 30 December 2020. From 1 February 2021–30 June 2021, a total of 34 deaths that occurred within 72 h of the deceased receiving their COVID-19 vaccination were referred to the Forensic Medicine Division of the Health Sciences Authority of Singapore. Autopsies, histological sampling and ancillary investigations consisting of total tryptase level, Immunoglobulin E (IgE), and C-reactive Protein (CRP), were performed on 29 of these cases. Our study has shown no definite causative relationship between the mRNA vaccination and deaths of individuals who died within 72 h after receiving the vaccination, in particular with regards to anaphylactic reactions, myocarditis and pericarditis, and thrombotic complications. Further studies may consider increasing the incident time frame from 72 h to seven days post-vaccination or longer to include any potential delayed presentation of adverse effects
Here's a study from Colombia: [142]
>A postmortem study of patients vaccinated for SARS-CoV-2 in Colombia
This study also found nothing
>A new coronavirus produces a disease designated as coronavirus disease 2019 (COVID-19). Vaccination against COVID-19 has resulted in decreased mortality. Postmortems of vaccinated patients play an important part in the forensic analysis of adverse effects after vaccination, which is essential for determining its efficacy and security. The main objective of this study was to describe the results of autopsies of patients vaccinated for SARS-CoV-2 carried out in two major centers in Colombia.
Materials and methods
>A descriptive cross-sectional study of 121 autopsies was performed following Colombian regulations in two main hospitals in Bogotá, Colombia, between March 1st and April 31st, 2021.
>Results
>118 of the 121 patients (97.52%) had been vaccinated with CoronaVac (Sinovac); only 3 had received other vaccines. Sudden cardiac death was the leading cause of death, with pulmonary embolism another critical finding. No relation between the cause of death and vaccination against SARS-CoV-2 was found.
>Conclusions
>A clinical autopsy is a vital for an accurate post-mortem diagnosis. Any relation between the SARS-CoV-2 vaccine and the cause of death should be carefully studied in order to provide the general public with evidence-based information about the safety of the vaccination.
What do we have? A couple dozen mortalities plausibly linked to COVID vaccines spread across several countries with millions of inhabitants. This is not exactly what you'd expect of some highly volatile, deadly snake venom, which is what digdeeper characterizes the COVID vaccines as being. With these numbers, the risk of dying from COVID is astronomically higher across all age groups than the risk of dying from the vaccines.
Of course, there could be deaths that the researchers failed to discover, but digdeeper has in his article assumed the stance that the medical authorities are a singular, omniscient entity which can perfectly track every death ever, seeing as the notion of countries, such as third world countries, failing to adequately track COVID deaths, doesn't even come to his mind once in the article, causing him to foolishly assert that impoverished third world countries "prove" the pandemic to be a sham.
Given the nature of these vaccine-induced deaths, it's unlikely that a meaningfully large chunk would go undetected.
The deaths tend to be sudden and unexpected.
Most developed nations investigate such fatalities, as they are unusual, and people desire answers. This is especially the case for young people. The sudden death of an old person may be overlooked, but it's unlikely to see such a thing regarding a young person. Why then are we seeing that most people reported to have died are on the older side, middle aged to elderly? The nature of the vaccine-induced death lends itself to investigation, and through this, discovery, due to its unusual, shocking abruptness, yet we have few documented deaths, and fewer deaths in the younger age groups that should be most intensely investigated. This is what we would expect to see from a vaccine that was not causing widespread death, particularly among younger people.
If vaccine-induced deaths were a significant phenomenon, the discovery of them at autopsy would become unavoidable, because there would be too many deaths for a country's general autopsy rate to miss them, and there would likely be an influence on nationwide mortality data explainable only by vaccines, but this hasn't happened anywhere.
It is possible that some deaths went undetected, meaning there may have been a couple dozen more deaths than were recorded. Nonetheless, this doesn't meaningfully influence the stance that the COVID vaccines were safe, and certainly far safer than COVID infection.
This major incident which dominated the news for at least a week during COVID, pertaining specifically to the subject of vaccine harmfulness, makes no mention in digdeeper's article. This is interesting for someone who supposedly spent so much time creating an article they felt to be somewhat comprehensive.
A motivation for omitting this incident from one's retelling of history would be that it serves to undermine their desired narrative.
The federal pause placed upon the Johnson & Johnson COVID vaccine by the United States Government significantly undermines COVID vaccine conspiracists notions of health authorities behaviors surrounding the safety of COVID vaccines. The incident demonstrates that health authorities were (1) monitoring the safety of the vaccines, and (2) willing to pull them from circulation if they should discover a meaningful risk of harm, which directly contradicts the conspiracists' notion of the health authorities circulating vaccines of which they did not know the safety, of which they did not care for monitoring the safety, and of which they were thoroughly uninterested in listening to safety concerns regarding.[143][144]
In April 2021 the FDA had Johnson & Johnson's COVID vaccine pulled from circulation.
Government officials monitoring VAERS noticed reports of thrombosis with thrombocytopenia, involving several individuals, some of whom died, after receiving the Johnson & Johnson vaccine, which prompted them to conduct an analysis, in part pulling medical records of affected individuals.
They discovered a legitimate risk of the Johnson & Johnson vaccine causing thrombosis with thrombocytopenia, usually in women in their thirties to forties, which could cause fatal strokes. 60 confirmed cases of thrombosis with thrombocytopenia were reported, in addition to 10 deaths. Although the risk of dying from the vaccine was low, given that 18 million doses had been administered, out of an abundance of caution, the vaccine was pulled from circulation. Nobody would be permitted to receive it.
This is not what you would expect from institutions who do not care about vaccines harming people, who even want for such things to happen. This is what you would expect from responsible institutions that have identified a previously-unknown, emerging, lethal risk associated with a fairly common vaccine, and wish to minimize harm by pulling it from circulation, in order to analyze the situation, before deciding what to do next.
Which brings up another vaccine pause. The pause of the AstraZeneca vaccine.
Just a month prior to the Johnson & Johnson pause, in March of 2021, several European countries, including Norway, Denmark, the Netherlands, Germany, France, Spain, Portugal, Italy, Slovenia, and Bulgaria, put a pause on the AstraZeneca vaccine due to concerns of recipients developing blood clots.[145][146]
The European Medicines Agency ruled that the benefits of the vaccine outweighed the risks of COVID, and most pauses were lifted.[147]
Instead of concerning himself with squaring these vaccine pauses with the notion of institutions seeking to kill people with vaccines, digdeeper has simply avoided the issue altogether, and focused on the misinterpretation of statistics.
Now, let's visit the beginning of the article: [148]
October 18, 2019. A New York City hotel is holding a pandemic drill which is supposed to educate the world leaders on what to do if such a situation arose in real life ... for now, just note that it contained people both from the USA and China. The highlight video of the event mentions stuff such as:
- The virus could cause a worldwide pandemic if not quickly controlled
- It spreads extremely fast
- Can only be combatted through corpos and governments from different countries working together
- Vaccine not likely to appear early enough to be useful
- Countries banning travel, flights being cancelled
- Economic collapse
- Governments being at war with the virus
- Social media platforms censoring "inaccurate" information
- Loss of faith in government
Meaning, they held an exercise for a highly virulent pathogen, which is what would cause a pandemic, which was what COVID was and what it did.
Who other than governments and corporations would combat a virus in the modern era? This is not strange.
Travel bans are also not strange given the scenario.
Nor is economic collapse seeing as travel is banned and global society would be shut down. Economies didn't completely collapse, though. Well, I guess it depends on what you consider a collapse to be.
I don't know what it means to be at war other than to fight it.
False information existed on the internet long before COVID, even cropping up around public health crises. It's not a surprise to me they would think to censor stuff in the information era if the information could be harmful to society by worsening the pandemic.
Censorship could then cause loss of faith in government. The government's response in general could cause loss of faith, if it was lackluster or inefficient and harmful in ways, which it predictably would be in a country like America.
Literally everything stated in the video has later happened in the real world.
Nothing that happened was exceptionally unique. It was all par for the course, what you'd expect during a global pandemic in the current state of civilization. In fact, their most significant predictions were incorrect, and their most damning details aren't actually all that significant.
They predicted that the virus would kill 65 million people in 18 months.[149]
>The invite-only event featured medical professionals, policy experts and business analysts all focused on how different institutions would respond to the onset of a deadly virus. The fictional coronavirus — a coronavirus, in general, being a specific kind of virus — in the scenario killed 65 million people over 18 months. Joint recommendations from participants urged international cooperation both in preparing for and handling a pandemic.
COVID killed at most half of that figure. It has been estimated that COVID killed a maximum of 35 million people worldwide. And this was over the entire course of the pandemic. That's not even close to their prediction. They predicted twice as many dead in half the time.
>The center further stated that the results of the scenario cannot be used to project for the COVID-19 outbreak because “the inputs we used for modeling the potential impact of that fictional virus are not similar to nCoV-2019.”
According to them their modeling wasn't all that useful.
>The origins and severity of the fictional pandemic differ from the current outbreak, as do the reactions of national governments and civic institutions. The disease in the scenario was "modeled largely on SARS" according to recaps of the program.
They also did not specify an origin country, like China, for example. If they did, that could be more damning. But even that wouldn't be too damning, as China has a historical precedent as being the originator of diseases, as does the Asian continent.
But the single piece of evidence that seals the deal is the fact that they mentioned a novel coronavirus right at the start - instead of any one of the hundreds other possible infections. How could they have known, if this wasn't planned in advance? They said that this wasn't a prediction and that the simulation was based on SARS (also a coronavirus) - but again, why not any of the other possible infections?
There have been previous coronavirus outbreaks since the new millennia. There was SARS in the 2000s.[150] Then MERS happened.[151] It shouldn't be a surprise that they would model this scenario on a coronavirus. Coronaviruses are highly contagious pathogens, with a precedent for causing large outbreaks.
They chose a coronavirus because that's the kind of virus that would spread in the manner the exercise anticipated. The majority of those diseases have low infectivity and or high lethality which precludes them from spreading extremely fast. A lot of them are not viruses, which can open the possibility of treatment with antibiotics, antiparasitics, and some of the viruses can be effectively treated with antiviral medications, unlike COVID. It's not realistic for those to cause a worldwide pandemic, it is realistic for a pathogen like COVID to have done this. What they predicted was similar to COVID, in the sense of being a coronavirus that caused a global pandemic, but that's about it.
They said that this wasn't a prediction and that the simulation was based on SARS (also a coronavirus)
You've conceded that it wasn't COVID itself but SARS which is not the same as COVID. The main similarity is that they're in the same family of viruses. That family of viruses is very contagious. And again, there's a historical precedent for their spread.
And why did they get everything else right
They didn't get everything right. They didn't posit an origin country, and they predicted far more deaths than were caused by COVID in half of the time. The predictions that they got "right" were things that anyone with even the slightest bit of an understanding of politics and geopolitics would be able to make.
Also, I didn't recognize any of the names of the participants of that exercise. I doubt that these people are global string-pullers, they're a bunch of people who seem to be mostly under the age of 50. Not distinguished members of the capitalist class. You have to assume the participants to be such string-pullers for this to be a truly malicious operation. I didn't see any Chinese people either.
And why would they even hold an event like this prior to COVID, while knowing what would happen in the future? It makes no logical sense. I know that many conspiracists buy into the notion of "predictive programming", that being the idea that "they", the conspirators, will plant ideas in the collective consciousness prior to performing them. They never provide any evidence of this even being a real phenomenon, or evidence of a real cabal of conspirators, but let's just put that aside. The logic works both ways. These "predictive programming" events can just as easily explained as the conspiracists being uncreative individuals, who falsely view certain ideas in popular culture, like pandemics, or buildings being demolished, as being exceptionally unique, when they aren't.
The "official" beginning
AKA the actual beginning
December 30, 2019. Li Wenliang, a doctor at the Wuhan Central Hospital, told his colleagues that 7 people were diagnosed with SARS infections that were traced back to the Huanan Seafood Wholesale Market, and that precautions should be taken. A few days later, Li was "educated" by the police to "not spread rumors". In the end, he was proven right - patients were coming in with a "new type of coronary pneumonia" and one of them even infected him on January 12 (translation graciously provided by the Big G botnet):
>I was very worried at first, but the doctor would comfort me every day when I went to the ward. I am no longer feverish, and my mental state is better than a few days ago. I believe the hospital and the doctor, I will definitely be cured.
You truncated that quote and removed crucial details from it.[152]
Here are two different translations of the quote in full:
I am currently in the isolation ward of the Respiratory and Critical Care Medicine unit at Wuhan Central Hospital. I'm receiving treatment in the monitoring room. I have difficulty breathing, I'm on oxygen, I can't get out of bed or speak; I occasionally look at my phone and type to communicate with others. At first I was quite worried, but the doctors check on me every day and comfort me. I no longer have a fever, my spirits are better than a few days ago, and I trust the hospital and the doctors — I will definitely be cured.
He is [mistranslation, should be "I am"] receiving isolation treatment in the intensive care unit of the Department of Respiratory and Critical Care Medicine of Wuhan Central Hospital. I have difficulty breathing, and I have an oxygen tube inserted. I can't get up or talk. I occasionally look at my phone and type to communicate with others. I was worried at first, but the doctor comforted me every day during ward rounds. I no longer have a fever and my mental state is better than a few days ago. I believe in the hospital and doctors that I will be cured.
He was in the ICU, had difficulty breathing, and was on oxygen with a breathing tube. The article you quoted is dated 31/01/2020 (the date actually appears in the URL, you don't need to read the article to see it). The information in the article appears to have been from that date and the time preceding it. Reports of Li Wenliang's worsening condition tend to appear in February.
The New York Times investigated Li Wenliang's death.[153][154]
>In early 2020, in the Chinese city of Wuhan, Dr. Li Wenliang lay in a hospital bed with a debilitating fever. He was no ordinary patient, and even then — before Covid had its name — he feared that this was no ordinary ailment.
>A government investigation into the circumstances around Dr. Li’s death concluded in a report that the Wuhan Central Hospital had spared no effort to try to save him. But a more complete picture of his medical care and his treatment by the authorities has remained elusive.
>The New York Times’s Visual Investigations team has now filled in some of these gaps with an exclusive interview with one of Dr. Li’s colleagues. He provided a firsthand account of Dr. Li’s final hours, describing the resuscitation measures that were used and discussed. We are referring to him only as Dr. B because he is afraid of reprisals from the Chinese government. The Times talked to Dr. B via video, and verified his identity with public information.
>The Times also obtained and examined internal memos from Wuhan Central Hospital and Dr. Li’s medical records, some of which backed up Dr. B’s account. The medical records have been verified by experts and contain details that match publicly available information. Eight U.S.-based Chinese medical experts, who have experience treating Covid patients or have practiced in Chinese hospitals, reviewed the medical records for The Times.
>We found no evidence his medical care was compromised. But these documents, along with Dr. B’s account and experts’ analysis, reveal important new details about his illness and treatment.
>In early 2020, the virus was spreading rapidly in Wuhan, the city in China where the pandemic first took hold. Dr. Li checked into the hospital on Jan. 12 with a fever, a lung infection and other symptoms. According to several of the doctors who reviewed his medical records for The Times, by the third day, Dr. Li was seriously ill and required oxygen support.
>“He was infected with an early variant of the virus, so the illness started acutely, its course was life threatening and it developed very fast,” said Dr. Wu Yuanfei, a virologist at UMass Chan Medical School in Worcester, Massachusetts.
>The experts said that based on the records, the treatment Dr. Li received, in general, followed the norms of that time for managing the symptoms of coronavirus patients.
>A little over a week into Dr. Li’s hospital stay, his doctors wrote that he was struggling mentally and diagnosed him as being in a depressive state, a detail that has not been reported. The record did not attribute his emotional condition to any specific factors, but noted that Dr. Li had lost his appetite and couldn’t sleep at night.
>He was kept in an isolation ward, allowed to communicate with his family only by video chat. He had just weeks earlier been disciplined by the police for warning friends in a private group on WeChat, a Chinese social media service, about the new virus that was spreading through the city. His employer, Wuhan Central Hospital where he worked as an eye doctor, had made him write a letter of apology, the content of which was obtained by The Times.
>But on Feb. 5, Dr. Li’s condition deteriorated severely — his pneumonia grew worse, his breathing became extremely labored.
>That afternoon, Dr. Li’s doctors ordered several tests of his lungs and heart, his medical records show. According to Dr. Yuan Jin, a pulmonary and critical care doctor at Good Samaritan Medical Center in Brockton, Massachusetts, these exams suggest that Li Wenliang’s medical team was responding to a worsened condition.
>By the morning of Feb. 6, doctors wrote in the progress notes that Dr. Li was at risk of multiple organ failure. Several physicians we spoke to said that Dr. Li’s condition was so serious that his medical team should have at this point, or before it, considered intubating him and placed him on a ventilator — a higher level of oxygen support.
>The records indicate that Dr. Li had earlier been given oxygen through a nasal tube and then an additional oxygen mask. His medical team also tried to use a noninvasive ventilator on Jan. 19, but wrote that “the patient could not tolerate.”
>It is unclear why Dr. Li was not intubated. Some doctors are more reluctant to intubate young patients; sometimes the patients themselves refuse it. To this day, there is no consensus on when invasive ventilators should be used on Covid-19 patients.
>On Feb. 6, Dr. Li went into cardiac arrest at around 7:20 p.m. Though his daily progress note did not explicitly say that his heart stopped, it recorded that the medical team started performing CPR — a procedure that is applied in such an emergency. They intubated him at that point, a common practice during resuscitation. The note said his pupils were not responding to light.
>According to the medical records, doctors tried to revive Dr. Li for over seven and a half hours, but his heart never restarted.
>The government investigation said doctors placed Dr. Li on extracorporeal membrane oxygenation. Also known as ECMO, it is a last resort, invasive treatment involving a machine that siphons blood out of the patient, runs it through an oxygenator and pumps it back into the body.
>According to Dr. B, who arrived at Dr. Li’s intensive care ward around 9 p.m., about two hours after Dr. Li entered cardiac arrest, the hospital’s leadership pushed the medical team to use ECMO because it wanted to show the public that no effort had been spared.
>But several doctors in the room argued that by that point it was too late for it to have been of any use, an assessment that six physicians we talked to agreed with. Dr. B also said putting Dr. Li on ECMO, given its invasive nature, would have been an “insult to his body.”
>Dr. B left the room around midnight. He said ECMO had not been used because an instrument to perform the procedure was not available. It is unclear whether it was ultimately used after he left.
>There is also no indication in the doctors’ orders from that night that the procedure was ever administered.
>But for some reason, the daily progress notes say ECMO was used. It was the only discrepancy of this kind found in the medical records.
By all reports, Li Wenliang was infected with COVID, and his condition worsened until he died. You are contesting this on the basis of his own self-reporting of his condition, which is relayed in an article dated 31/01/2020, prior to the worsening of his condition.
People who are seriously ill sometimes report feeling better, and their fever sometimes drops, but they die anyway. Fever reduction does not speak to the damage his organs and lungs had sustained. His infection could have improved, but that does not mean his organs were unscathed. Patients sometimes also report feeling better, before later dying. This happens with pneumonia patients.
You go on to state:
However, he ended up dying, even though he wasn't in the age group (34) that dies from corona:
You show an image that displays people in Li Wenliang's age group having a mortality rate of 0.08%. Since you didn't consider Li Wenliang's condition, the 0.08% figure doesn't give us much insight into what this truly means.
The source for this image wasn't linked but I tracked it down: [155]
>We assume that 30% of those that are hospitalised will require critical care (invasive mechanical ventilation or ECMO) based on early reports from COVID-19 cases in the UK, China and Italy (Professor Nicholas Hart, personal communication). Based on expert clinical opinion, we assume that 50% of those in critical care will die and an age-dependent proportion of those that do not require critical care die (calculated to match the overall IFR).
This study provides the reader with a reminder that people in critical condition were more likely to die than others, with how they assume a high rate of mortality.
If you actually look at the statistics for Wuhan, China, and for the earlier months of COVID in general, you will see that people in critical condition, like Li Wenliang, had a higher mortality rate. The mortality rate for people in critical condition was highest for those above the age of 50, but the rate of mortality was still heightened for younger people. It was greater than 0.08%. That 0.08% would primarily be people in critical condition.
There aren't any reports I've found of people saying that Li Wenliang was killed by anything other than COVID. He had medical staff monitoring him. Who would have killed him, and why? What would they have done to kill him, when he already had severe damage to his organs from the disease?
The whole point of your article is to minimize the dangerousness of COVID, and yet with this segment, you are taking a doctor who was trying to raise the alarm of the dangerousness of COVID, and saying he was killed, and that this somehow affirms your narrative on the "conspiracy" of COVID. By your own standards, it shouldn't be a big deal. So, why focus on this? It doesn't seem sensible to me. Your implicit viewpoint is that they killed him in order to quell panic i.e prolong efforts to mount a resistance to the disease with proactive measures like lockdowns i.e allow the disease to spread i.e let it go global and cause mayhem and give an excuse to implement tyranny. Yet you go on to rail against any efforts to stop the spread of the disease whatsoever and minimize its dangerousness. This is not coherent.
Let's assume Li Wenliang was killed.
I won't say it's impossible. The Chinese government, like the American and Russian governments, has done these sorts of things. I don't think there's much evidence it happened. He had several people monitoring him regularly, and performing tests on him. The NYT reported that there didn't appear to be evidence that his quality of care was compromised, in order to indirectly kill him, rather than directly kill him with some kind of poison or something. But, let's put that aside.
This itself doesn't evince an overarching, international conspiracy.
He was infected with an earlier strain of COVID, which was more lethal than later strains. His medical records support a worsening condition consistent with severe COVID. His health was also being monitored. I therefore think he probably died of COVID, and the Chinese authorities tried to quell panic, and this had disastrous effects which also made it seem to western audiences, primed with anti-Chinese propaganda, as though they killed him or got him killed. People in the west are brainwashed to despise China and harbor great suspicion towards the Chinese government, so it would be natural for westerners to perceive foul play where there may not be any.
You're assuming malice and only malice where there could be a non-malicious explanation. This is not a rational approach. This is what you do when you are working towards a desired conclusion, borne of personal, ideological investment. You will continue to do this.
How dangerous is the new coronavirus?
Analyzing case rates
First of all, let's realize the fact that whoever counts the cases can do it in whatever way he wants to. So, the numbers we've been presented for the entirety of the "pandemic" might have been fudged. It's the same principle as in the saying, that it doesn't matter who you vote for, but who counts the votes. It has actually already been admitted that the fearmongers double-counted tens of thousands of UK test results. I suspect they've done similar things in many other countries, so the overall case amount will be overreported even more. See how easy it is to create a "pandemic" when you control what is reported as a case? Hey, why not? No one can check up on you or punish you.
With the wording "I suspect they've done similar things elsewhere", you're assuming that they have intentionally inflated the numbers in other regions. On what basis is this being assumed? Presumably, on the basis of a global conspiracy, due to Event 201 supposedly having predicted COVID, which it clearly did not predict. This is then a baseless assumption of yours, driven by meaningful bias.
But let's be charitable and assume that a "case" is actually based on something real, like PCR test results. A PCR test is a tool that checks whether you have a certain genetic sequence in your body (in this case, a part of the COVID genetic sequence). Any time PCR testing is used - it is assumed that you having some genetic sequence inside your body means you are by definition sick and / or can infect others. Kary Mullis - the inventor of the PCR test - denied this interpretation, however; all a positive result means is that something's there, not that it's necessarily doing something bad.
With this, it should already be obvious that "counting cases" was pointless - but let's continue.
Your reasoning thus far:
A PCR test checks for a genetic sequence in your body.
Any time PCR testing is used it is assumed that you having some genetic sequence inside your body means you are by definition sick and / or can infect others.
Kary Mullis - the inventor of the PCR test - denied this interpretation
All a positive result means is that something's there, not that it's necessarily doing something bad
With this, it should already be obvious that "counting cases" was pointless
Your definition of the term "case" is also a bit nebulous. My definition would be that a person has been infected. That doesn't speak to the severity of their condition.
Counting cases is not pointless if you are seeking to track the spread of the virus, which governments were trying to do. A PCR test alone may not give one qualitative insight into how sick someone is, or if they're asymptomatic. But, it does tell you that the virus is or was in them, meaning they've been exposed, they've been infected. This is undoubtedly useful for tracking the spread of the virus. What are they supposed to do? Not track the virus? Let it run wild and free? If you want to take prophylactic measures, quarantining people who test positive for it may not be a bad call. That way you can see if their symptoms manifest or not. You can say that the virus being present within them does not mean it will harm them, but you cannot know that until either their infection manifests as illness or it goes away without causing symptoms.
Every PCR test is set at a certain cycle threshold, which just means the amount of times you amplify the sequence you are trying to find. This means that, the higher the cycle threshold, the more people will be found positive (less amount of virus sequence in the body will trigger the test). However, less amount of virus sequence in the body also means less potential to get sick and infect others. The important thing to understand here, is that you can increase or decrease the amount of reported cases just by changing the amount of cycles the tests are run at. To determine the logically optimal amount of cycles to use, we need to find the correlation between the cycle threshold and the infectivity. That's exactly what this study has attempted to do:
I've put the study cited by digdeeper here.[156]
Something to bear in mind with this discussion of Ct values and PCR tests is that Ct values are not a standardized metric. On different tests, Ct values can indicate different viral loads. But, the logic is still true that a higher value indicates a lower viral load. The viral load decreases exponentially.
Quoting Canada's public health services.[157]
>Ct values cannot be compared between different PCR tests
>There is no standard yet to be able to compare one test to another so the Ct range can greatly differ by the type of test used, that may use different signal detection methods. In fact, even when testing identical samples using different PCR tests, the results can differ by up to 8 Ct values (e.g., from 22 to 30). This has been observed in the laboratories from different jurisdictions (e.g., Ontario, British Columbia and Saskatchewan).
A document circulated by the APHL affirms this stance.[158]
>Can I compare a Ct value from one test method to another?
>Ct values and cutoffs are assay- and method-specific. A specimen with a Ct of 35 by one assay will not necessarily have the same Ct value by other assays. These values can vary up to two to three logs from test to test due to how the tests are designed.
End of quoting.
This graph shows that you cannot manufacture infectious virus in culture if the sample tested positive at 36 cycles or more. Even the people who tested positive with 30 cycles can only infect others 20% of the time.
From what I see, at 30 Ct, the amount of positive samples dropped to 18.6% after 2 weeks.[156] A 20% risk of infection is significant. Think of how many people one encounters in their daily life. On a societal scale, that's more than enough to ensure a spread of the virus. On the third week, at 30 Ct, 7% of samples were positive. 7% is still significant on a societal scale. In that study, most people who tested positive in the first week had a Ct value below 25. By your own standard, most would have a statistically significant risk of infecting others.
Now guess what amount of cycles have the authorities used for their tests?
You proceed to show an image with various cycles, that averages around 37.[159] Ct values were not standardized, so these could correspond to different viral loads.
This is only in the UK, but surely, this fraud was repeated worldwide. UPDATE: the same thing has been done in Australia (local) - "Each amplification reaction is known as a cycle, and usually 35-45 cycles are undertaken". And so, probably every country is in on the fraud.
Two similar countries with a shared history have similar policies, therefore, every country on earth has the same policies. This obviously does not follow. Nor is this a "fraud", that's your own characterization of what they are doing, based on your narrow interpretation of the utility of PCR tests. They can be employed to track the spread of a virus, not just the severity of illness. The tests do not give qualitative insight into the severity of one's illness. People with low Ct values can be relatively healthy, people with higher Ct values can be quite sick.
In terms of the UK graph - look at the amount of times figures above 36 appear, even though they are totally unjustifiable scientifically, since those cases cannot infect others. Since the 30-35 range is contagious 3-20% of the time (according to the first graph), the vast majority of cases tested positively with 30 to 45 cycles are fraudulent. And there are a lot of those:
You proceed to show a screenshot of Ct value statistics for some parts of the UK.[160] Ct values of 21-30 are on average 55% of tested cases. There is not really one universal percentage for the likelihood of a person with a Ct value of 30 infecting others. You mentioned 20%. It's not necessarily 20%. It could be lower, below 10%. But on a societal scale this does present the risk of it spreading around. That's why you have medical practicioners evaluate patients and determine what should be done, whether they should be quarantined, or not, on a case by case basis.
This graph shows that you cannot manufacture infectious virus in culture if the sample tested positive at 36 cycles or more. Even the people who tested positive with 30 cycles can only infect others 20% of the time.
About 30% of overall Covid cases are in the 31-40 CT range, and ~90% of those will be false positives.
On what basis will 90% of these results be false positives? You didn't show any evidence for this.
Even then, that's still the best case scenario for the fearmongers. Because other studies got even more damning results:
>SARS-CoV-2 Vero cell infectivity was only observed for RT-PCR Ct < 24
That is just one study
This other study relays cases of high Ct values with infectious samples: [161]
>In their recent article published in Viruses, Michel Drancourt and colleagues [1] have made an interesting but underestimated side-observation. As shown in Figure 1, they were able to isolate infectious SARS-CoV-2 virus from a clinical sample with a low concentration of viral RNA, which is reflected by a PCR Ct-value of 33
>Among the early publications implying that patients with Ct-values ≥ 30 are not infectious anymore is another study by the group of Didier Raoult [4], which already has unintendedly shown that 50% of clinical specimens with Ct-values ≥ 30 can be cultured and therefore may be potentially infectious.
>When they analyzed the outcome of an external quality assessment challenge, it turned out that quantitative results deviate in 7.7% of cases by more than ±4 cycles (up to 18 cycles) from the respective individual means, leading to the conclusion that standardization is needed, if patient management procedures should be based on SARS-CoV-2 (RT) PCR Ct-values.
This study also brings up the lack of standardization of Ct values, and how results can skew across tests.
>Additional studies have also shown that culturing of SARS-CoV-2 is possible with samples containing significantly less than the previously claimed culturing threshold of 106 genome equivalents [13] and that successful cultivation after day 8 from sampling or symptom onset is also possible [16,17]. Beyond this, a recent study from Switzerland demonstrated that a number of further environmental factors, such as air–liquid interface, contact and temperature difference, are further important factors for successful SARS-CoV-2 replication in cell culture, leading to the conclusion that we still cannot rely on Ct-values as a marker for infectiousness [18].
>The study of Aron et al. showed that 2 out of 8 samples (25%) with Ct-values higher than 30 could still be successfully cultured (see Figure 2 of [19]). Although the likelihood of culturing success decreases to 6%, Singanayagam and coworkers have shown that culturable virus may be shed more than 10 days after onset of symptoms, despite Ct-values > 35 [20] leading to infection control difficulties in periods of high infection rates, as observed in India, as it cannot be excluded that in rare cases patients can shed a viable virus more than 10 days after symptom onset.
>In addition, Kujawski and coworkers were also able to isolate a culturable virus from samples with higher Ct-values (>30) [12], suggesting that theoretically even small amounts of infectious particles might be enough to initiate an infection in vivo as long as no reliable data on the necessary minimum infective dose exists.
Here's a study which cultivated infectious samples at values above 30: [162]
>Severe acute respiratory syndrome coronavirus 2 viral load in the upper respiratory tract peaks around symptom onset and infectious virus persists for 10 days in mild-to-moderate coronavirus disease (n = 324 samples analysed). RT-PCR cycle threshold (Ct) values correlate strongly with cultivable virus. Probability of culturing virus declines to 8% in samples with Ct > 35 and to 6% 10 days after onset; it is similar in asymptomatic and symptomatic persons. Asymptomatic persons represent a source of transmissible virus.
It was possible for individuals with a viral load of 30 or greater to be infectious, but the probability was low.
Viral load tends to drop substantially over the course of 2-3 weeks. As a result, if you use a lower Ct value, you can easily miss people who had been infected with COVID, and thus hamper your ability to trace its spread.
According to this study, anyone with a positive test at 25 cycles or more is not contagious. If we took this study at face value, about 3/4 of the listed COVID cases would be fraudulent.
If you took the study at face value and rejected the utility of tracing the spread of the disease.
But it gets even worse - according to this paper:
>Culture medium presents ideal conditions for a virus to grow and may detect virus that is not present in the quantities required to initiate infection in a human host.
This means that the infectious potential is even lower between humans than in culture, and so the "real" amount of cases drops even more.
It would be lower, but the difference isn't entirely quantifiable.
They clearly wanted as many cases as possible to scare you, and that's why they set up the tests this way.
Like I said before, the spread of the disease can be better traced with higher CT values. You're assuming intent. This then becomes a discussion of how the media portrayed COVID.
There were already suspicions back in February 2020 that the tests are only 20% accurate.
>When the infection rate of the close contacts and the sensitivity and specificity of reported results were taken as the point estimates, the positive predictive value of the active screening was only 19.67%
He links to an article from Republic Broadcasting, some conservative pundit.[163]
It cites a withdrawn preprint of an article. A preprint is an article preceding peer-review. Peer-review is of course to verify the authenticity of the article's information.
Why was the article withdrawn? [164]
>Editor office’s response for Ahead of Print article withdrawn The article “Potential false-positive rate among the ‘asymptomatic infected individuals’ in close contacts of COVID-19 patients” was under strong discussion after pre-published. Questions from the readers mainly focused on the article’s results and conclusions were depended on theoretical deduction, but not the field epidemiology data and further researches were needed to prove the current theory. Based on previous discussions, the article was decided to be offline by the editorial board from the pre-publish lists
This is just one flawed study that is being cited by a conservative pundit, and you're using it to cast the narrative of "suspicions" as though they were widespread.
Looking at this with the wisdom of passed time, it's obvious to me that "counting cases" should have never been something that was done to begin with. All it does is provide a "big number" to scare people into submission to quarantines, lockdowns, and vaccines. And once you have people trusting that "big number", you can find ways to increase it infinitely and continue having a justification for the restrictions. Or you can then also reduce the "big number" whenever you want to show that a restriction has worked to contain the spread, for example. All while nothing really changes in terms of people getting sick, or the severity of their sicknesses. Meaning, the "bigness" of the number doesn't actually change what's happening in reality - as shown above in the many ways to fudge it. But, of course the rulers knew all this already before the "pandemic" started. And that's why they've focused so much on the "big numbers" (instead of - say - improving people's health so that they can survive the sickness). Another one of which was the coronavirus death rate:
You could juke the stats if you increased and decreased CT cycles, but there were established values which were quite high (above 30), and remained quite high. To deliberately rig the stats in the manner you're suggesting requires a global conspiracy, involving everyone who is testing for COVID. That's virtually impossible, and it quite clearly is not a serious consideration when you thoroughly examine how and why they tested for COVID, which you did not do.
Most tests could catch people who had been recently infected, but weren't necessarily ill or infectious. There was undoubtedly utility in tracking the spread of disease. Not tracking the spread of a pandemic that has popped up all over the world is incredibly reckless. It is not as though people who have a very low viral load could not have had a higher viral load prior to testing. What you've shown suggests that many people may not have been seriously ill, but were exposed, and were possibly ill, and could have infected others.
You are assuming the worst of medical authorities when there are alternative explanations for their actions.
Analyzing the death rates
Imagine you have in your hand a gun that can only kill people that wear green elf hats - it does absolutely nothing to anyone else. And even then - you'd have to wait weeks until the elf hat enthusiasts would maybe die. Wouldn't you think that is weird? Wouldn't you begin to wonder if - perhaps - it is those hats that kill their wearers, and not your weapon? If real guns worked that way, absolutely no one would buy such pieces of junk. Yet, that is exactly what COVID-19 does - except that the hat is replaced with chronic diseases and age:
Well, that's not true because healthy people did die, it was just uncommon. You're denying that their deaths happened.
As you can see, it's almost impossible to die from corona without those pre-existing diseases.
0.9% is not insignificant, that's almost 1%, which on a societal scale amounts to many people. 1% of 350 million people is 3.5 million people.
For an American example: COVID killed more Americans than World War II.
The number also doesn't give insight into one's probability of dying, that's not entirely quantifiable. You can assume that your chance as an individual of dying is low, but that number reflects the deaths of many people. You arrive at a mortality rate through people dying. It's not like taking a .44 magnum revolver with a 5 round chamber, with 1 bullet in the chamber, and then mathematically inferring that you have a 20% chance of death on your first shot, after spinning it randomly. It would be like having a magazine-fed pistol, which has an unknown capacity of rounds, and an unknown amount of live rounds in relation to dummy-rounds. You draw the gun upon a person, and pull the trigger, not knowing if it will be a dummy-round or a live round. Once you've established that the magazine is finally empty, you count the bodies, and gauge the chance of death. Then you use the same pistol with the same capacity and ratio of live rounds to dummy-rounds, in random sequence.
This is obviously assuming certain death from a headshot, and not considering long-term sequelae from COVID infection, as could be represented by gunshot injury.
Early Italy, which has had the highest death rate out of all the countries - provides even stronger evidence for my thesis. According to Silvio Brusaferro - head of Italy's health institute - not one of the over 4000 deaths has been confirmed to be exclusively from corona:
What he said was that they had comorbidities. All that means is that people without comobordities are far less likely to die.
So, not only were the people who died old (look at the chart at the top of this report to realize anyone under age 60 is pretty much immune), but they've also all had chronic diseases - both massive causes of death that certainly don't need help from some puny virus. The deaths are also almost all from heavily polluted areas - yet another contributing factor independent of corona. Anytime someone gets sick or dies, there is a multitude of contributing factors that control the progression of the situation
You cannot know that these people were all on their last legs. Cardiovascular disease, diabetes, chronic respiratory disease, hypertension, and cancer are treatable conditions and are quite common. In America, almost half of the adult population has some form of cardiovascular disease or hypertension.[165][166] About a tenth to an eighth has diabetes.[167]
Yet, you wouldn't say that half of Americans are terminally ill.
Europe tends to have lower rates. I can't give a blanket figure, but in a lot of countries at least a fifth of people have hypertension.
The people with comorbidities who died weren't all terminally ill, and on the brink of death. Looking at them from the outside, they could seem to be healthy people. But, they caught COVID, had a horrible infection due to their comorbidities, and died. Even young people with asthma who were otherwise healthy died of COVID.
What you are saying here implicitly is that people who suffer from diseases that act as comorbidities in COVID cases do not matter; that their lives do not count, and that we shouldn't care about them. That we should keep society open, and if they die, so be it. That's what you're saying here. So, you don't value the lives of people over the age of 50, and people suffering from health conditions that are widespread in society. We've established this.
Allowing those people to die would have horrific effects upon society. The death toll would amount to tens of millions of people. The economic impact would be catastrophic, it could threaten societal collapse, which would lead to much more death.
This is extremely callous. But, callous individualism is common among conspiracists. It makes less sense in the backdrop of your website, as you show, or at least feign, interest in the welfare of the masses. Maybe it's not genuine.
More recent evidence shows hospitals in the US are actually paid for putting COVID-19 on the death certificates.
He cites an article from some website called thespectator, which relays some lies from Fox News.[168]
Nothing about the article said that they were getting paid to put COVID as a cause of death. This is imbeciles on Fox News not knowing how the US healthcare system works, unless they're outright lying. Their idiocy is unsurprising, nonetheless.
The government is reimbursing the hospitals for the cost of caring for COVID patients. They're getting three times as much if the COVID patient goes on a ventilator because those patients cost more to take care of.
You don't understand how the US healthcare system works. It's not like in Europe where everything is covered. If the government didn't step in to cover medical expenses, it would either come out of the patient's end or the hospital's end. Capitalism demands that it comes out of the patient's end (see how the tariffs are driving up consumer prices in America, the supplier will never foot the bill). But, to make a patient foot the increased bill during a pandemic would have catastrophic societal effects, the personal bankruptcies could threaten revolution or collapse. Furthermore, many simply wouldn't be able to pay, so there wouldn't be any money to cover expenses. The hospitals then would need to pay, but, they'd eventually run out of money, and even if they didn't run out of money, the money they would spend would hamper their ability to care for people. The outcome would be hospital closures and mass death. This would again have catastrophic societal effects.
In a pandemic scenario, even capitalism has to make some concessions in order to survive. The capitalist-controlled government came in and footed the bill.
Also, it seems flu deaths have almost completely disappeared this year, just like that. Of course, it's because they've been reassigned to nCov.
Did you read the flu article that you cited? [169]
>There are several reasons the flu could be lower this year, though all are speculative at this point.
>Part of it could be due to increased vaccinations, according to recent data provided by the CDC.
>As of November 27, 2020, the CDC reports that “188 million doses of flu vaccine have been distributed in the United States” which is “the highest number of flu doses distributed in the United States during a single influenza season.”
>The flu vaccine is usually moderately effective with the CDC estimating that it “reduces the risk of flu illness by between 40% and 60%.”
>Social distancing, stay-at-home orders and substantially more people wearing masks may also be contributing to the record low flu activity. Though once again, that is speculative.
Compound this with the fact that the flu is less contagious than COVID and the world was locked down.
Where's your evidence of flu cases being assigned as COVID cases? Oh right, you have none. Just another baseless assertion.
If you think that's bad, wait until you see how the United Kingdom counts its coronavirus deaths:
He then provides this screenshot.[170]
I had to have faith in you to be truthful, as that screenshot alone wasn't proof of anything. So, I looked into it. As it turns out, people actually asked the UK government how they count deaths and they answered.[171]
>You asked
>I should like you to answer these questions
>Deaths within 28 days of a positive covid test, are now standing at over 140,000, please confirm how many of those deaths were JUST FROM covid, i.e. no other cause shown on the death certificate. Please just give me the figure, and not, as in the past, all the other details as well.
>Please also take any day you like in the past ten days and confirm how many positive covid tests there were on that day, and also how many negative tests there were on that same day.
>Please provide a breakdown of where these test results came from - CIS
>Please also confirm what steps if any have been taken to notify MPs and the media of the actual number of deaths FROM covid as opposed to WITH covid
>We said
>Thank you for your request.
>It is important to note that the ONS do not provide the number of deaths within 28 days of a positive COVID-19 test. This is the criteria used by public health agencies to monitor the pandemic.
>ONS counts a death involving COVID-19 as a death where COVID-19 is mentioned on the death certificate. Doctors are required by law to certify the cause of death 'to the best of their knowledge and belief'. This means the medical professional believed COVID-19 had been involved in the chain of events that led to the death. Testing could inform part of the information provided by the medical professional, but they could also use other information (such as symptoms and x-rays, for example). This means that someone could have COVID-19 on the death certificate who may not have been tested for COVID-19. Also, in some cases, the person may have tested positive for COVID-19, but the medical professional believed that COVID-19 did not play a part in the death. This means COVID-19 would not appear on the death certificate.
>Deaths within 28 days of a positive test are used by public health agencies and are useful to respond to the virus quickly. Information provided on the death certificates take longer to collate but provide more robust figures on the number of deaths involving and due to COVID-19.
>We use the term "due to COVID-19" when referring only to deaths where that illness was recorded as the underlying cause of death. We use the term "involving COVID-19" when referring to deaths that had that illness mentioned anywhere on the death certificate, whether as an underlying cause or not.
There is a difference between deaths "involving" COVID, which they track to get an idea of the overall situation, and deaths determined to have been caused by it. Death rates were not being inflated by these means.
They were tracking statistics of deaths involving COVID in order to get a sense of how bad the situation was. Then, they had a separate category of deaths confirmed to have been caused by COVID, as determined by autopsy.
It's a bit disingenuous for you to display that screenshot and act like it's being used to portray actual deaths from COVID, when that's not what is happening. I don't know where you got the photo from, so I can't know your true intent.
That's right! If you get tested positive, then fall of a ladder, you're a COVID death case. Example is from Croatia;
Did you read the article that you cited? [172]
>He suffered lacerations, minor bruises and abrasions from the fall and was declared dead at the scene, but it was later found that he was actually positive for COVID-19.
>An autopsy was conducted to find whether his death was really caused by the accident and doctors found evidence of damages to the man's organs including his heart and lungs, which were said to be "heavy" and had "markedly reduced air content," the report stated
>Based on the autopsy results, they concluded that the man suffered from acute respiratory distress syndrome (ARDS)
He died from COVID. The fall was the last nail in the coffin, he was on his last legs. Maybe he wouldn't have died were it not for the fall, maybe he would have. It's not as though he broke his neck. His injuries weren't consistent with his demise. If a guy falls a couple feet without breaking his neck and dies people are going to rightfully wonder what happened to him. So they did an autopsy and saw that he had been dying of COVID and the shock of the fall likely did him in.
I suspect they've done this kind of stuff everywhere, just only the UK government bothered to spill it.
Meaning, they've accurately linked deaths to COVID. What you're saying is just not true. There weren't non-covid deaths being linked to COVID. People committing suicide and dying in motorcycle crashes weren't listed as COVID deaths. Freakish incidents like with the man in Croatia on the other hand were, and because of how sensational they were, they got circulated widely by pundits trying to deny the reality of the pandemic.
Finland is another example of the same phenomenon in action:
This is just a reiteration of the same distinction of direct deaths and deaths involving COVID.[173]
Hey, let's compare COVID to other diseases. According to the WHO, 6,656,601 died from COVID up until now (December 24, 2022):
That's 3 years, and with fudged stats (but we will give the benefit of doubt to the scaremongers for now).
No, it's not with "fudged stats". You don't understand how cases were counted and likely made no effort to learn how, as it took relatively minimal research for me to understand how it was done. It wasn't some well-hidden trade secret. You claim on your site to have put "hundreds of hours" of work into topics. If that is true, it can only reflect the effort you've put into cherrypicking evidence.
On the other hand - in only one year (2020) - diabetes has killed more people:
>The International Diabetes Federation reported 6.7 million deaths worldwide among adults with diabetes in 2021
That is a problem. Piling millions more deaths and hospitalizations onto that problem only strains the healthcare system and puts everyone's lives in greater danger.
If you extrapolated that, it would be 3 times more deaths than during the whole 3 years COVID has been around. And yet, have you ever heard the mainstream media "informing" you about how many people died a certain day from diabetes, all day every day?
Diabetes is not a communicable disease and can be reliably treated.
>Cancer is a leading cause of death worldwide, accounting for nearly 10 million deaths in 2020.
Again extrapolating, it would be 30 million in those 3 years of COVID, which is almost five times more. Of course, those diseases have been ignored during the "pandemic" because they could not be used to install any kind of restrictions (in fact, their sufferers have been left to rot with the denied doctor visits).
Because of people like you denying the reality of the pandemic, encouraging people to behave recklessly, get themselves sick, and require care, which in turn stressed the system and deprived others of the attention that they deserved. You don't have the right to be using this as an argument against others, this is an indictment of yourself.
Also cancer isn't a communicable disease. The reliability of treatment varies.
Around one-third of deaths from cancer are due to tobacco use, high body mass index, alcohol consumption, low fruit and vegetable intake, and lack of physical activity.
Tobacco-use, obesity, alcohol consumption, lack of exercise, and a poor diet are not communicable diseases. For the most part, an individual can control their exposure to alcohol and tobacco. They can to a degree control their diet, though this is constrained by their socioeconomic status. Obesity is tied to genetics, this is not entirely in one's personal control. Anyway, these things are problems, but they in no way dismiss the significance of COVID.
As we can see, the COVID gun is full of dummy bullets; it can only seem powerful by plagiarising the deaths caused by other viruses, diseases, pollution, age or really any cause
No, people who died of COVID objectively died of COVID. The death toll stands around 7 million globally, but could be as high as 35 million. You've in no way established fraudulent death statistics.
Analyzing contagion
What would you guess is the probability of catching the virus if you live with someone who already has it? According to the media hype, you'd think it's pretty much a certainty. And yet the WHO's report tells a different story:
I've left the WHO report here.[174]
>preliminary studies ongoing in Guangdong estimate the secondary attack rate in households ranges from 3-10%
What about non-family specific close contacts?
As of 17 February, in Shenzhen City, among 2842 identified close contacts, 2842 (100%) were traced and 2240 (72%) have completed medical observation. Among the close contacts, 88 (2.8%) were found to be infected with COVID-19.
>As of 17 February, in Sichuan Province, among 25493 identified close contacts, 25347 (99%) were traced and 23178 (91%) have completed medical observation. Among the close contacts, 0.9% were found to be infected with COVID-19.
>As of 20 February, in Guangdong Province, among 9939 identified close contacts, 9939 (100%) were traced and 7765 (78%) have completed medical observation. Among the close contacts, 479 (4.8%) were found to be infected with COVID-19.
So, 38274 people - who were all in close contact with someone infected - were tested in three different locations, and the overall rate of contagion was a puny 3.1%. To better visualise this: imagine a corona-infected person shaking hands with 100 different people - only 3 of them will catch the virus. Of course, the types and durations of "close contacts" will be different, but you can expect the average contagion rate to be about 3%. For a practical example, check this.
Summarizing: 350 people were traveling from Wuhan to Toronto; one of them was positive for corona (confirmed through 2 different tests, each repeated twice). The flight lasted 15 hours, and despite there being 25 close contacts with the infected person, not one of them caught the virus. UPDATE: found another very well done study which supports low contagion. What the authors did was trace the close contacts of the 100 corona-infected people, locked them up after the last time they've met up during the study period, and checked if they got sick. What were the results?
>In this case-ascertained study of 100 cases of confirmed COVID-19 and 2761 close contacts, the overall secondary clinical attack rate was 0.7%
Amazing - the killer virus can't even muster enough strength to infect 1 person per 100. Anyway - for honesty's sake - the study mostly tested only the people who actually got symptoms. But if the killer virus is sitting in your body harmlessly, what's the problem? Shouldn't the point be to avoid disease instead of a label? However, they did test even some asymptomatic people:
>For high-risk populations, including household and hospital contacts, RT-PCR was performed regardless of symptoms.
For family and household, the contagion rate was somewhat higher - about 5%. This is still 95 out of 100 people living together with a COVID-19 case who will avoid infection. What about some studies that appear to show higher rates? Let's check one out:
>The secondary attack rate of SARS-CoV-2 in household is 16.3%
Oh no, 16%! I'm already hiding under my bed. This study measured only household infections, so it has no relevance to random outside "close contacts". Anyway, even the 16% isn't valid when you consider this gem:
>The quarantined contacts who had symptoms were inspected at least 4 times by SARS-CoV-2 RT-PCR until their tests were positive.
Hahahahaha. So, the way they got this contagion rate is thanks to fraud. Literally - repeat the test until we get the results we want. Thanks for the admission. But how many journalists will pick this bit up? And how many studies just completely avoid mentioning such information? But I digress. Anyway, when a study is properly done (the previous one only had one test per person), COVID-19 fails to show an infectivity worth worrying about. Recall, also, that the virus does not spread by touching surfaces despite what the authorities were scaring us with all this time. Now, to be quite honest, some studies found different results:
What you're saying here is not entirely false. But it's not very well thought out.
The handshake analogy is misleading, as COVID is spread mostly through the air, which dramatically increases your potential to infect others as an individual. Most people don't go shaking the hands of hundreds of people a day. But, many people in their day to day will encounter dozens of different people outside, indoors, in public transportation, and so forth. More than enough to infect at least somebody.
You characterize infection rates of 3.1% and 16.3% as "puny", and laughable, when they are actually very significant on a societal scale, and easily enable the pathogen to continue spreading around.
The figures you're giving speak more to society at large, and less of an individual.
To give an actual idea of an individual's risk of infecting others, look at the R0 metric. It helps to gauge an average person's risk of infecting members of an unimmune populace with a pathogen.[175][176]
In this article, the average R0 of COVID is in the range of 2. This means, on average, one COVID-infected person will infect two other people.[177]
This paper analyzes R0 values in some places around the world, they ranged from above 1 but below 2 in places like Brasil, all the way to above 6 but below 7 in places like China. Still, they seemed to average in the range of 2.[178]
The WHO estimated it as being 1.4-2.5.[179]
>Human-to-human transmission is occurring and a preliminary R0 estimate of 1.4-2.5 was presented
The Spanish flu outbreak of 1918 killed 50 million people worldwide.[180] Its R0 value was estimated to be around 1.4 to 2.8.[181] This is similar to COVID's R0 value.
So, as you see, even with the potential for one person to infect just up to 2 or 3 other people, tens of millions can die.
Have there been excess deaths compared to the usual?
The argument usually goes like: "There were (insert amount) of excess deaths in the year 2020 compared to 2019. The coronavirus provides a perfect explanation. Checkmate, denier!" This is usually used in the context of the US (which has had 350K more deaths in 2020 than expected), but also the UK and sometimes others. The argument sounds convincing on the surface, but falls apart upon closer examination. This is because it relies on the fraudulently counted death statistics which consider chronic disease deaths, flu deaths, old age deaths, or even unrelated deaths as coronavirus deaths. So, when you realize that, all you're left with is a bunch of unaccounted deaths for the year which could be from anything.
Those deaths are not fraudulent. They could not have died from just anything. These people got sick, died, and were confirmed to have had died from coronavirus. What else was it that killed them when their pathology indicated coronavirus killed them? People who died randomly in accidents or from suicides were not being counted as COVID deaths. Nor were flu deaths or other disease deaths. It was people who objectively had been ill with coronavirus. Tests and autopsies would confirm this. The majority of them may have had comorbidities, but that does not negate the fact that COVID caused their death. It's similar to saying guns don't kill people, blood loss and organ damage does. You're rejecting the concept of causality completely.
What you're saying is that people who are elderly or have comorbidities and die should not be counted, which implies that they are less valuable as human beings. The evidence all suggests that people who are elderly, obese, and have comorbidities like heart disease, diabetes, and asthma, for example, are more likely to die of COVID. It's undeniable that young people are significantly less likely to die, but that isn't the point. Most people in America had at least one comorbidity that put them at a higher risk of dying from COVID. And regardless of comorbidities, these people are human beings and don't deserve to die for having them. Short of people being terminally ill, you simply cannot know that a person who contracted COVID and died was going to die anyway. It's a callous outlook.
What was the other common thing between the countries which have excess deaths? The coronavirus response, of course. We know that it increases suicides, poverty and decreases doctor visits for anything other than corona, so that could explain a part of it.
That's not the case, as researchers focused specifically on deaths from natural causes. "Poverty" is very vague, if you mean people dying out in the cold or something, that could have happened, but that's not a natural cause of death. The healthcare system being overwhelmed could have contributed to naturally-caused deaths. If it wasn't overwhelmed, the deaths could have been prevented. This only inculpates responses to the pandemic that threatened to worsen it, like disobeying lockdown measures, refusing vaccines, and so forth. Suicides wouldn't be counted towards the excess deaths as they are an unnatural cause of death. So that also precludes accidents, homicides, and any other unnatural kind of death. The article I've cited below mentions that they focused on natural causes.
Otherwise, it could be any other cause, including something new that we will only discover years later. The point is, we can't use corona as an explanation for the excess deaths when we know the stats have not been accurately collected.
You don't know that they haven't been accurately collected, you've failed to establish this. Going off of the available information, the only inaccuracy could really be in the under-reporting of deaths, as the authorities cannot examine every single dead person.
UPDATE: ha! The detailed data for most countries is now in - and as usual, it reveals yet another beautiful argument of the doomers as an empty husk. Look:
I reverse image searched that chart at Google, Bing, Yandex, and Tineye, and couldn't find its source. So I guess I'll 'do my own research'.
This article from the NIH relayed the findings of a study, which reported up to a million potential excess deaths from COVID.[182]
>To understand how COVID-19 death counts reflect the true impact of the pandemic, a team led by scientists from the University of Pennsylvania, Boston University, and collaborative institutions studied excess mortality from natural causes, i.e., diseases and chronic conditions. Calculations of excess mortality are used to measure the impact of COVID-19 on deaths. Between March 2020 and August 2022, the U.S. had nearly 1.2 million more deaths than expected, with approximately 635,000 in the first year and 544,000 in the second year. Previous studies found that these excess deaths were higher than the reported COVID-19 deaths, but most of that earlier research investigated extra deaths from all causes. In this new study, the scientists focused on natural causes of death, which may provide a better estimate of unacknowledged COVID-19 deaths.
>The researchers employed innovative statistical techniques to examine monthly Centers for Disease Control and Prevention data on natural-cause deaths and reported COVID-19 fatalities across 3,127 counties spanning the first 30 months of the pandemic, March 2020 to August 2022. Their analysis revealed approximately 1.2 million more natural-cause deaths than expected during this period. Of these deaths, nearly 163,000 did not have a COVID-19 notation on their death certificates. The largest gaps between these excess deaths and reported COVID-19 deaths were in rural areas, the West, and the South.
>Increases in reported COVID-19 deaths often coincided with increases in excess natural-cause deaths, but many of the natural-cause ones were likely unrecognized COVID-19 deaths. The correlation between COVID-19 deaths and excess natural-cause deaths suggests that health care delays and social and economic impacts of the pandemic were not the main reasons for these excess deaths. For example, in areas where a greater proportion of excess deaths were assigned to natural causes, there may have been more unrecognized COVID-19 deaths due to less testing, more deaths outside hospitals, and less experienced death investigators. Some areas, such as New England and the mid-Atlantic metropolitan counties, had fewer excess natural-cause deaths compared to reported COVID-19 deaths, possibly due to declines in other causes of death (influenza, for example) due to COVID prevention policies and greater ability to work from home in some more economically privileged counties, or different reporting standards.
>Limitations of the study include the inability to know for certain if the excess natural-cause deaths were due to unrecognized COVID-19 cases or were related to health care interruptions and social and economic impacts from the pandemic. In addition, while death counts were final for 2020 and 2021, the data for 2022 was still provisional. Future research should differentiate unrecognized COVID-19 deaths from other causes and examine the differences based on individual factors, such as age, gender, race, and socioeconomic status, as well as access to health insurance and primary care. Overall, this study helps improve understanding of the pandemic’s true impact and may guide better public health responses and improvements in death investigation systems.
The full text can be found here.[183]
Here's another analysis. It reveals excess mortality predating the pandemic which was amplified by the pandemic. The excess mortality was greater in America than other wealthy countries (HIC = high income country), likely due to America's healthcare system, among other things.[184]
>We obtained all-cause mortality data for the US and 21 other HICs from the Human Mortality Database from January 1980 to December 2023.5 For each year, we computed age-specific mortality rates for the US and the population-weighted average of other HICs. We then calculated the number of US deaths that would have been expected each year had the US population experienced the age-specific mortality rates of other HICs. We computed ratios of observed-to-expected US deaths. We then computed numbers of excess deaths attributable to the US mortality disadvantage by taking the difference between observed and expected US deaths. We stratified by age. Finally, we fit a linear regression model to assess whether the number of excess US deaths in 2023 differed from the 2014-2019 prepandemic trend (eMethods in Supplement 1). Analyses were conducted with Stata/MP, version 18.0 (StataCorp LLC), and R, version 4.42 (R Project for Statistical Computing).
>Results
>Our analysis encompassed 107 586 398 deaths in the US and 230 208 265 deaths in other HICs from 1980 to 2023. We estimate that 14 735 913 excess deaths occurred in the US in this period compared with other HICs. US mortality rose rapidly in 2020 and 2021 during the pandemic, then declined in 2022 and 2023. The pandemic-era mortality surge was less pronounced in other HICs (Figure, A).
>Relative differences between the US and other HICs widened before and during the pandemic, particularly among younger adults, before contracting in 2022 and 2023. Age-standardized mortality rate ratios comparing the US with the average of other HICs were 1.20 in 2010, 1.28 in 2019, 1.46 in 2021, and 1.30 in 2023 (Table). In 2023, mortality among US adults aged 25-44 years was 2.6 times higher than in other HICs (Figure, B).
>Excess deaths attributable to the US mortality disadvantage peaked at 1 008 369 in 2020 and 1 098 808 in 2021, then declined to 820 396 in 2022 and 705 331 in 2023. These numbers followed 4 decades of rising excess deaths, reaching 631 247 in 2019 (Figure, C and Table). In 2023, excess US deaths accounted for 22.9% of all deaths and 46.0% of deaths among US residents younger than 65 years (Table).
>Regression analysis demonstrated that the rising trend in excess US deaths before 2020 continued during the pandemic. Excess deaths in 2023, although lower than in 2020 to 2022, were higher than in 2019 and consistent with the slope established from 2014 to 2019 (Figure, D).
What was killing these people? A pandemic happpens and all of a sudden there's more excess deaths than usual for no reason? There's no causal link? That's ridiculous. All of a sudden the conspiracy theorists believe in coincidences. They do the same thing with global warming. Sea levels, after being basically unchanging for millennia, just decide to rise the same year that the industrial revolution starts, for absolutely no reason. A complete coincidence.
What we're looking at here is up to a million excess deaths.
OWID just reiterates the point I've layed out regarding how deaths are counted.[185] The site reports that at least 7 million people worldwide died of COVID.
>In many richer countries, the vast majority of deaths are reported with an ‘underlying cause of death’ listed on their death certificate.
>Determining this underlying cause is challenging in many cases. Health problems are often connected and can interact, meaning that multiple conditions can ultimately result in death. Or one underlying condition can result in multiple complications, and each can trigger death.
>Health or legal professionals are responsible for filling out a death certificate. To do this, they determine the chain of events that led to the death using medical records, circumstances, national guidelines, and other knowledge. They can write up to four steps in the chain leading to death and should use as precise language as possible, but can mention if they believe a cause is ‘probable’.
>Hospitals or health departments then collect data from death certificates, which are compiled by the country’s national vital registry. The ‘underlying cause’, listed in the last step of the chain, is converted into a death code. Countries may have slightly different procedures for precisely converting which death codes; for example, they may use additional information about each deceased person.
>The death codes follow the classifications in the International Classification of Diseases (ICD) guidelines.
>This data is then submitted to the WHO annually. It tends to be delayed as it takes time for health or legal professionals to determine the causes of deaths, especially sudden or unexpected deaths, and for departments to compile this data from across the nation.
>In poorer countries, this process may be limited or lacking because of a lack of medical testing and records, health and legal professionals, hospitals, and vital registries.
>The process described above also takes place for deaths caused by COVID-19.
>But determining the cause of death for respiratory infections, such as COVID-19, can be complicated because they can lead to a range of complications such as pneumonia, acute respiratory distress syndrome (ARDS), and heart failure.
>So, how are deaths from COVID-19 reported? What is and isn’t included in these totals?
>As is standard in death reporting, countries are asked to follow the cause of death classifications from the WHO’s International Classification of Diseases guidelines.1 However, countries also typically provide their own guidance to practitioners on how and when COVID-19 deaths should be recorded on a death certificate.
>Let’s take a look at two concrete examples of national guidance: the United States’s guidance (in the CDC’s Vital Statistics reporting guidance, published 2023) and the United Kingdom’s guidance (in the Office for National Statistics’s guidance, published 2022). Both provide very similar guidelines for medical practitioners on the completion of death certificates.2
>Both guidelines state that if the practitioner suspects that COVID-19 played a role in an individual’s death, it should be specified on the death certificate. In some cases, COVID-19 may be the underlying cause of death, having led to complications such as pneumonia or ARDS, so COVID-19 should be listed.3
>Although confirmed cases are reliant on a positive laboratory confirmation of the COVID-19 test, a laboratory diagnosis may not be required for it to be listed as the cause of death.
>The UK’s guidelines, for example, make clear that practitioners should complete death certificates to the best of their knowledge, stating that “if before death the patient had symptoms typical of COVID-19 infection, but the test result has not been received, it would be satisfactory to give ‘COVID-19’ as the cause of death, and then share the test result when it becomes available. In the circumstances of there being no swab, it is satisfactory to apply clinical judgement.”
>This means a positive COVID-19 test result is not required for a death to be registered as COVID-19. In some circumstances, depending on national guidelines, medical practitioners can record COVID-19 deaths if they think the signs and symptoms point towards this as the underlying cause.
>The US CDC’s guidelines also make this clear with an example: the death of an 86-year-old female with an unconfirmed case of COVID-19. It was reported that the woman had typical COVID-19 symptoms five days prior to suffering an ischemic stroke at home. Despite not being tested for COVID-19, the coroner determined that the likely underlying cause of death was COVID-19 given her symptoms and exposure to an infected individual.
Strokes have been associated with COVID infection. While in that example it was the stroke that killed the old lady, it was likely COVID that precipitated the stroke. Strokes don't just happen for no reason, they have some sort of mechanistic cause. Everything has a cause. Given that COVID has been associated with strokes, and the time of her infection until death, it is not much of a stretch to surmise that her death was caused by COVID prior to confirmation. Regardless, cases like that are rare.
Here's how the CDC counted deaths: [186]
A physician, medical examiner, or coroner fills out a death certificate.
>Part I and II of a death certificate ask what caused a death and what other factors contributed to it. If COVID-19 appears among the causes and contributors, CDC guidance counts that as a COVID-19-related death.
>Part I asks for the “immediate cause” of death, followed by any “conditions that led to the immediate cause,” the CDC explains in guidelines for certifying COVID-19 fatalities. For example: In some COVID-19 cases, the immediate cause is an affliction that arose from the disease, such as pneumonia, while COVID-19 gets listed under that as an underlying condition that led to death. In other words, COVID-19 caused the pneumonia.
>Part II asks for conditions that did not set off medical events that led to death but contributed in some other way. Here, COVID-19 appears as sort of an accomplice to a fatality that was probably going to occur from something else (such as a preexisting, terminal disease), albeit later than if the person had not contracted COVID-19.
>For instance: In Aiken’s example of a patient near death from Alzheimer’s disease before contracting COVID-19 (which she described as taken from several cases, not one in particular), COVID-19 would be a contributing condition, not a cause. “She was already in decline, had a short life expectancy, and COVID-19 may have tipped her over, but just barely,” Aiken says.
>COVID-19’s role in a death is perhaps most clear in an ICU. By the time COVID-19 patients get there, they are suffering severe symptoms of the disease and have probably tested positive for it.
>“They might die from septic shock,” Auld says, referring to a faulty immune response that can cause tissue damage and organ failure and has been linked to COVID-19. “But when you go back to the reason they came to the hospital and got so sick, it’s COVID. If you go back to the root cause, it’s COVID.”
>The assessment is often less clear in emergency departments. Some patients there are treated with no time to test them for COVID-19, notes Ali Raja, MD, MBA, MPH, executive vice chair of the Department of Emergency Medicine at Massachusetts General Hospital. Some do show obvious and severe COVID-19 symptoms or have a previous diagnosis of the disease.
>“We put that [COVID-19]” on the death certificate in those cases, he says.
>Others, however, have no COVID-19 symptoms or previous diagnosis. For those who die — from a heart attack, for instance — the role of COVID-19 might never be determined unless there’s a reason to run a post-mortem test for the disease, Raja explains. As for those killed by traumas such as accidents and assaults, a test wouldn’t matter.
>“Whether or not you have COVID isn’t going to change your cause of death when you get hit by a car,” he says.
>The CDC uses different sources to post slightly different fatality figures.
>Death certificates provide the data for the agency’s daily updates of COVID-19 deaths. In mid-February, the total stood at 462,000.
>At the same time, the agency’s COVID Data Tracker reported 486,000. That data comes from the National Notifiable Diseases Surveillance System (NNDSS), which gathers information from state and local health departments when a disease is diagnosed in someone in a health care setting. (Estimates vary among media outlets and other organizations because they use various sources, including the CDC.)
>Why use two counting methods? The NNDSS provides “real time” awareness of fatalities linked to a disease, Robert Anderson, PhD, chief of the Mortality Statistics Branch at the CDC’s National Center for Health Statistics, says via email. He explains that it takes about two weeks longer for death certificate information to work its way up to the daily updates.
The CDC's method is basically the same as the UK's method.
>“Ultimately, the official numbers will be based on the death certificates,” Anderson says.
>Nevertheless, the official numbers don’t capture all COVID-19 deaths, for several reasons.
>When tests for COVID-19 were scarce while the pandemic raced across the country in the spring of 2020, many infected people died without being tested. That includes those who showed mild symptoms or symptoms that were attributed to other causes.
Some further information from the CDC: [187]
>Provisional death counts deliver the most complete and accurate picture of lives lost to COVID-19. They are based on death certificates, which are the most reliable source of data and contain information not available anywhere else, including comorbid conditions, race and ethnicity, and place of death. >The National Center for Health Statistics (NCHS) uses incoming data from death certificates to produce provisional COVID-19 death counts. These include deaths occurring within the 50 states and the District of Columbia.
>NCHS also provides summaries that examine deaths in specific categories and in greater geographic detail, such as deaths by county and by race and Hispanic origin. >COVID-19 deaths are identified using a new ICD–10 code. When COVID-19 is reported as a cause of death – or when it is listed as a “probable” or “presumed” cause — the death is coded as U07.1. This can include cases with or without laboratory confirmation.
>Provisional death counts may not match counts from other sources, such as media reports or numbers from county health departments. Counts by NCHS often track 1–2 weeks behind other data.
>Death certificates take time to be completed. There are many steps to filling out and submitting a death certificate. Waiting for test results can create additional delays.
>States report at different rates. Currently, 63% of all U.S. deaths are reported within 10 days of the date of death, but there is significant variation between states.
>Provisional counts are not final and are subject to change. Counts from previous weeks are continually revised as more records are received and processed.
So, like I said, they weren't counting random deaths as COVID deaths. It's people who objectively had COVID when they died, which most likely killed them. They aren't just going off of hearsay. Laboratory tests are conducted. Autopsies are conducted. It's not like a doctor looks at a dead guy and says "Eh, he must've had COVID", and writes it down on the death certificate. A medical investigation is conducted first. The evaluations take 1-2 weeks to make. First, they have an initial determination and that goes to one death statistic. Then, they conduct a more-thorough investigation and determine what really caused the death, and that goes to an official death count.
The media may have been using death rates to scare people, I won't deny that, but that speaks to the media. There may have been inaccuracies with the reporting of deaths at the time as well. But that comes down to fearmongering. People shouldn't make wild assumptions off of imperfect surveillance systems, but people did, which is their problem, not the authorities'. The authorities are only guilty for not regulating the media.
Now that the pandemic has been over for a considerable amount of time, we probably have accurate death statistics. Enough time has passed for incorrect data to be corrected and further investigations to be conducted. The death count stands at a minimum of 7 million dead worldwide.
Sweden versus Belarus (The Panic Destroyer)
Sweden's death rate is a little over 10% of all corona cases! This has been used by the media as proof that it's their lax response which has caused the deaths. Let's bust that claim right open
Similar to Italy - it's just old people yet again. I suspect a bunch of "co-morbidities" as well, but I don't think we have such great data proving that as from Italy
Showing again just how callous COVID deniers can be. Do you not hear what you're saying? Your reasoning is literally:
This is really bad.
Anyway - why is this significant? Because Belarus' response to the coronavirus was even weaker than Sweden's!
You're trusting the capabilities of Belarus' government, which showed little care for COVID, to accurately track it, which is nonsensical. Belarus was widely criticized for appearing to not have accurately tracked the disease in their country. Internal reports on the state of affairs in Belarus contrast heavily with the mild figures the image you've shared displays. The internal reports showed that their medical system was strained during the pandemic.
This article details regional reports of strained hospitals, large numbers of patients and deaths: [188]
>In Belarus, about a third of the total bed capacity has been repurposed to provide care to patients with COVID-19, the Ministry of Health reported. In the regions, people are hospitalized in city infectious diseases hospitals; in some medical centers, a number of departments are being repurposed to receive patients. The Zerkalo.io portal decided to look at the situation with COVID-19 infection in areas of six regions according to regional media reports.
>Almost all local publications in the Minsk region urge residents to get vaccinated, but not everyone has the latest data on the number of coronavirus cases in the region. Based on the data from the “districts” from October 4 to October 8, the situation with COVID-19 in the region is as follows:
>Borisov district: coronavirus incidence is not decreasing
>According to the head physician of the Borisov Central District Hospital, Alexander Drozd, as cited by the Adzinstva newspaper, the incidence of COVID-19 is not decreasing. To help people with probable (confirmed) cases of COVID-19 and pneumonia, the departments of Borisov Hospital No. 2 and the “infectious diseases” department, which is part of it, have been temporarily repurposed. There are more than 250 patients in the “red zone” here.
>Report from the “red zone” of Borisov Hospital No. 2:
>Dzerzhinsky district: more than 100 people hospitalized
>In the Dzerzhinsky district, “the situation is difficult, but controllable.” More than 700 patients are being treated on an outpatient basis for coronavirus in the region, over 100 are hospitalized, dzr.by writes.
>“At the same time, about half of those hospitalized need oxygen support and more intensive therapy,” notes Igor Shamal, chief physician of the Dzerzhinsk Central Regional Hospital. “Unfortunately, against this background, we are seeing serious exacerbations of chronic diseases, as well as an increase in the number of heart attacks and strokes, where the trigger is also coronavirus. Up to 10% of patients with Covid pass through the intensive care unit (previously there were significantly fewer such cases).
>Zhodino: wards are 100% full
>According to the deputy chief physician of the Central City Hospital, Olga Kosovets, since October 1, 120 beds have been allocated at the medical institution for the treatment of patients with COVID-19, plus nine intensive care beds.
>“All 22 wards and intensive care units are 100 percent full,” reports Zhodzinskiy News. Of the sick, the publication notes, only a few have been vaccinated. >Krupsky and Berezinsky districts: the situation is unstable
>In the Krupsky district, “the epidemiological situation regarding the incidence of coronavirus infection remains unstable,” the local “district” figuratively describes the situation.
>In the Berezensky district the situation is also not the simplest. In an interview with Byarezinskaya Panarama, general practitioner of the local central district hospital Maria Vasilevskaya said:
>— In the morning, three doctors see patients in the “red zone”, and two in the evening. […] One doctor must examine an average of 30 patients per day. You also need to go to calls, and there are never less than 10 of them a day; today there are 19 in total.
>Myadel district: the situation is “very tense”
>There are no recent data with figures for the region for the last week. In an earlier interview with the Narachanskaya Zara newspaper, acting. The chief physician of the Myadel Central District Hospital, Andrei Polyagoshko, said that the situation with COVID-19 in the area is “very tense.”
>“During the period from September 9 to September 30, the number of patients with confirmed coronavirus infection in outpatient treatment increased 6 times, with pneumonia - 4 times,” the doctor cited the figures. — The reception rooms for patients with fever are operating at the limit of their capacity.
>Volkovysk district: the situation is unfavorable
>In the Volkovysk region, the coronavirus situation is “unfavorable and unstable,” the district’s chief sanitary doctor, Maxim Zhukovich, said at the beginning of the week.
>— Over the last calendar week in the Volkovysk region there has been an increase in the incidence of coronavirus infection by 2.1 times, pneumonia by 1.5 times, and an increase in the contribution of adults to the structure of acute respiratory infections to 43.7 percent of the number of registered cases over the last week. These indicators clearly indicate a deterioration in the epidemiological situation.
>Zhukovich noted that in the last two weeks, almost half of the cases have been registered in patients aged 30-49 years.
>Grodno: they offer vaccinations to the homeless and repurpose new institutions
>In the media, doctors and officials note that the number of cases is increasing. Thus, in Grodno, six medical institutions were repurposed to receive patients: the regional clinical cardiology center, city hospital No. 2, the regional infectious diseases clinical hospital, the regional clinical hospital for medical rehabilitation, the regional clinical center “Phthisiology” and a department at the university clinic.
>In early October, the Grodno Plus TV channel visited the “red zone” of the local infectious disease.
>The hospital had a hundred beds for Covid patients, all of them were occupied. Half of the patients are in serious condition and receive oxygen subsidies.
>— A new patient will take the place of the discharged patients in the evening. And we don’t even know what condition he is in; perhaps he will be in a more serious condition. And, as practice shows, they are not vaccinated,” said the chief doctor of the infectious diseases hospital, Natalya Malashko.
>In the second city hospital, three departments (cardiology, therapeutic and pulmonology) provide care to patients with COVID-19. There are also no free places.
> — Our hospital is filled with 180 patients. Of the 180, only one or two patients received the full dose of the vaccine. The rest are not vaccinated,” said Svetlana Lozovik, deputy chief physician of Hospital No. 2.
>From October 8, the institution planned to add additional diagnostic beds, where patients with a presumptive diagnosis of COVID-19 will be admitted, and will also provide the opportunity for follow-up treatment.
>The Chief Sanitary Doctor mentions that in Mogilev itself, five hospitals are currently used to treat coronavirus patients. At the same time, there are no statistics on recent or relatively new cases of the disease and their number either in the local press or on the website of government agencies. We only know that five days ago Health Minister Dmitry Pinevich visited the city on a working trip.
>“The situation now is difficult, although predictable, its complexity lies in the fact that the high incidence rate has been maintained for quite a long time,” he noted during the business trip. — Of course, this is accompanied by the hospitalization of patients with pneumonia in hospitals in all regions. And Mogilevsky is no exception here. Therefore, the main task now is vaccination and compliance with preventive measures.
>Belynichi district: the situation has been difficult since September
>In the Belynichi district, the situation with coronavirus was difficult back in September. Moreover, the latest detailed information on this matter was published at the very beginning of last month. Even then, the local publication “Zara nad Drutstyu”, citing the chief doctor of the hospital, reported that the incidence rate in the area was 274.5 per 100 thousand population and was one of the highest in the Mogilev region. For comparison, the average number of cases in the region was 152.5.
>Dokshitsy district: increase in coronavirus cases by 2.5 times
>In addition, the Dokshitsy district media reported a 2.5-fold increase in coronavirus cases. Doctors add that the number of young patients in the regional hospital is growing - their number is 60% of all patients. District doctors urge people to get vaccinated and explain: among the people who have been vaccinated, no one is on a ventilator.
I was omitting quotes relating to vaccination, but I'll add this one. Repeatedly throughout the article doctors stress the effectiveness of the vaccines
>— If we take comparative statistics, then only 3.5% of cases are among vaccinated patients. Of this number, only 0.15% were hospitalized. The rest suffered a mild coronavirus infection while undergoing outpatient treatment,” comments Sergei Kubor, head physician of the Central Regional Hospital.
This study finds excess mortality to have jumped by 29-39% during the pandemic, and found a 149% increase in searches for things like coffins and funeral services: [189]
>Excess mortality in Belarus during the COVID-19 pandemic as the case study of a country with limited non-pharmaceutical interventions and limited reporting
>Depending on the model, the Belarusian mortality for June of 2020 was 29 to 39% higher than otherwise expected with the corresponding estimated excess death was from 2953 to 3690 while the reported COVID-19 mortality for June 2020 was only 157 cases. The Belarusian excess mortality for June 2020 was higher than for all neighboring countries with an excess of 5% for Poland, 5% for Ukraine, 8% for Russia, 11% for Lithuania and 11% for Latvia. The relationship between Google Trends and mortality time series was studied using Granger’s test and the results were statistically significant. The results for Google Trends searches did vary by key phrase with the largest excess of 138% for April 2020 and 148% for September 2020 was observed for a key phrase “coffin”, while the largest excess of 218% for January 2021 was observed for “funeral services”. In summary, there are indications of the excess overall mortality in Belarus, which is larger than the reported COVID-19-related mortality.
This statistical analysis suggested that Belarus capped the amount of daily infections they would report at 1,000: [190]
>Some cases of interest appear among the countries with officially lower total infection counts. The Belarus (BY) case is present in all four tables (Tables 1–4). The least noisy Belarusian counts curve appears in Figs. 8 and 9. As with the other panels in the daily counts figures, the vertical axis is set by the data instead of starting at zero, in order to best display the information on the noise in the counts. With the vertical axis starting at zero, the Belarus daily counts would look nearly flat in this figure. They appear to be bounded above by the round number of 1,000 SARS-CoV-2 infections per day, which, again, as in the case of India, could appear to be a psychologically preferred barrier. Media have expressed scepticism of Belarusian COVID-19 related data (Kramer, 2020; AFN, 2020).
Hackers deduced the mortality rate from citizen data that they stole from the Belarusian authorities. Around 32,000 people are believed to have died.[191]
>Excess mortality – 32 thousand people. Belarusian authorities repeatedly underestimate statistics during the coronavirus epidemic - leaked data
>Present Time conducted a study of data received from “CyberPartisans” - hackers who claimed to have hacked the “Passport” system in Belarus. It shows that from March 2020 to March 2021, excess deaths in the country amounted to 32 thousand people - 14 times more than the authorities reported.
>The information analyzed in this article was obtained by hacking an array of personal data of citizens of Belarus. The use of malicious programs in the Criminal Code of Belarus is punishable by up to 10 years, and unauthorized access to computer information is punishable by up to two years. The Ministry of Internal Affairs of Belarus did not respond to a request from Current Time regarding this hack.
>“Cyberpartisans” - anonymous Belarusian hackers who announced support for protesters in the country, in July 2021, spoke about the hacking of a data array with all the personal data of Belarusians - the Passport information system. The editors of Present Time then managed to confirm the hack: upon request, the hackers sent the data of two citizens of the country (who agreed to participate in the experiment at the request of journalists), including their photos and technical information from their passports. This non-public information came to the “CyberPartisans” as a result of the special operation “Heat” - they claim that they physically penetrated the facilities of the Ministry of Internal Affairs of Belarus, “opened several accesses” to internal networks and “continue to work in them”, despite the authorities’ attempts to stop the leaks.
>Now “CyberPartisans” have shared with Present Time an array of personal data of 1.4 million Belarusians who died from January 2010 to March 2021. >How we verified the authenticity of the leak
>To make sure that the data array is reliable and contains information about people who actually died during this period, the editors first selected from the list provided by CyberPartisans random birth dates of those who died in the last 10 years - the first day of each month of 1989. The sample included 54 people. We made sure that there was no one among them who continued to run social networks; many had condolences from friends and relatives published on their pages.
>The array contains the names and data of a variety of Belarusians: the founder of an opposition website (found hanged in 2010), a rock musician (died in 2018), a former prime minister (died in 2020) and the former primate of the Belarusian Orthodox Church (died of COVID-19 in 2021). In addition, we took from the website “Remember.online” the names of people who are buried in different cemeteries in Belarus, and also obtained an almost one hundred percent match with the data from the leak.
>Before the coronavirus epidemic, mortality data from the AIS “Passport” differed little from what was published by the National Statistical Committee of Belarus (Belstat). Here is a tentative explanation for this small discrepancy in the numbers: the tables from the passport system show that in approximately 20% of cases, police officers did not enter the date of death into the database - then we used the date the information was entered into the death registry for the calculation. Thus, according to data from the merged passport system, 121,515 people died in Belarus in 2019, and according to Belstat – 120,913 people.
>Belstat has not published new mortality data since June 2020. In the AIS "Passport" leak, the data ends on March 31, 2021. Prior to this, November, December and January show record monthly mortality rates compared to data from at least 2008 (the earliest data available on the UN website, where Belstat sends it monthly). In 2020, based on the leak, 145 thousand people died in Belarus - this is the highest figure in the post-war history of the country, except for 2002, when due to various demographic circumstances, primarily the aging population, 146 thousand died. For comparison: in Russia, the record mortality rate occurred in 2003.
>How many people have died from coronavirus? Officially, in 2020 – 1,424 people, and by the end of March 2021 – 2,247. But according to excess mortality rates (the “gold standard” by which the scale of the coronavirus epidemic is determined), it is an order of magnitude higher. In Belarus in 2020, excess mortality amounted to 25 thousand people. This is the actual mortality rate (145 thousand) minus the predicted mortality rate based on data from previous years (120 thousand).
>25 thousand people in 2020 is 17 times more than the Belarusian authorities say.
>Excess mortality from the end of March 2020 to the end of March 2021 amounted to 32 thousand people. This is 14.4 times more than official data shows.
>“The indicator is exactly the same as it was before this leak based on data until June 2020,” Dmitry Kobak, a data analyst from the University of Tübingen (Germany), who collects data on excess mortality in different countries, tells Present Time. “That is, they are underestimating quite consistently. For 100 thousand people, this amounts to 340 deaths. This puts Belarus in 10th place in our database. Basically, close to neighboring countries: Lithuania (370), Russia (420). In Ukraine there are fewer (210)."
>But this is data until the end of March 2021, the expert notes. If the Belarusian authorities continue to hide real deaths in the same proportion, then we can talk about record figures. “If we take the undercount factor of 14.4 and extrapolate from official deaths today, we get more than 500 excess deaths per 100 thousand population - this is higher than all countries in Eastern Europe and Latin America, with the exception of Peru. Excess mortality shows a wave in May-June 2020, then a winter one: October-November-December-January, then a fall in As of March 2021, excess mortality is approximately zero. In Russia, it seems that a new surge in excess mortality occurred in June-July 2021,” the expert notes.
>The same indicators based on data from the AIS “Passport” are given by Andrei Eliseev, research director of the Warsaw analytical Center EAST: “If this figure can be trusted, and it fully corresponds to my assessment made from fragmentary data at the beginning of the year, then the excess mortality in Belarus for 2020 was about 25 thousand people, which is 20% higher than the normal figure. This indicator reflects the real mortality from coronavirus. It is 17 times higher than the official figure, according to which less than one and a half thousand people died from coronavirus in 2020. Firstly, this indicates colossal manipulation of statistics. Secondly, this means that Belarus is one of the European countries most affected by the coronavirus (in the European Union, excess mortality averaged 12%). This is completely refutes the messages of state propaganda about the “corona catastrophe” in Western countries and the best method of combating the epidemic in Belarus. Thirdly, given the very slow progress with vaccination, the consequences of the epidemic for the period 2020-2021 for Belarus will inevitably turn out to be even more dire in the regional perspective."
Excess deaths in Mogilev.[192]
Almost 2 times more people died in Mogilev in November than in November 2019:
>In November 2020, more than 580 deaths were registered in Mogilev - the information of the registry office department was published on the website of the city executive committee. In November 2019, almost 2 times less people died - about 330.
>Accurate monthly mortality statistics are difficult to determine: the registry office publishes data by week, not by month: for example, from November 30 to December 5. However, according to the published data, it can be seen that
>that if a year ago in November the number of deaths in Mogilev each week did not exceed 80, then in November 2020 between 122 and 163 deaths per week were registered.
>According to statistics, from January to November 2020, 4,375 people died in Mogilev. This is 609 more people than in the whole of 2019 (3,766 deaths), Euroradio reports.
>At the same time, in the last 5 years, the number of deaths in Mogilev per year did not exceed 3.8 thousand people. That is, more people died in 11 months of 2020 than in any entire year since 2016.
>About 350 deaths were registered in Mogilev in two thirds of December.
Excess deaths in Mogilev.[193]
>In November 2020, 1.8 times more people died in Mogilev than in November 2019. The Mogilev Registry Office is the only one in the country that publishes such statistics on mortality.
>577 people died in November 2020, and 320 in the same period last year. It is difficult to explain the difference of 257 people with anything other than the consequences of the COVID-19 pandemic.
>According to the official statistics of the Ministry of Health, only 177 deaths related to the coronavirus infection were recorded throughout Belarus in November 2020.
Doctors anonymously testify that they witnessed more deaths in their hospitals per day than were reported daily by the government: [194]
>"District anomaly"? The number of people who died from COVID-19 in Belarus may be underestimated by seven times
>Three doctors explain why the official statistics about the coronavirus epidemic in Belarus are clearly false.
>Dr. S. Bobruisky (he asked to remain anonymous, the editors know his name) had access to district data on the number of people infected with COVID-19 and those who died from the disease. The documents he presented to Radio Svaboda show that in the area where a little more than 2 percent of the population of Belarus lives, more than 8 percent of all officially recognized cases of COVID-19 were registered, as well as more than 18 percent of all nationally recognized deaths from this disease.
>In 2020, 16,309 cases of COVID-19 were officially registered in Bobruisk and Bobruisk district. This is 6,998 infections per 100,000 inhabitants. About 7% of the district's population suffered from the disease — every 14th person.
>At the same time, according to the figures of the Ministry of Health as of December 31, 2020, 194,284 people fell ill throughout the country during the same period.
>According to Belstat data, it is only 2,065 per 100,000 inhabitants, approximately 2% of the population of Belarus - every 50th.
>If we take the figures for the year from February 28, 2020 to February 28, 2021, 287,306 people (about 3% of the population) officially fell ill across the country, and in one city of Babruysk — 21,059 people (about 10% of its population)
>"There was a period when 30-40 new cases of coronavirus were registered in Bobruisk every day, and about 300 were registered throughout the country," says Dr. S. "I asked the chief doctor of the Bobruisk Hygiene Center: 'Is every tenth case in Bobruisk? It's impossible.' He answered me: "Don't get into it, it's not my question."
>"We had 3-5 people die, and 7-9 deaths were announced all over the country"
>According to Dr. S., requests from newspapers and Internet resources for figures for Bobruisk were rejected with the answer that everything is "like the average for the republic, measures are being taken."
>However, in reality, the numbers did not match the official figures for the country at all, he says. In Bobruisk alone, more than 360 people died of COVID-19 during the year of the epidemic (from February 28, 2020 to February 28, 2021). If these numbers are projected onto the entire country, the total number of dead should be around 16,000.
>At the same time, according to the figures of the Ministry of Health as of February 28, 2021, 1,976 people died from COVID-19 during the entire pandemic.
>Ultrasound diagnostics doctor Anna Styapanova, who worked at the 1st hospital in Minsk, also talks about the strange ratio of the dead: "Only in our hospital, 3-5 people died in the covid wards every day, precisely from COVID-19. At the same time, at that time, 7, 8 or 9 deaths from the coronavirus were officially reported across the country."
>Both doctors note that the official death rate in the country among registered patients with COVID-19 for the year from February 28, 2020 to February 28, 2021 was suspiciously low — only 0.69%. And this despite the fact that the nationwide official number of patients appears to be greatly underestimated.
>In Babruysk, during the same time, the mortality rate was 1.72% of the number of patients.
>We appealed to the Ministry of Health with a request to comment on statistical anomalies with the number of patients with COVID-19, but we have not yet received a response.
>"We were limited in the number of tests"
>Both Dr. S. and Anna Stepanova say that, at least at the local level, statistics on the number of patients and deaths from COVID-19 were mostly collected honestly. However, people with symptoms of the disease were often not tested, but simply recommended to self-isolate.
>Dr. K., who in 2020 worked as a therapist in one of the clinics in Minsk, explains: "Last fall, 30-40 patients came to me during my shift, and about half of them, very likely, had covid. But we were actually limited in the number of tests - a maximum of 10. Usually I sent 5-7 people for tests, and almost all of them were diagnosed with the disease."
>Both Dr. S. and Anna Stepanova say that, at least at the local level, statistics on the number of patients and deaths from COVID-19 were mostly collected honestly. However, people with symptoms of the disease were often not tested, but simply recommended to self-isolate.
>Dr. K., who in 2020 worked as a therapist in one of the clinics in Minsk, explains: "Last fall, 30-40 patients came to me during my shift, and about half of them, very likely, had covid. But we were actually limited in the number of tests - a maximum of 10. Usually I sent 5-7 people for tests, and almost all of them were diagnosed with the disease."
>Dr. K. adds that in those days, when it was officially announced about 7-8 deaths per day throughout the country, his colleagues from Minsk hospitals told him about 3-5 deaths in each.
>He also says he personally filled out a card for a deceased patient who apparently died of COVID-19 and tested positive for the coronavirus, but was listed as a pneumonia death.
This article estimates that the population of Belarus decreased by 47.8 thousand people over the course of COVID: [195]
>Belstat published population data for 2020. However, it did it in a strange way. But if you apply some mathematical calculations, the same terrible truth will be revealed - about 30 thousand people probably died from the coronavirus in Belarus.
>The Kastrychnitsky Economic Forum writes about how they managed to reach this terrible figure.
>“With today’s (March 9, 2021) post, we would like to thank Belstat for publishing population data for 2020. Finally, you did it - though in a slightly strange way... There is a whole layer of “per capita” indicators. Realization of this fact forced us to rummage through the Belstat website, and we discovered a wonderful indicator “retail trade turnover per capita, rubles.” And another - “retail trade turnover, million rubles.”
>If we divide the second indicator by the first, we get the average population for the year. The discrepancy between this calculated indicator and the actual data is minimal - from 2 people in 2014 to 113 people in 2016 (in 2018 and 2019 - 8 people in one direction or the other).
>So, a simple calculation shows that the average annual population in 2020 was 9417.9 thousand people (plus or minus a few dozen people).
>In 2019, the average annual number was 9465.7 thousand people, in 2018 – 9483.5 thousand people, in 2017 – 9498.3 thousand people.
>That is, if in 2018 the population decreased by 14.7 thousand people, in 2019 - by 17.8 thousand people, then in 2020 the average annual number decreased by 47.8 thousand people.
>We cannot say anything about why the population decline accelerated so much, but the fact is that in 2020 the population decreased by 30 thousand “above the norm,” if we take the dynamics of 2019 as the “norm.”
>What's the problem with this metric? In 2019, a census was carried out, after which the population in Belarus turned out to be noticeably lower than current census data.
>According to data updated taking into account the census, as of April 1, 2020 (the most recent published data), the population of Belarus was 9397.8 thousand people. In other words, the average annual number of 9417.9 thousand people is the number calculated without taking into account adjustments to the census results.
>Obviously, Belstat has not yet adjusted the data on the average annual population for the decade between the 2009 and 2019 censuses, so to calculate retail turnover “per capita” it simply used the old data series, adding to it the negative increase in 2020, thereby ensuring comparability.
>Thus, from the published data on retail trade turnover per capita, we can only learn that over the past year, on average, the population of Belarus decreased by 47.8 thousand people.
>This is not a net reduction for the year (from January 1, 2020 to January 1, 2021), but you can definitely get a general idea of what happened with mortality and birth rates last year from these data. It’s a pity that in this way...”, conclude the analysts of the Kastrychnitskaya Ekanamichnag Forum.
>And the main conclusion is that in 2020 the population decreased by 30 thousand “above normal”, and as WHO representatives explained last year, all so-called excess mortality should be counted as mortality from coronavirus.
This article reports that in Belarus more deaths were reported on a regional level than on a national level, implying that the national government wasn't counting deaths entirely; that mortality increased by 29% during the pandemic; and that the largest increase in mortality occurred among older people.[196]
>Official reports from the Ministry of Health on the number of people infected with coronavirus and those killed due to it are very different from the data that officials themselves collect for internal use. In 2020, more people were infected and died in Minsk than the Ministry of Health reported for the entire country - this was shown by data from Minsk registry offices and health care institutions, to which Mediazona received access. It follows from them that over the past year, five thousand more people died in Minsk than usual - the mortality rate increased by 29%. And the main victims of the epidemic were people over 60 years of age.
>The first victim of the coronavirus epidemic in Belarus is officially considered to be 75-year-old actor of the Yakub Kolas Theater Viktor Dashkevich - he died on March 31, 2020 in Vitebsk. Throughout 2020, 1,433 people died from COVID-19 in the country—this is official data from the Ministry of Health.
>The materials used in this publication come from three different sources. One source provided Mediazona with a table with data from Minsk registry offices on mortality in 2020 - it contains, among other things, information about the name of the deceased, the dates of his birth and death, and the registration number of the death certificate. Some deaths in the table were duplicated, some more people died at the end of 2019 - we deleted these lines. We checked randomly selected deaths - looked at publications in the media and social networks, contacted relatives and friends. In all cases the data coincided.
>The information on deaths in November and December 2020 in this table coincides with the mortality data obtained from the registry office of the main department of justice of the Minsk City Executive Committee (they were provided to the editorial office by another source). These tables, entitled “Report to Medical Statistics,” contain more detailed information about those who died in Minsk from November 5 to December 30 - among other things, the cause of death is indicated there (including coronavirus).
>The third archive, obtained from another source, contains emergency notifications of COVID-19 cases identified in all medical institutions in Minsk from the beginning of June to the end of November. It lists sick patients, the dates of their registration at the Center for Hygiene and Epidemiology, and much more. A doctor at a city clinical hospital confirmed that the data in his institution’s database coincides with the information in our archive. We also contacted randomly selected people from the list - they confirmed the correctness of the data about the time and place of registration of coronavirus.
>The information in all tables is the numbers that Belarusian officials definitely have at their disposal. They allow us not only to draw conclusions about how the coronavirus epidemic unfolded in Belarus last year, but also about how official reports from the Ministry of Health compare with reality.
>More cases of coronavirus were registered in Minsk every day than officially in the country
>Doctors interviewed by Mediazona explained that every institution that has identified a patient with an infectious disease - and this is not just coronavirus - sends an emergency notification to the district center of epidemiology and hygiene every day. From there the information is sent to the Minsk city center.
>The basis for the diagnosis of COVID-19 can be not only a positive PCR test, but also a computed tomography scan, as well as the presence of antibodies in the body, doctors say. That is, some cases of coronavirus were registered “retrospectively” in patients who had already recovered by that time.
>The Ministry of Health publishes data on new cases of coronavirus daily on its telegram channel - and if you compare these figures with data received from the source on identified cases of infection, it turns out that in reality, more infected people were registered in Minsk every day than in the whole country, according to the official version of the authorities.
>The Ministry of Health claims that from July 5 to November 29, 88,753 patients with coronavirus were registered throughout the country - including Minsk. While emergency notifications for Minsk alone for the same period report at least 101,966 sick people.
>At the same time, our data is missing six days from this period. Based on the figures for neighboring dates, it can be assumed that about 4 thousand more cases of COVID-19 were identified during these days.
>The numbers on the graph are smoothed using a centered moving average - this means that each specific point represents the average value over seven days (the current one, the previous three and the next three). This was done in order to smooth out the image, since on weekends the number of sick people is practically zero, which is why the graph sags, and at the beginning of the week peaks appear - sick people from the past days are entered there.
>Also, the values are presented in terms of 100 thousand population of Minsk and Belarus, respectively, to clearly show the difference between official reports and internal data of officials. The population of the capital is 2 million people, the entire country is 9.35 million.
>Judging by these statistics, infections began to decline only in mid-June; after the 16th, their number dropped below a thousand per day. At the same time, the Ministry of Health never reported more than a thousand new infections throughout the country during the spring and summer.
>The second wave of the pandemic, judging by our data, began in September; by mid-October, in Minsk alone, doctors were registering more than a thousand cases daily, and a month later - more than two thousand. The Ministry of Health has never recognized such a high number of infections: according to the department, the most new cases were identified on December 11 - 1,975 people throughout Belarus.
>In November and December, more people died every day in Minsk than officially in the whole of Belarus
>The data we received from the registry office of the main department of justice of the Minsk City Executive Committee contains information on deaths registered in the capital from November 5 to December 29, 2020. For each person, the cause of death according to ICD-10 coding is indicated, as well as the organization that established this cause.
>In these two months, coronavirus was listed as the cause of death in 700 cases. Those who died from it accounted for 15% of all deaths during this time.
>The Ministry of Health does not publish data on coronavirus deaths in Minsk - only for the whole country. From publications on the department’s telegram channel, it follows that throughout Belarus during this period, only 415 people died from COVID-19 - that is, even less than the Minsk registry office officially registered during the same time.
>In December, according to registry office data, about 15 people with coronavirus were registered daily in Minsk as the cause of death. The Ministry of Health at this time spoke of 8-9 deaths per day throughout the country.
>Like the graph of reported coronavirus cases, this graph is also smoothed using a centered moving average. In 2020, the record for the number of deaths from coronavirus, judging by our data, occurred on December 17 - 27 people. According to the Ministry of Health, there were only nine deaths across the country that day.
>There may be even more deaths - Covid is not always listed as the cause of death
>An employee of one of the pathology bureaus in Belarus anonymously explained the death registration system to Mediazona: “Let’s say a person dies in a hospital. In this case, the doctor makes a final diagnosis, which indicates the main, background and concomitant diseases, as well as complications.” All diseases are coded according to ICD-10. Doctors inform relatives about the death of the patient, and the body of the deceased is transported to the pathology bureau.
>An autopsy is performed there - if the decision on its necessity was made by the administration of the institution where the person was treated and died. After the autopsy, a pathological diagnosis is made, which will be recorded on the death certificate. If an autopsy is not performed, the attending physician makes a final diagnosis and issues a death certificate.
>After this, the relatives of the deceased are given a medical death certificate, with which they go to the district registry office, where this death is officially registered. From the city districts, all data is transferred to the registry office of the main department of justice of the Minsk City Executive Committee, where mortality statistics in the capital are compiled - this is exactly the data that Mediazona received from the source.
>If a person died at home, the police and local therapist are called. The police check that there are no violent injuries and leave. The local therapist looks at the card from the clinic: if the deceased recently visited a doctor and had an illness that could potentially lead to death, then it is indicated as the cause of death. In controversial cases, the body is sent for forensic examination.
>When coronavirus must be indicated as the cause of death, the Ministry of Health clarified in an order dated April 2, 2020. It states that the disease caused by COVID-19 (for example, viral pneumonia) is placed in the pathological diagnosis as the main one “in the presence of severe interstitial viral pneumonia with characteristic morphological signs.”
>If the deceased had other serious illnesses that received complications due to coronavirus, then COVID-19 may be part of a combined underlying disease - and in this case, the order states, it is the coronavirus that should be coded on the medical death certificate as the underlying disease.
>According to the same pathologist, the registry office data includes the underlying disease, and in both cases, from the order of the Ministry of Health, COVID-19 will be indicated as the cause of death. Accordingly, in our mortality data for November-December, 700 deaths are only those for whom coronavirus was indicated as the main disease.
>The interlocutor notes that if all doctors followed this order of the Ministry of Health, “we would have the most honest statistics in the world.” Falsifications, in his opinion, occur according to oral orders from the management of healthcare institutions and are “formed from below.”
>According to him, in order “not to spoil the statistics,” the pathologist can simply indicate the coronavirus in another paragraph of the certificate. If, in addition to COVID-19, a person had another serious illness, the expert can simply indicate Covid as the second main disease (and only the first one is included in the statistics).
>Among such diseases, behind which the coronavirus is often hidden in statistics, the doctor names heart disease - this is, for example, atherosclerotic or post-infarction cardiosclerosis, as well as arterial hypertension.
>“It’s very good to hide anything behind atherosclerosis, because most of those dying from coronavirus are over 50 years old. By the age of 50, every third person will have some manifestations of atherosclerosis,” says the interlocutor. Therefore, behind this cause of death there are many diseases, not just COVID-19, he notes.
>According to the registry office, 1,549 people died from types of atherosclerotic heart disease - this is 32.8% of those who died in November-December. It is difficult to say how many of these deaths may be related to the coronavirus, notes an employee of the pathology bureau, because “a fairly large percentage of controversial cases fall into this category when it is difficult to establish the exact cause of death.”
>According to him, old age as the cause of death (if an autopsy was not performed) can be indicated if the person was over 85 years old. According to Minsk registry offices, there were 123 such cases in November-December, and 29 of the deaths were slightly younger than this age.
>Without a positive test for coronavirus, it will never be indicated as the cause of death, the source adds, “even if everything is obvious to the pathologist at the autopsy.” And the result of a post-mortem examination is not always informative, and it is often received with a long delay, especially in the regions. In Minsk in 2020, 29% more people died than the five-year average
>With statistics on coronavirus infections and deaths unreliable, excess mortality data—a number that shows how many more people died in a year than the average over the past five years—helps estimate the scale of the epidemic.
>Typically, the number of deaths in Minsk is published by Belstat every quarter; the average number for 2014-2019 is about 17.4 thousand deaths per year.
>From the registry office data obtained by Mediazona, it follows that in 2020, 22,454 people died in Minsk - 5 thousand more than usual. That is, during the year of the epidemic, mortality increased by 29% - almost by a third.
>The quarterly data shows that the COVID-19 epidemic reached its peak during the second wave in the fall—the increase in mortality in the fourth quarter was more than 59%.
>The main victims of the epidemic are people over 60 years of age
>81% of deaths in Minsk in 2020 were people over 60 years of age. The largest increase in mortality occurred among such elderly people - instead of the usual 13,827, 18,191 deaths were registered in Minsk. The increase in mortality for those killed aged 60-69 years was 30.45%, for those over 70 years old - 27.7%.
>In November-December, at the height of the second wave of the Covid epidemic, the share of people over 70 years old among those who died from coronavirus was 56.3% (if you add them to those who died in the range from 60 to 69 years old, you get 81.6% of deaths from COVID-19).
>The average life expectancy in Belarus is 78 years for women and only 64 years for men. In all age groups, men die 2-3 times more often, with the exception of people over 70 - there are many more women here.
>A more complete picture of excess mortality in all of Belarus, and not just in Minsk, could be provided by Belstat data - but the agency has already postponed the publication date of these statistics for 2020 several times without explanation: at first it was about the beginning of April, then the agency planned to publish the data on April 16, the next date is set for May 17. But it’s not a fact that she won’t survive either.
>But the data already available to us on deaths in Minsk allows us to say that Belarus is faced with an unprecedented increase in mortality, and the official figures from the Ministry of Health do not reflect reality and are refuted by documents from registry offices and health care institutions.
End of quoting.
Funny how the country with the least restrictions also ends up with the smallest death percentage
This is a gross misrepresentation of the facts. Tens of thousands of Belarusians died over the course of the pandemic, that much has been revealed through the analysis of excess deaths, internet searches for coffins and funeral services, alongside reports from several sources of swamped hospitals incongruent with the national government's portrayal of everything being completely fine. Several reports suggested that the national government was not accurately counting deaths.
We don't know exactly how many Belarusians died, but we can deduce that's in the tens of thousands.
This should have aroused skepticism in you. How could a country that didn't take COVID seriously at all ever hope to have accurate statistics to provide? The answer is that it probably couldn't, which should prompt further examination. But, you didn't bother to do this, because what the Belarusian government said appealed to your desired narrative.
It's deeply ironic for you to cite an openly authoritarian government which suppresses information as a sort of ray of hope in a sea of darkness. The simplest explanation for their stats being incongruent with those of everyone else's, is that their openly authoritarian, oppressive regime decided to ignore the pandemic and under-report the severity of the disease.
It's doubtful that this could simply be a conspiracy by Western liberals to demonize Belarus, as Russia, another boogeyman of the Western liberals, did not receive this sort of flak in the media. It was because Russia didn't pretend that COVID didn't exist and try to cover up its existence. They took actual measures against COVID. In spite of similarities in the governments of Russia and Belarus, Russia responded far more substantively than Belarus did. Of course if you look, you will find criticism of Russia's response to COVID, but it's not on the same level as Belarus.
Unlike your hypothesis of the rest of the world having done this, which has virtually no evidence, this hypothesis actually does have quite a bit of evidence.
Are hospitals overcrowded with dying patients?
That's literally fake news - journalists went to those hospitals, and saw no one there
First off, a random conspiracy theorist on the web is not a journalist.
Generally speaking, the sick people are in a specific area of the hospital out of the access of regular people because real life isn't a pandemic movie where there's a bunch of dying people lying on the floor all around the hospital.
Also, it could be in some instances that the hospitals local to the "journalists" were not busy. Their anecdotal reports do not translate into conclusive, wide-sweeping data.
"But they only treated a handful of patients"
This is one regional hospital in a part of Britain, it doesn't speak for anything other than that region, so you're out of order to be using this as sweeping evidence. What does it mean to treat them? They don't specify. If we assume it is hospitalizing and caring for sick people, then sure, it is not many people.
Either way, it's not like hospitals being overcrowded has never happened before regardless of COVID-19. It even seems that the hospitals are overloaded every year, so corona did nothing special as usual
It is unusual because these overcrowdings were due to a pandemic that was killing people.
This doesn't come close to meeting the burden of proof required to refute all of the testimony suggesting hospitals to be overcrowded.
COVID was created in a laboratory
Now let's check out the evidence for the lab leak theory:
- US government paid the Wuhan lab to study bat coronaviruses. And so, we have a possible place where the virus could have been created.
- A natural origin for the virus still hasn't been found after 2 and a half years. The suggested pangolins have been ruled out.
- The furin cleavage site of COVID-19 contains a very rare arrangement of genes (1 in 36 chance) - and exactly the same one that is used in gain-of-function research.
- In late February 2022 it has been discovered that the furin cleavage site contains a sequence that is also found in a Moderna patent from a few years back - with a 1 in 3 trillion chance to arise naturally. The furin cleavage site is what allows the virus to infect people. This is the biggest change (in terms of the amount of bases) compared to other coronaviruses.
The claims made here suggesting it to be artificial are misleading, and fail to establish an artificial origin. This alone does not then prove that it did not originate from a laboratory, but it makes it irrational to insist for this to be the preferred explanation, let alone the only explanation.
Latching on to scientists doing their job by ruling out potential sources of origin, like pangolins, is nothing new for conspiracists, and demonstrates how they cannot seem to argue in good faith. One's perception of the significance of pangolins is dictated by the media's reporting of their significance, and is not objectively indicative of conspiracy.
The claims of artificial creation have been widely refuted. I will present this refutation across several articles, and summarize their arguments. The first article is from biospace.[197]
>The sequence Moderna patented is part of a gene known as MSHE and is involved in how damaged cells repair themselves. It is a possible target for cancer therapies. Twelve of the 19 amino acids are in SARS-CoV-2’s furin cleavage site, with the remaining seven matching nucleotides in a part of the genome nearby. The researchers suggest that this matching code may have become part of the COVID-19 genome by way of infected human cells expressing the MSH3 gene
>Lawrence Young, Ph.D., a virologist at the University of Warwick, said it was interesting but probably not significant enough to suggest the virus was manipulated in a laboratory. “We’re talking about a very, very, very small piece made up of 19 nucleotides. So it doesn’t mean very much to be frank, if you do these types of searches you can always find matches. Sometimes these things happen fortuitously, sometimes it’s the result of convergent evolution (when organisms evolve independently to have similar traits to adapt to their environment). It’s a quirky observation but I wouldn’t call it a smoking gun because it’s too small. It doesn’t get us any further with the debate about whether COVID was engineered.”
>Simon Clarke, Ph.D., a microbiologist at Reading University, also questioned the one-in-three trillion statistics, saying, “There can only be a certain number of [genetic combinations within] furin cleavage sites. They function like a lock and key in the cell, and the two only fit together in a limited number of combinations. So it’s an interesting coincidence but this is surely entirely coincidental.”
The second comes from healthfeedback.org.[198]
>Moderna’s patent US 9587003, which was filed in 2017, can be found here, and the complete sequence of the modified gene, given the number 11652, is shown here on GenBank, a database of nucleic acid sequences maintained by the U.S. National Center for Biotechnology Information (NCBI). According to the study, the modified gene is based on a human gene named MSH3, which is involved in DNA repair. This is unsurprising, as the title of Moderna’s patent signaled that they intended to use the modified gene sequences in cancer research.
>The sequence identified in the study, CTCCTCGGCGGGCACGTAG, is 19 nucleotides long. Nucleotides are the building blocks of nucleic acids like DNA and RNA. The authors stated that they didn’t find this sequence in any eukaryotic or viral genomes, except SARS-CoV-2.
>What made it appear more intriguing to the authors was the fact that the sequence occurred in the part of the spike protein known as the furin cleavage site (FCS), a short sequence of amino acids that can improve the virus’ infectivity of human cells. The presence of an FCS is not unique to SARS-CoV-2; other coronaviruses found in the wild[2], including MERS-CoV, also possess an FCS. The particular FCS in SARS-CoV-2 comprises a short sequence of amino acids in this order (table of amino acid abbreviations): PRRARSV (see Figure 1).
>Overall, the claim seems to be founded on the belief that because the sequence in the spike protein of SARS-CoV-2 was identical to a manmade gene sequence, the sequence couldn’t have occurred by chance, and must therefore have been designed.
>However, as scientists showed using the same search tools as the authors, this 19-nucleotide long sequence occurs naturally in other living things. For example, the sequence is present in eukaryotes, like a species of birds, contrary to the authors’ statement that it cannot be found in eukaryotes. This raises the question of whether the authors simply failed to check for matches to other organisms. https://t.co/SMJ5XvDLgM
>It is also present in a bacterium, although bacteria aren’t eukaryotes: https://t.co/rkUtL3OLAo
>In short, the 19-nucleotide sequence isn’t unique to the modified MSH3 gene patented by Moderna and isn’t uniquely manmade, as it can occur in nature.
>Using the NCBI’s BLAST tool, we can also find genes from other organisms that are highly similar to the modified MSH3 gene patented by Moderna, such as the chinchilla
>In summary, the assumption that the most likely explanation for the FCS in SARS-CoV-2 is that it was derived from the modified MSH3 gene isn’t supported by the evidence, given that this particular sequence already occurs in many different living things naturally.
>In addition, the 19-nucleotide sequence doesn’t produce amino acids corresponding to an FCS in the context of the modified MSH3 DNA, as pointed out by bioinformatician Moreno Colaiacovo.
The third is in a twitter thread from a scientist.[199]
>Moreover, if we translate the sequence using a tool like ExPASy translate, we notice that the short sequence does not encode for PRRAR in this protein, but rather YVPAE (which is not a furin cleavage site). The translation is from 5' to 3' in frame 1. 5/ pic.twitter.com/ARqQmIY0Yj
>This is because the 19-nucleotide sequence is present on the reverse complement strand of the DNA. Double-stranded DNA comprises two strands of DNA, which are complementary to each other and run in opposite directions (see Figure 3 below). The two ends of the strand are labeled 5’ and 3’. The production of protein from mRNA, which codes for the instructions from DNA, is based on the sequence of the sense strand (the strand running from 5’ to 3’), not the reverse complement (antisense) strand (3’ to 5’ strand). This is why the 19-nucleotide sequence, which is on the reverse complement strand, isn’t relevant to protein production and doesn’t lead to a furin cleavage site.
>This isn’t the first time that a very brief nucleic acid sequence in SARS-CoV-2, which happened to be identical to already-known genetic sequences, was used to support claims that the virus was engineered in the laboratory. In 2020, a similar false claim that SARS-CoV-2 contained sequences from the human immunodeficiency virus was also made on the same spurious basis. Scientists cautioned that such short, identical sequences are commonly shared by many living things, and on their own don’t provide evidence of lab engineering.
The fourth, another article from healthfeedback.org.[200]
>The evidence available so far hasn’t shown signs that the virus was engineered[3]. For starters, there isn’t a known coronavirus that is genetically similar enough to SARS-CoV-2 to be a plausible candidate for genetic modification. The closest known relative to SARS-CoV-2, a bat coronavirus named RaTG13, is 96% identical to SARS-CoV-2[4]. But in evolutionary terms, even this level of similarity would still require RaTG13 to undergo decades of evolution in order to produce SARS-CoV-2. In addition, there are also numerous technical obstacles that would have to be involved in an attempt at genetic modification
The fifth, another article from healthfeedback.[201]
>As Stanley Perlman, a professor of microbiology at the University of Iowa, said, “it would not be known in advance what sequence should be used to replace the RaTG13 Spike protein.” Susan Weiss, a professor of microbiology at the University of Pennsylvania countered the hypothesis with the question: “Where would they get the RBD from to insert into RaTG13?”
>After the SARS outbreak in 2003, which was caused by another coronavirus, SARS-CoV-1, researchers identified a set of key amino acids within the Spike RBD important for SARS-CoV-1 infectiousness[9,10]. To improve the infectiousness of a coronavirus, the best engineering strategy would have been to use the amino acid sequences discovered in SARS-CoV-1, as these are known to be efficient and can then be refined to produce an even better molecular design for SARS-CoV-2.
>Surprisingly, the current SARS-CoV-2 Spike RBD doesn’t contain this optimal set of amino acids recognized in SARS-CoV-1[1], yet it is nonetheless able to bind to its target human cells with an affinity even higher than SARS-CoV-1[11,12]. This finding undermines the claim that SARS-CoV-2 is the result of modifying RaTG13 to give it an enhanced Spike RBD.
>David Robertson, Professor, University of Glasgow:
>Q: Is it likely that SARS-CoV-2 is derived from RaTG13 by artificially replacing the Spike RBD?
>A: No, the replacement of RaTG13’s RBD with SARS-CoV-2’s RBD would still be a relatively divergent virus from SARS-CoV-2. This is because there are other mutations in RaTG13’s genome that make it distinct from SARS-CoV-2. This was quantified here by Wang et al.[8]. You’d have to change these other parts of RaTG13’s genome to arrive at SARS-CoV-2’s sequence.
>Q: Is it likely that SARS-CoV-2 is the result of gain-of-function experiments?
>A: It’s extremely unlikely SARS-CoV-2 was generated by gain-of-function experiments. We didn’t know anything about this new coronavirus before it emerged in 2019 so how could it have been designed? What would have been the template for this? It’s just incredibly implausible that some random experiments could have generated a virus with such dramatic properties but so unlike anything we’d observed before.
>Moreover all of the properties of SARS-CoV-2 can be explained by natural processes such as a mutation and recombination that are well documented in coronaviruses. We discussed the probable source of the SARS-CoV-2 progenitor here in a study by Lytras et al.[2].
>Susan Weiss, Professor, University of Pennsylvania:
>Q: Is it likely that SARS-CoV-2 is derived from RaTG13 by artificially replacing the Spike RBD?
>A: NO. The RBD is not the only difference between the two genomes. They would have to make many other changes. Where would they get the RBD from to insert into RaTG13? Why would they suppose that changing the RBD of some random bat virus would produce a virus lethal for humans? These viruses are naturally selected to do what they do—just as variants now are selected to optimize stability and spread.
>Robert Garry, Professor, University of Tulane:
>RatG13 could not have served as the backbone of SARS-CoV-2. While 96% sounds close, in evolutionary terms, it is quite distant, and it would take decades of evolution for the genome of RaTG13 to resemble that of SARS-CoV-2. The difference is about 1,200 bases or 400 amino acids. Gain-of-function research cannot close that gap. Passage in cell culture or transgenic animals would never create the changes. Replacing the RaTG13 RBD with the RBD of another virus (such as the pangolin coronavirus) certainly would not close the gap. It still leaves you with a virus that is still 96% different from SARS-CoV-2. It is highly unlikely, in fact,near impossible—that SARS-CoV-2 is the result of gain-of-function research. This would require a virus much closer than RaTG13, at least 99% similar or more likely 99.9% similar.
>Stanley Perlman, Professor, University of Iowa:
>Q: Is it likely that SARS-CoV-2 is derived from RaTG13 by artificially replacing the Spike RBD?
>A: RaTG13 is 4% different from SARS-CoV-2. This is equivalent to 1,200 nucleotides.
>I do not know what fraction of the differences between SARS-CoV-2 and RaTG13 are in the S protein; there are certainly some outside of the [Spike RBD] protein.
>In addition, it would not be known in advance what sequence should be used to replace the RaTG13 S protein. Finally, the whole process of reverse genetics for coronaviruses is difficult, even for experts. So my answer is that it is very unlikely (impossible) for this scenario to be the explanation. It is much more likely that nature did this.
>Q: Is it likely that SARS-CoV-2 is the result of gain-of-function experiments?
>A: This possibility implies that a virus was already in hand that was known to infect human cells. There is no evidence for this. Even if this putative virus existed, it would not be known in advance how to modify it to enhance transmission and virulence. Passage through tissue culture cells generally results in virus attenuation. In fact, that is how the poliovirus vaccine was developed from wild type polio.
The supposed genetic similarities are nothing damning. The genetic sequence isn't unique at all and has been found in other organisms. The genetic sequences don't lead to a furin cleavage site either. Beyond this, you've presented no other evidence of this being a bioweapon other than the U.S. Government funding a Chinese lab (they do this all around the world), and a biolab being in proximity to the origin of outbreak. That region was a favorable location for a biolab in the first place, with all of the bats and diseases around there, so I don't think it's a crazy coincidence.
It is highly implausible that COVID was a bioweapon. There was no other virus like it prior to the pandemic, which raises the question of where it came from if it was a bioweapon. It was significantly different from every other virus in ways that a lab of that caliber would probably not have been capable of engineering in the span of five years, according to the scientists interviewed in the above articles.
Then was the issue of how the scientists could have coerced the virus to develop a trait that would enhance infectivity, without knowing that the genetic trait would enhance infectivity. Evolution is a mindless process, which does not consciously work towards any particular objective. They would likely have had to perform experimentation on living organisms in order to know it would enhance infectivity. They would probably have to experiment on humans. There are many questions as to how they could have genetically modified it in ways to enhance infectivity. They probably would have necessitated animal and or human experimentation and all sorts of stuff that would leave lots of witnesses and evidence behind, of which nothing has come to light.
There wasn't a 1 in 3 trillion chance of the sequence occurring naturally, this was the conjecture of the authors of that particular paper. That number by itself doesn't even mean anything. 1 in 3 trillion out of what? The sequence was subsequently found in several other organisms.
$3.7mil was given to the Wuhan lab over the course of 5 years, beginning around 2014, ending around 2019. These grants were approved yearly under Obama and Trump. What this means is that the conspiracy must have been in motion under both presidents. It also means this amount of money must suffice to develop such a bioweapon. And, it also means this must have been enough time to develop a bioweapon that genetically distinct from all other pathogens, seeing as the closest relative is RaTG13, which is 96% similar — the 4% difference by all accounts likely amounting to far more than 5 years of evolution. The implausibility of the conspiracy is growing.
In 2018 and 2019 the NIH provided approximately $2.5 million in additional funding to various organizations in China, Wuhan University included. In 2007, while George W. Bush was president, the NIH provided more than $2 million to various research centers across China, though this doesn't mean anything reached the Wuhan lab. Was Bush also involved?[202]
If we asssume that this specific lab got all of the money, which it didn't, that is still only $8.2 million.
It's hard to estimate how much money it would cost governments to manufacture a single bioweapon, but going off of the budgets of bioweapons programs that the public is aware of, their programs tend to be in the range of hundreds of millions, to billions. The United States government for instance spent over $400 million on its bioweapons program, most of which was for research and development. Bear in mind, they weren't (as far as we know) engineering some pathogens to be so distinct as to be unrecognizable. Comparatively, the work they were doing was more rudimentary, and yet they spent incredible amounts of money.[203]
>From the onset of the U.S. biological weapons program in 1943 through the end of World War II the United States spent $400 million on biological weapons, mostly on research and development.[33] The budget for fiscal year 1966 was $38 million.[34] When Nixon ended the program the budget was $300 million annually
Basically every country that has run a serious bioweapons program has had to spend at least several hundred million. And these people weren't developing things as complicated as COVID.
Now, the high overall costs can be explained by the fact that they were working on numerous projects under one program, but individual projects still usually cost tens of millions.
America gives money to all sorts of missions around the world, so mere funding is not inherently suspicious. When combined with other evidence, it may be, but what other evidence is there to compound the lab leak hypothesis?
So, the virus was indeed created in a lab. There is no other way to explain all of the above.
There are other explanations. Natural selection can explain what you've cited. The lab-leak hypothesis does not hold up. Also, just for a second consider the absurdity of the situation. Why would Moderna use a publicly patented genetic sequence in a bioweapon, discoverable to literally any scientists with specialized search tools? This is almost on par with the absurdity of supposed Moon-hoax blunders, like forgetting tire tracks or stars.
A conspiracy carried out under two — maybe even three — presidencies, in collaboration with the Chinese government and Moderna. That has to involve quite a lot of people. So far there's been no leaks from the supposed conspirators.
Low vaccinated countries did not get ravaged by COVID
For example, Senegal - where only 6% of people took a COVID vaccine - had a COVID death rate of 12.1 people per 100000 (or 0.0121%). Nigeria with 10% jab rate had an even lesser death rate - just 0.0016%. Cameroon - 4% vaccination rate, 0.0075% COVID deaths. Algeria - 15% / 0.016%. Syria - 10% / 0.0185%. Chad - 12% / 0.0012%. You can pretty much pick any of the really low vaccinated countries and find a low COVID death rate, too. On the other hand, the country with the highest COVID death rate (Peru at 0.657%) had 83% of its inhabitants take the shot. Why did the jabs not save it? Why are really highly vaccinated European countries (such as Italy or Spain) rotting with COVID death rates of 0.2796% and 0.2296% (over 10 times higher than the low vaccinated ones)? Hungary - the fourth highest country in terms of COVID deaths - had 64% of its inhabitants take the shot; and yet that didn't save them. Looking further down, Serbia or Ukraine have twice less deaths with much lower jab rates
Senegal is also a third world nation. So are all the other countries. Poor, impoverished, and developing nations have worse reporting systems. This should be obvious. Another thing to note is that in some of these Western African countries, when people die, they are often buried the same day without much of an official processing of their death.
Notice how even Eastern Europe is lower than Western Europe but above other poorer countries around Africa and the Middle East? Their systems are also not necessarily as great as Western Europe's, as they tend to be poorer and their governments less efficient. Not to mention the differences in how most third world countries are structured as opposed to European ones. Rural as opposed to highly urbanized. There are various factors that make it so poorer countries will have lower reports, but it generally comes down to less efficient medical systems.
This is only evidence of African countries being unable to properly track COVID deaths. Maybe they had lower rates of death though.
Analyzing VAERS
The COVID vaccines are over ten times more likely to cause side effects than all the other vaccines from previous years put together. More than 90% of COVID vaccines used in the US are Pfizer and Moderna - both using the newly developed mRNA technology - so they are the ones mostly responsible for the increased side effects. For the 2018-19 season (before corona) I'm taking into account flu vaccine doses ONLY - because I wasn't able to find the data for any others. If I did, it would increase the taken doses, decrease the percentage of side effects (since the amount of VAERS reports is already determined), and tip the scale against the COVID vaccines even more. Fact checkers ... try to deny the results of VAERS by saying that anyone can submit a report and that they "just show signals", etc. UPDATE June 2023: I still see shills on Twitter making this non-argument, so let me give a more thorough reply. Do you really think that, since the introduction of COVID vaccines, there suddenly became ten times (or more) the amount of trolls willing to submit fake VAERS reports? Look at the VAERS submission form for yourself and see how much data is required; it probably takes an hour or so to fill. There might be a few people willing to do that for the lulz, but there are much much more effective ways to troll; so this surely doesn't explain the millions of reports
>Warning: Knowingly filing a false VAERS report with the intent to mislead the Department of Health and Human Services is a violation of Federal law (18 U.S. Code § 1001) punishable by fine and imprisonment.
What are the chances that this law will be enforced? Jaywalking is illegal. But is it really? Where I live, it might as well be like crossing the sidewalk.
A doctor submitted a false report in 2018 saying he turned into the Incredible Hulk after getting a flu shot. Nothing happened to him. Funnily, VAERS needed HIS permission to remove his false claim from their database.[204]
Is the government, during a massive health crisis when all systems are swamped, going to investigate potentially "false" reports? Would the average person know filing a false report is a crime? What even would a false report consist of? People could mistakenly blame unrelated symptoms on the COVID vaccine in a report, thereby making a "false report", however, that isn't malicious falsity.
So again, there can't be that many trolls willing to push through regardless. But! Maybe these reports aren't trolling. Maybe people really believe they are having a vaccine reaction, but are simply mistaken? Even if the effect came a few days or hours following the vaccine? Still - even if all those people are simply wrong - it is then appropriate to ask from where such a massive increase of reports is coming from? We have removed trolling as a possibility, so what's causing a ten times (or probably more now) increase in reports right after the introduction of the COVID vaccines? What other thing happened at the same time? I don't see anything
Maybe it's articles like this? Maybe they aren't trolls but are just delusional people manipulated by stuff they've seen online? You don't see anything because you aren't removing yourself from your conspiracy bubble. How often do you think of conspiracies you believed in that turned out false? There was a massive influx of insane conspiracy theories relating to the vaccines before they even came out. You don't think that would've contributed to people's fears? It definitely contributed to mine.
The higher the amount of vaccines given in an USA state, the more injury reports. The states with the least vaccinated people have almost no reports. An almost perfect correlation.
How are you supposed to make a report based in delusion if you haven't received a vaccine? By falsely remembering you got the vaccine when you didn't? It isn't strange to me that reports would rise with vaccination. This may serve to suggest that delusional reports were more common than fraudulent reports, but that's all.
VAERS is not proof unto itself of the vaccines being objectively harmful. It is a system for people to report harmful effects from vaccines in case some issues arise that weren't discovered during clinical trials. These reports can be investigated. And they are investigated, sometimes resulting in changes to government policy, like with the Johnson & Johnson vaccine pause. People aren't and weren't dropping like flies from the vaccines.
It is individuals thinking they've been harmed by a vaccine, and people who know individuals who think they've been harmed, or people who think those individuals were harmed, making the reports, in addition to people making fraudulent reports. The system is not immune to false reporting. It's completely devoid of controls that would ensure false reports are not made. Anyone can send in a report.
Analyzing V-Safe
V-Safe is no more reliable than VAERS. Anyone can make a report. It suffers the same drawbacks.
Astonishing. One out of four people injected with these concoctions (both doses, as recommended by "the experts") will experience joint pain during 7 days after taking the vaccine. Almost half of the lab rats patients will have a headache, more than half fatigue. And 30% fever; what corona allegedly causes is also done by the vaccine
I don't know how you can write that with a straight face.
None of these side effects are severe. They're quite standard for vaccines. There's nothing serious that is widely reported like anaphylaxis or something awful.
It's hypocritical to attack health authorities for supposedly deeming a case to be COVID on the basis of one symptom while at the same time lambasting the vaccines as deadly snake venom because of people experiencing typical vaccine side effects.
What's worse: Soreness and redness of an injection site, or respiratory failure and death?
UPDATE November 2022: hey, no wonder they've decided to use scientists to gatekeep the actual V-Safe data. Because this recently dropped:This does not give any insight into the specific issues people faced and the long-term effects they suffered. It doesn't give any insight into the legitimacy of the claims either.
This data was produced during a lawsuit levied by ICAN, an anti-vaccine scam organization known for shaking down companies for money, and making crappy "documentaries" about the dangers of vaccines. While this doesn't completely render all of the information they put out false, I'd be a lot more skeptical of them, as they have a financial incentive to demonstrate harm from the vaccines and have a record of trying to do this. You are choosing to trust them over everyone else.
Considering that there isn't evidence of this many vaccine induced hospitalizations and medical emergencies elsewhere, I wouldn't buy into it. Not to say that what they've released is completely fraudulent and fabricated, they may simply be overstating their claims.
Extreme consequences of the COVID vaccines
These are extremely rare. This then becomes a matter of weighing the consequences individually and societally. Individually, you'll likely be harmed more by COVID than the vaccine. Societally, there will be much more harm caused by rampant infection than vaccination.
The vaccine destroys the female reproductive system
Yet vaccinated women are still getting pregnant and having babies. This section was just a waste of time, but I wanted to be thorough.
First of all, consider the fact that Pfizer has excluded pregnant women from their vaccine study:
Now why would they do that other than a suspicion that the vaccine is in fact harmful to pregnant women?
Probably because they didn't know how it may affect an unborn baby, so they made the responsible decision of excluding pregnant women. They're damned if they do, damned if they don't. To take precautions for pregnant women will spark fear, but to throw caution to the wind will incite outrage. It's deeply hypocritical to chastise them like this. You're grasping at straws at this point.
Yet that didn't stop the "fact checkers" and the governments from claiming that the vaccine is safe for pregnant women, despite having no specific tests.
I audibly sighed after reading this because of how stupid it is.
Look at the image you just displayed.[205] Note the date, "07October2020". When was the article you cited published? [206] "20 August 2021". Almost an entire year later. It literally says it in the damn URL, I saw the date when my cursor hovered over it. The evidence behind that claim arose within that ten month window.
Another reason to suspect the vaccine attacks the reproductive system is the fact the ovaries are a major mRNA accumulation point (in rats, since it wasn't tested in humans):
Rats aren't humans.
When the US government attempted to prove that the vaccines are safe for pregnant women, they had to resort to fraud. Look:
I've left the study cited by digdeeper here.[207] digdeeper cannot understand basic philosophy of science.
>V-safe pregnancy registry participants who received at least one dose of an mRNA COVID-19 vaccine preconception or prior to 20 weeks’ gestation and who did not report a pregnancy loss before 6 completed weeks’ gestation were included in this analysis to assess the cumulative risk of SAB using Life Table methods.
What this means is they've arbitrarily excluded the women who've had their miscarriages happen before week 6. Which just so happens to be the week when miscarriages stop happening:
The rate of miscarriages is 50-75% in week 3 and 4, 21% in week 5, 5% in week 6 and even less later. And the study only considered women who miscarried week 6 or later. So, the "researchers" eliminated the women who could actually get miscarriages
If miscarriages "stop happening" after week 6 (which is patently false, they're relatively common up to 10 weeks) as the numbers you yourself display show, then it makes sense to exclude women who've had them before week 6. It would be anomalous to see them after week 6, according to your logic. 10-20% of all pregnancies end in miscarriages. In the beginning weeks of pregnancy, they're highly common. It's also harder to track when exactly a miscarriage occurred that early in a pregnancy, a lot of early miscarriages are chemical.
You omitted important information from the study that you quoted, like this quote, which clarifies your confusion:
>The inclusion of participants pregnant at 6 completed weeks’ gestation reflects when pregnancies are generally recognized and is consistent with previous literature estimating SAB in the general population.5, 8–10, 15
4-6 weeks of gestation is when pregnancies are generally recognized, as the miscarriage rate has dropped significantly by that point, and is relatively stable.
It would be like, if I wanted to prove that people can't jump, I would only include the obese in my study, who actually can't jump. The honest way to do the study would be to include all the weeks - but they couldn't have done that because it would show that the vaccine DOES in fact induce miscarriages. An admitted fraud, right in the methods
This is your opinion stemming from not understanding how scientific studies are conducted, and not having a scientific mind. By excluding a group that often gets miscarriages, specifically miscarriages which can be hard to track accurately, you will discover anomalous miscarriages. It's a pretty basic concept.
Even if they did "arbitrarily" exclude women prior to 6 weeks, this still wouldn't prove that they were hiding miscarriages caused by the vaccines, you're assuming that they could be causing miscarriages because of a study about rats, and you're assuming their intentions behind excluding miscarriages before 6 weeks. Overall this is very flimsy argumentation, and doesn't come close to meeting any reasonable burden of proof, but that can be said for almost all of the arguments in this article.
The vaccine destroys the male reproductive system
Yet vaccinated men are still impregnating women. Billions of people injected, and yet birth rates haven't catastrophically tanked in the wake of the vaccine rollout.
Oh, by the way, we now have proof that the vaccine attacks the male reproductive system, too. "Repetitive measurements revealed −15.4% sperm concentration decrease on T2 (CI -25.5%–3.9%, p = 0.01) leading to total motile count 22.1% reduction (CI -35% - -6.6%, p = 0.007) compared to T0.". The people reporting the results have of course begun with the standard lip service for the vaccine: "The development of covid-19 vaccinations represents a notable scientific achievement". Hahaha. By the way, I've read the paper itself and (as usual) the abstract as well as the media reporting are fraudulent. The situation is much worse than it seems - look:
T3 are the results 150+ days after taking the shot, and they still show a "Total Motile Count" drop of 19.4%, and "Sperm concentration" drop of 15.9% compared to the baseline (before vaccination). Comparing T2 to T3 shows that the sperm concentration still keeps falling at month 6 after the shot - while the abstract claims that "T3 evaluation demonstrated overall recovery." of sperm functionality. Science is in on the fraud, my friends. The vast majority of people will only read the abstract, and trust the assurances of fact checkers - which repeat the same "recovery" lie - so the fraud works very well. Let me reiterate, the month 6 sperm functionality is lower than the month 3 one. This likely means that the damage is forever. After all, wouldn't the functionality have come back after five months if it was supposed to? A bone break heals long before that, for example. But the data shows the sperm parameters are still getting worse at that point.
Let's grapple with the evidence: [208]
>Covid-19 vaccination BNT162b2 temporarily impairs semen concentration and total motile count among semen donors
>To investigate the effect of covid-19 BNT162b2 (Pfizer) vaccine on semen parameters among semen donors (SD).
>37 SD from three sperm banks that provided 220 samples, were included in that retrospective longitudinal multicenter cohort study. BNT162b2 vaccination included two doses, and vaccination completion was scheduled 7 days after the second dose. The study included four phases: T0 – pre-vaccination baseline control, which encompassed 1–2 initial samples per SD; T1, T2 and T3 – short, intermediate, and long terms evaluations, respectively. Each included 1–3 semen samples per donor provided 15–45, 75-120, and over 150 days after vaccination completion, respectively. The primary endpoints were semen parameters. Three statistical analyses were conducted: 1) generalized estimated equation model; 2) first sample and 3) samples' mean of each donor per period were compared to T0.
>Repetitive measurements revealed −15.4% sperm concentration decrease on T2 (CI -25.5%–3.9%, p = 0.01) leading to total motile count 22.1% reduction (CI -35% - -6.6%, p = 0.007) compared to T0. Similarly, analysis of first semen sample only and samples' mean per donor resulted in concentration and TMC reductions on T2 compared to T0 - median decline of 12 million/ml and 31 million motile spermatozoa, respectively (p = 0.02 and 0.002 respectively) on first sample evaluation and median decline of 9.5×106 and 27.3 million motile spermatozoa (p = 0.004 and 0.003, respectively) on samples' mean examination. T3 evaluation demonstrated overall recovery. Semen volume and sperm motility were not impaired.
>This longitudinal study focused on SD demonstrates selective temporary sperm concentration and TMC deterioration three months after vaccination followed by later recovery verified by diverse statistical analyses.
Here's the issue with your interpretation of this study: Under sperm concentration and sperm motility we see that the results are worse in T3 than T2, suggesting that the sperm quality has been getting worse with time. The problem here is that sperm concentration has a p value of .044, and sperm motility has a p value of .058. According to statistical analysis, low p values, those being under .05, suggest statistical significance. Those greater than .05 indicate there's insufficient evidence for statistical significance. Statistical significance indicates the veracity of the hypothesis.
The results showing improvement have lower p values than the ones showing the opposite, meaning they have greater veracity. Sperm motility is, as I said, .058, which is not statistically significant i.e null, meaning it doesn't prove that the sperm are worsening. Sperm concentration is not entirely null, but it is barely escaping from being null, and has poor confidence intervals.
With the confidence intervals, if the percentage you see becomes greater than 0%, that means you can't reject the null hypothesis of no change. The confidence intervals affirm that the sperm quality worsened, then improved, but they don't affirm that they worsened, and continued to worsen. The confidence intervals for results showing no improvement are also low, as you can see.
The reason the authors said that the subjects improved was due to the results saying otherwise not being statistically significant.
The fact that you've cut the p values from your screenshot suggests that you're unaware of their significance. This is an egregious error, p values and confidence intervals are essential to determining the veracity of data.
Something else to note is that this is just one study, only examining 37 males.
This article digdeeper cites and raves about in conspiratorial fashion is quite reasonable. The people they interview question the statistical significance, call for more research, and postulate other factors that could've contributed to the results e.g stress, seasonal changes.[209]
The article also mentions this study: [210]
>Methods
>This was a prospective cohort study conducted on sperm donors at the sperm bank of a tertiary, university affiliated medical center. All sperm donors donated sperm repeatedly and the average sperm parameters of all available samples were compared before and after receiving the SARS‐CoV‐2 vaccine. Each donor served as his own control. For all participants, at‐least one sperm sample was received 72 days after completing the second vaccine. Main outcome measures included total sperm count, total motile count and percent of motile sperm.
>Results
>A total of 898 sperm samples from 33 sperm donors that were vaccinated with the Pfizer BNT162b, mRNA, SARS‐CoV‐2 virus vaccine were analyzed, 425 samples were received before the vaccine, while 473 samples were received after vaccination. Total sperm count and total motile count increased after the second vaccine compared to samples before vaccination. Percent of motile sperm did not change after vaccine.
>Conclusion
>The Pfizer BNT162b, SARS‐CoV‐2 vaccine has no deleterious effect on sperm quality. Patients and physicians should be counseled accordingly.
Unlike with your study, the results demonstrating improvement are statistically significant. It's of a comparable size to your study.
With that being said, let's see other research.
Here's a systematic literature review: [211]
>Safrai et al [55] published the first study on the impact of the COVID-19 vaccine on sperm parameters, demonstrating that the BNT162b2 mRNA vaccine (Pfizer or BioNTech) was not associated with a decrease in sperm quality. The study enrolled 72 individuals (57 of whom had normal sperm parameters). Sperm parameters in men with normal and abnormal sperm analysis did not change significantly after vaccination. The authors noted that after COVID-19 vaccination, none of the sperm parameters changed significantly [55]. In February and March 2021, Lifshitz et al [54] evaluated the effects of the Pfizer COVID-19 vaccine in 75 men with proven fertility [54]. The primary outcome was the percentage of abnormal sperm parameters in men 1 to 2 months after the second injection of the COVID-19 vaccine, including abnormal sperm morphology, reduced percentage of motile spermatozoa, and oligozoospermia rates. The results showed that the semen parameters after COVID-19 vaccination were mostly within the normal reference ranges established by the World Health Organization and did not indicate any causative negative effects of the COVID-19 vaccination. However, the participants in this study were a relatively homogeneous group, consisting of fertile male individuals from high socioeconomic groups. Moreover, participants were only followed up for 1 to 2 months after receiving the second dose of vaccine; therefore, long-term results have not yet been reported. In contrast, in a retrospective, longitudinal, multicenter study recently published in Andrology, the effects of the COVID-19 BNT162b2 vaccine on semen parameters were evaluated in 37 semen donors at different time points, before and after immunization [53]. Compared with the prevaccination levels, there was a selective decrease in sperm concentration and TMSC 75 to 125 days after vaccination (P=.01 and P=.007, respectively). Normal levels of these parameters were restored 145 days after vaccination, and no changes in sperm volume or motility were observed. Similarly, Abd et al [51] observed that the total motility and progressive sperm activity decreased significantly after BNT162b2 injection. Notably, considering that all semen parameters were still within the normal range, the investigator considered that the vaccine had no deleterious effects on semen parameters [51].
>Surprisingly, significant improvements in some sperm parameters were noted after the COVID-19 vaccination. Massarotti et al [38] conducted a prospective study in which 101 vaccinated men (who were undergoing fertility treatments) had semen testing before vaccination and 2.3 (SD 1.5) months after the second dose of vaccine (76% of the participants were vaccinated with mRNA vaccine and 20% with viral-vectored vaccine). The investigators found a significant reduction in the median volume of the sample (from 3.0 to 2.6 mL), whereas sperm concentration, progressive motility, and TMSC increased (from 25.0 to 43.0 million/mL, from 50% to 56%, and from 34.8 to 54.6 million, respectively) [38]. In another prospective cohort study published in JAMA, Gonzalez et al [35] evaluated the effect of mRNA vaccines in 45 healthy volunteers (21 Pfizer and 24 Moderna) and found no significant decrease in sperm parameters. Semen samples were collected before the first dose and a median of 75 days after the second dose [35]. The baseline median sperm concentration was 26 million/mL, and the TMSC was 36 million. After the second vaccine dose, the median sperm concentration increased to 30 million/mL, and the median TMSC concentration increased to 44 million. Sperm motility and semen volume also increased significantly. The authors suggested that the increase in sperm parameters might be explained by known individual variations in sperm and increased abstinence time before postvaccine sample collection. Similarly, Barda et al [56] evaluated the effect of 2 doses of the vaccine (BNT162b2) on the sperm parameters of 33 sperm donors who donated sperm on multiple occasions. Compared with the percentage of motile sperm in the sample before vaccination, the percentage after the second dose of the vaccine did not change. However, the total sperm and motile counts increased unexpectedly.[56]. One possible explanation is that some participants changed their lifestyle habits or were more health conscious than the retrospectively enrolled infertile population, which acted as a confounding factor and positively affected sperm quality [58].
>Two previous meta-analyses examined the effect of COVID-19 vaccination on sperm parameters based on published data [59,60]. Both studies suggested that the vaccination had no discernible negative impact on sperm quality. However, the 2 meta-analyses had nonnegligible limitations: the included studies used different types of vaccines, administered different doses of vaccines, had mostly unknown time intervals from vaccination to sperm analysis, had large differences in the participating populations, and had a small sample size for each group after the subgroup analysis. In other words, the methodological quality of meta-analyses assessing the impact of COVID-19 vaccination on semen parameters is currently unsatisfactory. As new controlled trials and prospective cohort studies with larger sample sizes emerge, the possibility of a negative effect of the COVID-19 vaccine on sperm quality must be further clarified.
>According to a study by Gat et al [53], the systemic immune response following BNT162b2 immunization may contribute to the deterioration of selective temporary sperm concentration and TMSC; however, the long-term prognosis remains favorable [53]. It is important to note that similar studies did not have data on the detailed health and immune status of the participants before vaccination. Therefore, their conclusions should be interpreted with caution. Carto et al [65] examined data from a large US electronic health record database on the risk of orchitis, epididymitis, or both in men vaccinated against COVID-19 [65]. They discovered that the serum levels of antisperm antibodies and antiphospholipid antibodies against cardiolipin, phosphatidylserine, annexin V, and 2-glycoprotein-1 did not differ significantly before and after vaccination. Furthermore, the levels of these autoimmune antibodies did not correlate with the sperm parameters. Their findings even suggested that COVID-19 vaccination was linked to a lower risk of orchitis, epididymitis, or both (odds ratio 0.568, 95% CI 0.497-0.649).
>In addition, BNT162b2 and mRNA-1273 are lipid nanoparticle-formulated vaccines against SARS-CoV-2. These excipients, adjuvants, or both may act as vehicles for therapeutic content delivery while also increasing the intensity of the immune response [22]. Several studies have shown that these nanoparticles can cross biological barriers and can be deposited in reproductive organs, such as the testes, impairing sperm quality by increasing inflammation, damaging DNA structure, decreasing mitochondrial function, and inducing apoptosis [66]. Therefore, some researchers are concerned that vaccine excipients, adjuvants, or both may induce testicular damage. However, Olana et al [36] found no significant differences in the levels of reactive oxygen metabolites, electrolytes, or interleukin-6 in the seminal plasma of participants before and after the BNT162b2 vaccination [36]. Indeed, the current basic research evidence and clinical data supporting the idea that a systemic immune response after COVID-19 vaccination can lead to impaired sperm quality are insufficient.
>Although semen analysis serves as the foundation for evaluating male fertility, it should be noted that it is an imperfect predictor of fertility potential. Further persuasive evidence comes from ART and artificial insemination by partner outcomes in couples after receiving the COVID-19 vaccine [57,67]. In a prospective cohort study involving 735 infertile couples, Dong et al [47] demonstrated that the quality of the embryos and the pregnancy rate in IVF treatment were unaffected by the couples’ vaccination status or vaccine type. Similarly, no differences in fertility or pregnancy outcomes were observed in the study by Orvieto et al [57]. In another multicenter prospective study of 4185 couples, Wang et al [68] found no association between COVID-19 vaccination status (eg, inactivated, adenoviral, and recombinant vaccines) and pregnancy rates in artificial insemination by partner treatment [68].
>Conclusions
>In summary, the data in this review show that the COVID-19 vaccine is safe for male reproductive health. Serious side effects of the COVID-19 vaccine are extremely rare, and men experience few problems with sperm parameters or reproductive potential after vaccination. Considering that SARS-CoV-2 infection itself may be associated with impaired fertility, vaccination could serve as a potential tool to preserve male fertility by preventing COVID-19. Therefore, vaccination should be clearly recommended for all men wishing to have children unless there are additional contraindications.
There's more evidence suggesting harm and recovery than permanent damage. Vaccination status did not impact fertility in studies of artificial insemination and IVF. If the vaccines lowered fertility, then there should have been diminished fertility in those studies.
It seems the authors of this study did another study on men and women.[212]
>Effects of COVID-19 vaccination on human fertility: a post-pandemic literature review
This study also doesn't show men's fertility being "destroyed".
Note: I brought this issue up to digdeeper in his MUC. He didn't seem to pay much attention to it. And, it seems that he hasn't rectified his errors in this article yet.
The COVID vaccine is not a vaccine
AKA words' definitions change and broaden over time
The meanings of words change over time. The vaccine is not genetic therapy, but it is also not a conventional vaccine technology like what has been used throughout most of history. Ultimately, it functions as a vaccine, so it is regarded as one.
Okay, that's enough. We can see from all of them that prevention is the name of the game. But does the COVID vaccine prevent getting COVID? No: >The COVID-19 vaccine does not prevent COVID-19. A person who is fully vaccinated can still contract the SARS-CoV-2 virus, which causes COVID-19, and may go on to develop the disease.
It lowers the chances of contracting COVID and lowers the severity of the disease. This would serve to ameliorate the pandemic.
Now let's compare to other vaccines, such as the tetanus one:
>Tetanus vaccines can completely prevent tetanus
And rabies:
>Rabies is a 100% vaccine-preventable disease
This is false, no vaccine will prevent a disease with 100% certainty, there are documented cases of people vaccinated against tetanus and rabies developing the diseases.[213][214] They will say that they are 100% preventable to express the fact that the vaccines are very effective (over 99%) at preventing illness, and encourage people to receive them.
The context of disease prevention with respect to these vaccines is not comparable. These vaccines are not analogous to COVID vaccines.
There are two contexts in which people are vaccinated against tetanus and rabies. Pre-exposure prophylaxis (PREP), and post-exposure prophylaxis (PEP). For COVID, there is only one, which is pre-exposure prophylaxis.
In the case of PREP for tetanus and for rabies, the vaccines definitely do not prevent the manifestation of disease 100% of the time.
To clarify up front, the analogy with tetanus is misleading from the very beginning, although I'm not accusing digdeeper of being misleading, he's just ignorant to this. Most people are vaccinated against tetanus across the course of their life. They have had multiple doses of the vaccine, giving them an established level of immunity.
These people can then go on to be exposed to tetanus, and you know what happens? They have to get another dose of the vaccine. They need to do this, because their established level of immunity is typically not enough to reliably prevent tetanus. It is high enough that one extra dose of vaccine will give them enough immunity to prevent tetanus, but not high enough to prevent tetanus outright. Their immunity wanes with time, so they can sometimes have had enough immunity to prevent tetanus, and go on to lose this. A person in their thirties who has regularly received boosters against tetanus throughout their lifetime and steps on a nail 3 years after receiving their latest booster will likely need another booster. If they don't receive one, they have a real chance of developing tetanus.
People who have no established immunity to tetanus, people who have never received a tetanus shot before, have to receive several doses of the vaccine over the course of a year. It can be up to three doses of the vaccine. If a person has a high risk of developing tetanus, from a severe wound, they can receive tetanus immunoglobulin as well, which is a separate injection. Tetanus immunoglobulin contains tetanus antibodies, which provides one with an immediate level of immunity against the tetanus toxin, so that one does not need to wait for their body to create its own antibodies.
Overall, tetanus vaccination can be characterized by multiple, repeated doses of tetanus vaccines. In this aspect, tetanus vaccination is no different from COVID vaccination. Furthermore, when given in the form of pre-exposure prophylaxis, tetanus vaccines, like COVID vaccines, do not prevent illness 100% of the time.
In the case of PREP for rabies, PREP only expedites the process of vaccination, it does not provide full immunity by itself. PREP for rabies consists typically of two doses of rabies vaccine. This provides a person with partial immunity to rabies. This is not full immunity, it is only partial. If a person who has gotten PREP rabies vaccines is bit by a rabid animal, and they do not receive treatment, they will likely develop rabies and die. A person who has gotten PREP rabies vaccines and is exposed to rabies must receive two more doses of rabies vaccine in order to ensure that they do not become prodromal.
Rabies PREP merely speeds up the process of vaccination. It's really just intended for people with a high risk of exposure to rabies, who live in rural areas that make it difficult and or costly to seek medical treatment. Farmers, for instance, who may be unable to afford to go to the hospital which is 8 hours away, 4 times in one month, in order to get vaccinated against rabies.
Most people vaccinated against rabies receive their vaccines in the form of post-exposure prophylaxis, not pre-exposure prophylaxis.
There are two kinds of post-exposure prophylaxis vaccine regimens administered in the case of rabies. There is a regimen of rabies immunoglobulin combined with rabies vaccines, and there is a regimen of only rabies vaccines. Rabies immunoglobulin contains rabies antibodies, which provide one with immediate immune protection from the rabies virus, and also can kill rabies virus in one's system.
In the West, immunoglobulin seems to be administered quite often. In less-resourced nations, such as Turkey, it is less common, due to the cost of manufacturing it, and so it is only administered in cases where a high viral load is suspected.
The rabies vaccine regimen with immunoglobulin consists of 5 injections. The first day will be 2 injections, one of immunoglobulin, one of the rabies vaccine. The following 3 doses of rabies vaccine are spread across the subsequent weeks. If immunoglobulin is not recommended, it will be 4 doses of rabies vaccine spread over the course of several weeks. If the subject is immunocompromised, then it is usually 5 doses of rabies vaccine instead of 4.
This is far more doses than most people ever received for COVID.
The rabies vaccines are not any different from the COVID vaccines in the sense of repeated vaccination, and in the sense of PREP not reliably preventing illness.
The rabies and tetanus vaccines are extremely effective at preventing disease in the context of post-exposure prophylaxis. The vaccine regimens are serologically calculated to eliminate any and all of the targeted pathogen/toxin in your body. There are specified levels of antibody titers intended to prevent the manifestation of disease. The vaccines are designed to bring you to the appropriate antibody levels. If your antibody levels are below a certain threshold, you can become prodromal, and, in the case of rabies, almost certainly die. Immunocompromised people sometimes need to get their antibody levels tested while receiving the rabies vaccine regimen.
In the context of how the rabies and tetanus vaccines are administered, it is usually not for the sake of merely developing immunity prior to infection, but rather for the sake of eliminating the pathogen within your system. In the process of doing this, you develop immunity.
You cannot do post-exposure prophylaxis for COVID.
The dynamic of the diseases are different.
The incubation periods for tetanus and rabies are typically very long when compared to COVID.
The incubation period for tetanus is usually 1-2 weeks, but it can be several months.[215] For rabies, the incubation period is usually one to three months, but sometimes can be weeks to days,[216] and in rare cases can be years,[217][218] possibly even decades. For COVID, the incubation period is usually just a couple days.[219][220] This is far shorter.
The long incubation periods for rabies and tetanus provide one with more than enough time for their body to develop immunity, and eradicate any pathogen in their system, before disease manifests. The existence of immunoglobulins, which can provide immediate protection, and even neutralize pathogen/toxin, also adds to this effect.
When it comes to COVID, after being vaccinated, you may not necessarily have enough time to develop full immunity by the time you're exposed to the disease.
Some other reasons why vaccines for tetanus and rabies are more effective than COVID vaccines:
Tetanus is caused by a toxin, not a virus causing physical damage within the body.[221] The dynamic here is very different. The tetanus toxin doesn't really change across strains.[222][223][224] The tetanus vaccine targets this toxin, and does not target the bacterium itself. So, the bacteria can mutate and develop into strains, but it's insignificant, because their disease-causing toxin, which the vaccines target, remains virtually the same. This enables the vaccines to consistently prevent illness.
Rabies is much less mutagenic than COVID. Part of the reason why is because it is much less infectious than COVID, due to the dynamics of how the virus proliferates. It essentially proliferates solely through direct contact via bites and/or scratches from saliva-contaminated claws, and has extremely low human to human transmission, usually reserved to freak accidents with medical procedures e.g rabies-infected blood, or organs. As a result, it has less opportunity to evolve some new pathways for infecting humans that would impact the effectiveness of current vaccines. Also, at a baseline it seems like COVID is inherently more mutagenic than rabies, meaning that in isolation COVID seems to mutate faster.
Because rabies is less mutagenic, rabies variants tend to largely retain their viral surface proteins, which are what enable the infection of hosts. COVID variants, on the other hand, have had their spike proteins change considerably over the passage of time. Since rabies' viral surface proteins are largely unchanging, the vaccines will consistently prevent illness. But with COVID, the virus and its spike proteins frequently change, and as a result the vaccines do not consistently prevent illness.
Rabies and tetanus both need to progress to the brain in order to manifest as illness. The proximity from the wound/point of exposure to the brain typically determines the incubation period. Someone bit on the head by a rabid bat will likely develop rabies much sooner than someone bit on the toe. So the same for someone who stepped on a nail in the woods, as opposed to someone who cut their hand, or had a head injury of some sort.
At the time of exposure, the pathogen is largely isolated to the part of the body it was introduced to. While in that part of the body, it can't do much of anything to harm you. So, you get vaccinated, which supplies you with antibodies, which in turn proliferate throughout your system and neutralizes any virus or toxin before they reach your brain.
With COVID, you can introduce the virus to your system through mucus membranes, like by touching your face with contaminated hands, or by inhaling virions. The infection from that point is immediate. It will proliferate throughout your respiratory system, and can spread further. It's not as though the virus has to progress along the nerves in your body until it eventually reaches the brain, like rabies. There's simply no time for a vaccine to step in and cut off the infection.
Bear in mind, the same is true for rabies and tetanus. When rabies becomes prodromal, and has thus begun to proliferate throughout your brain cells, immunoglobulin and vaccines will in all likelihood do nothing to save you. There's a very weak correlation, possibly none at all, between the vaccination of prodromal rabies patients and their survival. In a lot of rabies cases I've read, the doctors usually administered immunoglobulin as a desperate attempt to save the patient, but it never really works. Still, they had to try something.
You have also not considered the fact that rabies and tetanus are and were far better understood than COVID and vaccines against them have existed for far longer. Literally, one of the first vaccines ever made was for rabies, that was over 100 years ago.
For a less than 100% effective vaccine, look to the flu. Let's quote a source you cite in your own article: [225]
>The flu vaccine is usually moderately effective with the CDC estimating that it “reduces the risk of flu illness by between 40% and 60%.”
Why didn't you freak out and claim that it's not a vaccine? After all, it's even less effective than the COVID vaccine. Probably because that would not be ideologically convenient. You wouldn't be able to single out the COVID vaccine, you would have to acknowledge the flu vaccine, and then, you'd open up the possibility of other vaccines also not being "100% effective" (which none are). Only in a vacuum of context, of knowledge, can this be done.
All this being said, you don't even need to have an understanding of these vaccines and their respective pathogens and toxins to refute this argument. Something not being 100% effective does not mean that it has no utility whatsoever. This is childish. Airbags and seatbelts don't guarantee that you won't break your neck and die in a wreck, but you wear them anyway. They can even trap you in your car, and you can burn to death in a fire. But, it's more likely for them to save you than for them to trap you in a burning car.
While on the topic of rabies; The rabies virus is itself also quite fragile and weak. I bring this up because a grifter mentioned in the article tacitly suggests people to take garlic if they've been exposed to rabies.
Garlic is not going to kill rabies inside of someone's system. If you get bit by a rabid dog and eat garlic thinking it'll save you, it won't, you'll just die a horrible death a couple weeks or months later. Garlic might kill rabies virus externally, but that's meaningless. Heat kills rabies. Drying/air kills rabies (it can only survive in saliva and nerve cells). Sunlight kills rabies. It is a very delicate pathogen. It would be completely insane to favor garlic over vaccination, which is implied by one of the psychotic cranks you've cited later in your article
Renowned herbalist Richard Schulze (who ran a clinic for decades, curing all kinds of allegedly incurable diseases) heavily praises garlic:
>Garlic has been tested against many viruses and is known to destroy on contact the viruses that cause ... Rabies
Unless he's shilling some kind of garlic disinfectant spray which happens to kill rabies, just like most other disinfectants, I couldn't see this as anything but a suggestion to just take some garlic if you've been exposed to _RABIES_. There's only been a couple dozen documented survivors of rabies over the decades, most of them with debilitating long-term neurological sequelae, out of the tens of thousands who die from it annually. Statistically speaking, some of those people who died probably ate garlic during the incubation period, yet it didn't save them. Don't take his insane advice.
I'll briefly go over Schulze later when he shows up chronologically. The guy is a dumb fuck, and a piece of shit putting lives in danger.
What should we call it? How about an arbitrary code execution exploit, but for humans? Since that's what the mRNA vaccines literally are. Funnily enough, they started changing the definition of the word "vaccine" on some sites to protect the COVID genetic therapies.
It's not a genetic therapy. mRNA does not alter DNA. Going off of the current understanding of human biology, it seems to be mechanistically impossible for it to do so. The mRNA goes into your arm's muscle cells and inside it instructs them to produce spike proteins. The cells then present the spike protein on their surface. The immune system then recognizes these as being foreign and attacks them, producing antibodies. Eventually, the mRNA degrades and the body ceases producing spike proteins. That's it.
The studies you cited don't prove that the COVID mRNA vaccines alter people's DNA.
(your study)[226]
>Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line
Here's some criticism of the study.[227]
>... this experiment was done on cells being grown in a lab ... In vitro experiments are done all the time and they are important for providing information and clues as to what might happen in a person (“in vivo”). However, to make a conclusion about what is happening in people, one must have some evidence that it is actually happening in people, not just that it might be possible. The authors acknowledged this when they wrote, “At this stage, we do not know if DNA reverse transcribed from BNT162b2 is integrated into the cell genome. Further studies are needed …” (p. 1122). They go on to suggest two alternative experimental methods for getting more information.
>The authors used a cancerous liver cell line. This is important for two reasons; both of which were acknowledged by the authors. First, cancerous cell lines replicate, whereas our liver cells typically are not replicating. As such, even if DNA representing the viral RNA was integrated into the cell, no other cells with the altered DNA would be produced. The authors also pointed out that this cell line has been shown to have genetic and protein expression differences specific to RNA metabolism (p. 1123). This means that what is seen in these cells may not be representative of what would happen in non-cancerous liver cells (or even a different line of cancerous liver cells). Second, they measured LINE-1 activity. Importantly, LINE-1 has been associated with various disease-related conditions, including cancer. It has also been shown to affect immune responses. For these reasons, while the changes related to LINE-1 are interesting, we can’t be sure the effects would be the same in a non-cancerous cell line. The authors also made this point by stating, “The exact regulation of LINE-1 activity in response to BNT162b2 merits further study.” (p. 1123).
You then brought up some study[228] that proved RNA from COVID (and thus presumably the mRNA vaccines which contain it) can get integrated into your DNA
, no massive leaps to any conclusions there. Here's some criticism of it.[229]
>The first thing to keep in mind is that the coronavirus is an RNA virus, so there's a big barrier to getting that integrated into the DNA genome of a cell. You need a reverse transcriptase enzyme, one that runs the usual tape backwards and makes DNA out of an RNA sequence instead. We humans don't do that ourselves, but there are plenty of viruses that do. And over the untold millennia, we have been infected by many of these, and a good amount of the stuff that they jammed into our genome is still there. This information freaks some people out when they first learn it, but it's true: somewhere around 5 to 20% of our genomic DNA appears to be detritus from ancient retroviruses.
>You can see evidence of this in retrotransposons, which likely have a retroviral origin and can at any rate act like built-in retroviruses. We have a lot of those in our DNA, because they just keep on copying themselves. A particularly well-studied case is the LINE1 sequences. There are a lot of these in the genome, and most of them have deteriorated to the point that they are inactive. But every human still has a few dozen of them that can be expressed into active proteins, among them a reverse transcriptase that then turns around and makes LINE1 DNA and inserts it back into the genome. In mammals, these sequences seem to have undergone evolution inside our cells, showing the history of a long-term "arms race".
>So our cells don't have any need for a reverse transcriptase themselves, but we have one running around thanks to LINE1. And the PNAS paper under discussion presents evidence that under some conditions, this enzyme can pick up coronavirus RNA during an infection, make DNA off that sequence, and insert it back into the genome of a cell. In the paper, though, those conditions include modifying the cell lines so that they have even more LINE1 than usual, and this is one of the reasons that the extension of these results to real-world infections has been challenged. An earlier version of the paper also took incoming fire because the human/virus chimeric sequences they detected can also be produced artifactually, but this latest version seems to have addressed many of those concerns.
>It's also important to note that even under the cell-culture conditions used here, the authors are just seeing some variable-length insertions from one end (the 3' one) of the viral genome. This process does not produce infectious virus. And it's also important to note that authors themselves say that these results in no way imply that the mRNA vaccines cause integration of Spike protein into a cell's DNA, either. The mRNA in the vaccines does not look like the 3' end of the viral genome - they have completely different "untranslated regions" (UTRs), and for what it's worth, the Spike protein itself is nowhere near the 3' end of the actual viral genome. A vaccination is enough to set off your immune system for future action, but it's really not like being infected with the virus, either in the scale of it all or in the many details.
Your application of those studies, in the pursuit of demonstrating the vaccines to alter DNA, fails. They experimented upon cancerous liver cells, which could be more prone to integrating genetic material from the vaccines into their genome than healthy muscle cells in one's arm. To demonstrate altered DNA, you would probably need clinical studies involving healthy humans, not some cancer cells extracted from a Japanese man in 1982.[230]
There simply is no parity between the two. The authors themselves in the study literally stated that there wasn't proof of genomic integration of the DNA that the cancer cells reverse-transcribed parts of the mRNA into, meaning there's not proof of any sort of persistent genetic alteration with the sort of cells the study concerns. This is a pathetically flimsy argument.
You can rant about the mRNA vaccines "getting your body to directly execute external instructions", but viruses do this. COVID is forcing your cells to produce more copies of itself. Vaccines act similarly in how they encourage the production of an antibody. The mechanism is just different with mRNA, because you're not using a neutralized/modified pathogen. Arguably, it's a safer route, without the pathogen. It's also probably cheaper, in part due to the fact that you don't need to take prophylactic measures to ensure that your vaccine pathogen is indeed neutralized, among other things, like cultivating the pathogen, and modifying it if it's a live pathogen as opposed to a netralized one. You are ultimately choosing to be infected by what you believe is a bioweapon, and have your cells forced to create more copies of a bioweapon, instead of having a vaccine instruct your body on how to not be infected by said bioweapon.
The vaccine contains self-assembling nanotechnology
To prove this, digdeeper cites this study,[231] which he says was "extremely well done", because it adhered to all of his biases.
Where am I? On Infowars? NaturalNews? The Covid Blog? No, it's an actual scientific journal.
No, it's not an "actual scientific journal". Some anti-vaxxers got together and made a journal of their own to publish lies about vaccines, because they could never get their lies published in reputable journals, due to the peer review process, and the mountains of contrary evidence that would crash down upon their lies. Creationists and other idiots do the same thing. I can go grab a bunch of people and make a journal with them and we can publish studies of our own proving whatever bullshit we want. Having this information and our identities tied to a journal doesn't make it true, nor does it make us any more credible than we would otherwise be. The deciding factor is the authenticity of the information, which comes down its veracity in the face of falsifiability. If a journal consistently puts out authentic information then they could be deemed reputable. This is nothing more than an appeal to authority. While that doesn't immediately discount your argument, you haven't even established these people as an authority worth considering — as a legitimate "authority". Your basis for considering them is that they pander to your personal beliefs.
Something that stands out to me as suspicious is the fact that their study seems to affirm all sorts of bizarre conspiracy theories people had, such as 5G worsening COVID, prior to there being any evidence to support these theories — back when the theories were completely unfounded. It is as though they are affirming people's delusions. They just conveniently found self-assembling nanotech and postulated that this would conduct 5G waves? You, on the other hand, take this as a plus.
>Young Mi Lee, MD Practicing Physician, Hanna Women’s Clinic Doryeong-ro 7, KumgSung Building, 2nd Fl., Jeju, Jejudo, 63098, Republic of Korea (South Korea)
>Young Mi Lee, MD, is a practicing physician specializing in obstetrics and gynecology, and is also a reproductive endocrinologist; because of her work over the last three years she has become an expert in stereomicroscopy and in the microbiology of incubated COVID-19 injectables, especially, Pfizer and Moderna
What is it to be an expert in "the microbiology of incubated COVID-19 injectables"? I guess I'm an expert too, since I have an idea of their mechanism. How do they know that because of her work she has "become an expert"? Did she obtain some kind of qualifications? No.
>Daniel Broudy, PhD Professor of Applied Linguistics, Okinawa Christian University
And a linguist. I wonder what he would know about microbiology or nanomachines (precisely nothing).
>The contents of COVID-19 injectables were examined under a stereomicroscope at up to 400X magnification. Carefully preserved specimens were cultured in a range of distinct media to observe immediate and long-term cause-and-effect relationships between the injectables and living cells under carefully controlled conditions. From such research, reasonable inferences can be drawn about observed injuries worldwide that have occurred since the injectables were pressed upon billions of individuals. In addition to cellular toxicity, our findings reveal numerous — on the order of 3~4 x 106 per milliliter of the injectable — visible artificial self-assembling entities ranging from about 1 to 100 µm, or greater, of many different shapes. There were animated worm-like entities, discs, chains, spirals, tubes, right-angle structures containing other artificial entities within them, and so forth. All these are exceedingly beyond any expected and acceptable levels of contamination of the COVID-19 injectables, and incubation studies revealed the progressive self-assembly of many artifactual structures. As time progressed during incubation, simple one- and two-dimensional structures over two or three weeks became more complex in shape and size developing into stereoscopically visible entities in three-dimensions. They resembled carbon nanotube filaments, ribbons, and tapes, some appearing as transparent, thin, flat membranes, and others as three-dimensional spirals, and beaded chains. Some of these seemed to appear and then disappear over time. Our observations suggest the presence of some kind of nanotechnology in the COVID-19 injectables.
>Materials and Methods
>Fifty-four samples were used in the study: 50 residual injectable vials (43 Pfizer, 7 Moderna) acquired immediately after their use in the COVID-19 vaccination campaign, and 4 unopened new injectable vials (2 Pfizer, 1 AstraZeneca, 1 Novavax). Initial observations were made on Pfizer and Moderna products under an Olympus stereomicroscope on the same day the vials were first used. Residual fluids in the vials were preserved at −20° Celsius in a laboratory freezer for subsequent study. Later, after thawing, the residual samples were placed in various culture mediafor long-term observation.The objective was to observe any changes that might occur over time and that might be observable under the microscope
>The Makler chamber aided in an accurate method of counting unidentified floating materials in the various products.All vials were preserved by refrigeration at −20° Celsius and were examined under the microscope after thawing at room temperature (RT) to approximate more closely the environment at sites where the injectables were administered —hospitals, clinics, and other health institutions. Because the study involved numerous data points, it was exceedingly difficult to control all the samples and associated lot numbers, so we offer Table 1 containing only the ones that were tracked and could be confirmed.
>Blood and semen samples were also examined for their exposure and potential reactions to all four COVID-19 injectables with the flu vaccine and normal saline(0.9% Sodium Chloride)being used as controls.
>To rule out bias and possible confusion with blood potentially contaminated from injectable contents, a whole blood specimen was collected from a non-vaccinated participant and plasma was prepared from a supernatant layer via natural sedimentation for approximately 3 hours at room temperatureto avoid any kind of mechanical damage from the centrifugation. In the interest of preserving natural coagulation mechanisms and avoiding unexpected biochemical intervention, for the purity of the samples (blood or plasma), this procedure did not use anyEDTA-coated containers.
>Eight separate glass slides were prepared for observation of how injectables interacted with blood samples. Each of the first four slides held one drop of whole blood and a micro drop of each injectable. The drops were positioned in a way that interaction could be easily achieved and observed with the use of cover slips whichallowed for the progressive mixing of samples. Four plasma samples were, subsequently, treated for observation in the same way. In the interest of understanding interactions of the injectable materials in various media —blood plasma of non-injected persons, whole blood of such persons, semen samples from injected and non-injected males, and various other liquid media over time. Digital documentation of the changes in bodily fluids and living cells was accomplishedby repeated video recordingsover regular intervals from 5~10 minutes, 30 minutes, 1 hour, 2 hours, or more, and for studies involving just the injectable materials incubated in various fluids, the recordings varied from intervals of days to weeks and months as are reported in our Resultssection.
>(Pharmaceutical Technology, 2024). A minute sample (0.03ml) of each injectableproduct (Pfizer 1, 2,and4, Moderna, AstraZeneca, and Novavax), was added to normal saline, sterile distilled water, and Hartmann’s solution each contained in a separate culture dish (either a 1.2ml forembryo culture dish, 5-welled culture dish,or an 8 mlfor Petri dish) at room temperature (15~25 degrees Celsius, adjusted for seasonal changes) without any special addedmaterials.Threekinds of culture dishes and aschematic of each culture dish can be seen in Figure 2.Because of the way each dish was covered and maintained inrelativelysterile conditions, the possibility of outside contamination was minimal. Over the course of all the incubation studies run in parallel, there is strong evidence that none of the culture dishes were ever contaminated by any outside bacteria or fungal spores.
Well here's one potential avenue for contamination. "Relatively sterile". They think the risk is minimal, and they think that there's "strong evidence" for a lack of contamination. But these people are stooges.
Something I find bizarre. How are these nanomachines assembling in what is essentially a vacuum? How are they self-assembling in distilled water? How are they self-assembling amidst sodium chloride? Matter cannot just come out of nowhere. The nanomachines need resources to be able to assemble. Is it coming from the water? If so, how? I don't think it's possible to form some crystalline, carbonic structure out of water. There's no carbon in water. Nor is there in salt. So, perhaps it would depend upon the vaccine solution.
Definitely couldn't simply be that this study is a crock of shit, and the dipshits who conducted it didn't think of this while they were fabricating evidence or letting mold grow in a petri dish and then thinking it was nanobots.
>Figure 2. Various culture disheswith ahand-drawn schematics and notations
Is this drawn in magic marker? This is hysterical.
>The solutions containing added crystals included (1) various brands of colloidal silver and gold, mica (aKorean mineral complex), (2) EDTA(ethylenediaminetetraacetic acid, a chelator that readily attaches to iron and calcium, which is an aminopolycarboxylic acid with the formula [CH₂N₂]₂), (3) silica water, and (4) baking soda.
>Blood plasma reactions were also studied with separate specimens taken from two non-vaccinees. Each consisted ofthe supernatant of the person’s whole blood separated via natural sedimentation. The sample of blood was merely left standing for about 3 hours in a containerto obtain the plasma after most oftheblood cells accumulatedin the lower part of the container
>Throughout the entire incubation period,which exceeded one year, no signs of bacterial or fungal contamination were observed in any of the mRNA vaccine specimens(Pfizer and Moderna). This is noteworthy because we did not rely on periodicexposure to any of the typical antibiotics orantifungal agentsthat arecommon to basic incubation studies. Because we were persuadedfrom direct microscopic observationsin an earlier short-term incubation study (not presented here)that these foreign materials are not organic, but rather at least synthetic hybrid organismsor possibly animate robotic structures, we adopted an atypical approach to incubation
These are quite extraordinary findings they've made.
There's a few potentialities:
(1) The vaccines contain self-assembling nanotechnology
(2) The vaccines don't contain self-assembling nanotechnology
(2a) The study's evidence was falsified
(2b) The authors made some mistakes that contaminated the samples, and due to their inexperience, they were unable to identify these mistakes
(2c) The authors are observing innocuous materials contained in the vaccines
(2d) A combination of the three points above.
(1) Meaning there has been a conspiracy to contaminate Moderna and Pfizer vaccines with this technology.
This is presumably a large conspiracy, as they are assumedly contaminating a significant portion of the doses, if not all of them.
What other evidence is there of this conspiracy?
Billions of people got Pfizer and Moderna vaccines. Surely, some of these people have had medical issues at some time proceeding vaccination and had have biological samples extracted from their bodies and analyzed, e.g blood, potential tumors, spinal fluid. Surely, some of these people volunteered to be parts of scientific studies and had to have biological samples taken from their bodies and analyzed before participating? Surely, people wanted to donate things like blood, or plasma, or bone marrow, or organs, or whatever, and had these materials analyzed under a microscope? Surely some of these people died and had their bodies examined by coroners either during autopsies or because they donated their bodies?
Has anyone observed strange nanomachine structures in these samples? Well, there's no credible reports of it. It would probably be something people would report because that is not a normal observation to make. I think at this point it is extremely unlikely that people could not have independently verified the existence of nanomachines. There should be far more observations than there have been.
So, they've contaminated who knows how many doses, kept this a total secret, and nobody has verified the findings of this study.
It's ridiculous. Somehow, the only people discovering evidence of nanomachines are highly dubious fraudsters.
It's because there's no nanomachines. It's all made-up. Every single forensic sciences department that examines dead bodies across the whole world has to be in on the conspiracy. Every single coroner has to be in on it. In America, there are thousands of coroner's offices, hundreds of medical examiner's offices, and hundreds of forensic labs. They all have to be under total control.
And not just them. People who examine biological samples from living people, like at medical laboratories, also have to be in on it. We're talking about what is probably millions of conspirators worldwide right now.
In America alone there's thousands of facilities.
>This report provides data on the workloads, staffing, resources, policies, procedures, and budgets of the 326 standalone forensic labs and multilab systems (totaling 423 individual labs) in 2020. It also includes counts of employees and service requests in 2019.[232]
>A total of 2,037 unique and eligible offices were enumerated for the CMEC, of which 1,648 responded for an overall response rate of 80.9%.[233]
>A total of 2,112 ME/C officers were identified during verification efforts and were initially contacted to participate in the study. Of these, 44 were deemed ineligible based on responses to screener questions and 31 offices were compiled with another office's response. Of the remaining 2,037 unique and eligible offices, 1,648 responded for a total response rate of about 81%. Of the respondents, a total of 1,341 (82%) responded to the long version of the survey, and 307 (18%) responded to the critical-items version of the survey.[234]
Because you do not have any insight into these sorts of sciences, you foolishly think that it's actually possible for a conspiracy of this scale to be possible. You need to research criminal cases that involve forensic analysis of corpses to get an idea of how ridiculous this all is. It's Dunning Kruger, and nothing more. It's flat earther level paranoia, assuming that pilots, people who work in Antarctica, satellite operators, and so forth, are all in on it, or can somehow be fooled into not realizing that the earth is flat. In this case, coroners will just not pay attention to the suspicious nanomachines in the samples they observe. A shadowy figure standing over their shoulder will whisper into their ear, telling them to not worry about it, and they'll all magically listen. The hive mind is just that powerful, that the hundreds of thousands or millions of coroners worldwide will stay silent.
(2) Considering how improbable it is that these structures are prevalent in people's bodies but have gone completely undetected by everyone but anti-vaccine grifters, an alternative scenario is that the people who authored the study are wrong.
(2a) Maybe they faked the evidence. As of now, there's no evidence for that. But, this study doesn't have much attention as of yet. There's presumably only been two people involved in it as well. Shams like Wakefield's vaccine autism claims were disproven, but the dynamic of his study was different from their's. To disprove his study, all people had to do was interview children's families and learn that some of the children weren't autistic at all and others were autistic prior to vaccination. Who can you interview other than the two people behind this study? What evidence can you find that they faked evidence? Probably not any. At which point, the only option is to reproduce their study.
(2b) Maybe the authors contaminated the samples somehow, and due to their inexperience, they were oblivious to these mistakes. They stated that they kept these samples around for months to observe them. There isn't any chance that the samples got contaminated in that timeframe?
What "expertise" did you want? Running the microscope, with a sprinkle of analytical thinking, should be enough
They have no idea what they could be doing wrong. If you don't know what you may not know, then there's no way of knowing what you do and do not know. Take an example of the Dunning Kruger effect with so-called "race realists" i.e racists who try to use science to make their racism seem more justified, nuanced, and meaningful. One time I saw this white supremacist online show a study that measured some chemical in people's genes, and basically there was a bar chart showing different genes, and the amount of this chemical measured in each type of gene. I think it was acetylcholine. There were genes relating to the nervous system, genes relating to metabolism, genes relating to pigmentation, skeletal structure, all sorts of genes. The white supremacist presented the chart, saying that it proved that when going off of ethnic groupings, genes for the brain have more genetic differentiation than genes for pigmentation. They used this to effectively debunk the claim that race is only skin deep. Amazingly, the chart they displayed directly contradicted their statement. They didn't realize that the bars were measuring similarity, and not difference. They saw that genes for the nervous system had the biggest bars, and in their troglodyte mind thought "Big bar meen moar difrent". Because of how little they knew about genetics, they were utterly incapable of comprehending the supposed evidence that they were citing.
There's all sorts of contamination that could be occurring. If they don't know what they're doing, they won't know how to facilitate a reliable study. I'm not going to trust in the abilities some creditless "expert in the microbiology of COVID-19 injectables" and a linguist from some joke Christian "university". These people have no clue what they're doing.
>Various kinds of transparent ribbons, films, coils, and spirals appeared in the Pfizer sample incubated in distilled water. These were very similar in structure to the micro- and magnetic- nanorobots already presented in numerous scholarly papers (Zhou et al., 2021). These structures, according to numerous researchers, could serve as signal conductors, biosensors, switches, and/or electronics devices needed for the transhumanist movement toward a post-human society
These structures ... could serve as signal conductors, biosensors, switches, and/or electronics devices needed for the transhumanist movement toward a post-human society
Definitely the words of sane, non-biased researchers here.
The structures in the Zhou paper don't look similar to me.[235][236]
Some of them are designed to imitate biological organisms like algae. So, what they've found could be nanomachines imitating microorganisms, or they could be actual microorganisms, like algae or fungi.
Not to mention the strength of the fields necessary to manipulate these from a distance. Probably not something that can be achieved outside of a controlled environment with specialized, heavy-duty equipment.
(2c) Or maybe they've found stuff that is in the vaccines, but is innocuous.
I think it's probably a combination of things. Contamination and potentially things that really are in the vaccines but are innocuous. The only way to know would be to reproduce the study. It seems like nobody is interested in doing this. Probably because of how batshit insane it is.
Nonetheless, nobody has to reproduce the study. The existence of forensic sciences labs, and medical labs, proves that this is a crock of shit. Every single person whose work involves looking at biological materials from humans under a microscope has to be in on it. You might be thinking, "But what about XKeyscore", or the Manhattan Project, or some other conspiracy, but that's a non-starter, because those conspiracies were all exposed, were magnitudes smaller than this conspiracy, had significant contextual differences from this conspiracy, and in the two that I named, only took like 3 years to be revealed.
The authorities' useless coronavirus response
If the lockdowns worked, we should expect the cases to go down after the restrictions get implemented. Sure, some countries - such as Austria or Belgium - do follow that pattern; but others - like Ireland, Israel or Poland - have cases shoot up after the lockdowns. This shouldn't happen if these measures worked to contain the spread; the cases should either fall or at least not rise. Funnily enough, the Netherlands have had their amount of cases fall after the first lockdown, but rise after the second; clearly showing the lockdowns have nothing to do with it!
There's a few things you're not considering:
(1) People could (and did) disobey lockdown guidelines
(2) People could be infected prior to a lockdown and become symptomatic prior to its instatement
(3) Certain countries could have implemented lockdowns too late for them to be effective
Notice how cases were on the rise in Poland, Ireland, and Israel, but in Belgium and Austria they were on the decline, when lockdowns were implemented.
(4) Not all lockdowns are equal. Certain countries could have inadequately enforced lockdowns in terms of the lockdown policies.
Measures taken to lower transmission not being 100% effective does not mean that they were ineffective. They were effective in some countries, and in others they weren't. Overall, it appears that they did not significantly reduce mortality, and the effect on transmission varied from country to country. So, the harms brought about by the lockdowns could be seen as a greater cost than the benefits brought about by the lockdowns, which weren't consistent. This appears unlikely when looking at places like Sweden and Belarus which did not take COVID seriously and experienced many deaths as a result.
Either way, this is not an indictment against the authorities, as the effectiveness of a lockdown can only be gauged in retrospect. It does not indicate a conspiracy. At most, it could indicate incompetence/bad investments on behalf of the authorities.
In America there is evidence that lockdown measures and adherence to measures for preventing the spread of COVID like masking, social distancing, and vaccination, was effective. America, unlike many other countries, is a decentralized dumpsterfire of a country, where your ability to be sent to prison for certain "crimes" is determined by which state you inhabit. COVID policies varied across partisan lines.
Red (Republican) states in America had higher rates of COVID death than Blue (Democratic) states.[237] During COVID, you'd struggle to find just one democrat that was opposed to COVID vaccination. Virtually all of the COVID anti-vaxxers were right-wingers, which is conducive to voting Republican. So, I would not say that the lockdown measures were entirely ineffective. I would say that they weren't entirely effective, which comes down to humans' inability to properly implement and adhere to the measures. Hopefully, next pandemic, if there should be a next pandemic, which there might be, people don't act like idiots.
Quoting from the study I just cited which found Red states to have higher COVID death rates than Blue states.[237]
>Highlights
Political party-affiliation has shaped response efforts to the COVID-19 pandemic.
Red states had higher COVID-19 infection rates and deaths in 2021 compared to blue states.
Red states implemented fewer political decisions to mitigate COVID-19 than blue states.
Biological factors such as age and obesity predicted deaths only in red states.
Vaccination rates predicted fewer deaths in blue states.
>The study investigated infection variables and control strategies in 2020 and 2021 and their influence on COVID-19 deaths in the United States, with a particular focus on comparing red (Republican) and blue (Democratic) states. The analysis reviewed cumulative COVID-19 deaths per 100,000 by year, state political affiliation, and a priori latent factor groupings of mitigation strategies (lockdown days in 2020, mask mandate days, vaccination rates), social demographic variables (ethnicity, poverty rate), and biological variables (median age, obesity). Analyses first identified possible relationships between all assessed variables using K-means clustering for red, blue, and purple states. Then, a series of regression models were fit to assess the effects of mitigation strategies, social, and biological factors specifically on COVID-19 deaths in red and blue states. Results showed distinct differences in responding to COVID infections between red states to blue states, particularly the red states lessor adoption of mitigation factors leaving more sway on biological factors in predicting deaths. Whereas in blue states, where mitigation factors were more readily implemented, vaccinations had a more significant influence in reducing the probability of infections ending in death. Overall, study findings suggest politicalization of COVID-19 mitigation strategies played a role in death rates across the United States.
>The current study has four objectives:
>1) to differentiate naturally occurring clusters based on all the variables assessed (biological, social demographic, and mitigation strategies), and to assess if these clusters differentiate between red, blue, and purple states;
>2) to investigate whether the states’ political affiliation as red or blue is associated with COVID-19 deaths in 2020 and 2021;
>3) to investigate to what extent COVID-19 deaths are predicted by biological, social, and behavioral/political mitigation variables overall.
>4) to investigate to what extent COVID-19 deaths are predicted by biological, social, and behavioral/political mitigation variables in red and blue states.
>We focused on COVID-19 cases and deaths of 2020 and of 2021 separately, considering the Delta variant and the availability of vaccines.
>2. Method
>Data was gathered from all fifty states within the United States, including data for bio-demographic, socio-political, and behavioral mitigation variables to measure the effects of COVID-19 deaths from previously documented data. Specific data sources are identified below.
>COVID-19 cases and deaths were categorized per state for 2020 and 2021 by the “CDC Data Tracker” and organized per 100,000 instances. The Center of Disease Control and Prevention (CDC) Data Tracker collects surveillance measurements on confirmed COVID-19 deaths from hospitals, healthcare systems, and laboratory data from various community, state, and territorial public health departments [36]. The COVID-19 cases and deaths count for this study were assessed from January 21, 2020, to December 31, 2020, for the year 2020 and from January 1, 2020, to October 25, 2021, for the year 2021. The years 2020 and 2021 are separated because of the impact and presence of vaccine in 2021. Additionally, within the CDC Data Tracker, New York State and New York City were separately recorded for 2020 and 2021. For the purposes of this study, New York State and New York City data was combined to provide the most accurate picture of the overall population.
>2.2. Predictor variables
>Bio-demographic
>Adult Obesity Rate. The adult obesity rate for 2020 was published by the Robert Wood Johnson Foundation project and reported the data collection from the Behavioral Risk Factor Surveillance System (BRFSS) conducted in 2020. The BFRSS is a cross-sectional survey administered to each state in the United States that investigates behavioral health risk factors for individuals 18 and older in each state, which includes state obesity rate measured by the body mass index, BMI [37]. The data recorded for the BRFFS in 2020 on the obesity rate per state was measured by the percentage of adults with a BMI of 30 or higher.
>Median Age. Median age by state in 2019 was collected from Statista [38] by collecting the ages of the population for each state and reporting the median age.
>Minority Population. The minority population per state variable was identified by the data from the 2020 Census on Race and Ethnicity in the United States [39]. The population percentage per state calculates the total population for minorities and does not include those of Hispanic Origin. The total population count for each state was categorized as Black, American Indian or Alaskan Native, Asian American, Native Hawaiian or Other Pacific Islander, Some Other Race, and 2 or More Races. In our analyses, however, we only focused on the two largest groups, Black and Asian American. Hispanic minority status per state was operationalized as the percentage of the population by state identified as Hispanic Origin and was also included in the analyses.
>Poverty Rate. The poverty rate, defined as the percentage of the population for each state that is in poverty, was collected from the 2019 Census in the U.S. with the 2019 American Community Survey [40].
>Socio-political
>The socio-political affiliation for each state was derived from collecting the Gubernatorial Party affiliation, State Senate affiliation, and State House of Representatives affiliation within the year 2021 [41], [42]. Overall political affiliation within the context of this study was measured as Democratic/blue or Republican/red. States with mixed political affiliations, commonly referred to as purple states, were excluded from the regression analysis for extreme comparison. This study defined the state’s political affiliation by the governor’s political affiliation and if either state senate or state house had the same political affiliation as the governor. If the governor’s party affiliation was different from both state senate and state house, then we coded this state as purple. There were 22 red, 16 blue, and 10 purple states. The two states, Montana and West Virginia, where state governors changed in 2020 were also excluded from state comparisons.
>Often in research, the presidential election results are used to determine red, blue and purple states in studies [32]. Since COVID-19 related measures in states are often initiated by the state’s executive branch, i.e., the governor, this study primarily relied on the governor’s political affiliation. A state was defined as blue if the governor was a Democrat and either state senate or state house are democratic. A state was defined as red if the governor was a Republican and either state senate or state house are republican. If the governor’s political affiliation is different from the dominant affiliation of state house and state senate, then the state was defined as purple.
>Behavioral / political regulations
>State Lockdown Days for Year 2020. The behavioral variables measured for the year 2020 for this study included the number of lockdowns by state. The number of lockdowns per state was defined by the state lockdown order issued by state government officials [43], where each state is listed with the dates of the lockdown order, state lockdown report, and title of the order. The numerical count for the amount of lockdown duration reported in days was calculated by taking the difference between the start date of a lockdown order and the end date of a lockdown order by the state documented on state orders.
>Mask Mandate Days for Years 2020 and 2021. Mask mandate by state, measured by the number of days the mask mandate was issued until lifted by state officials, was reported for 2020 and 2021. The mask mandates were identified as those reported on U.S. News and World Report [13]. The number of mask mandate days for each state was calculated by counting the days from when the mandates were initiated and lifted. Mask mandates were categorized for the year 2020 and year 2021 as active mask mandates or no mask mandates. The active status of mask mandates was documented for 2020 with the dates January 1, 2020, to December 31, 2020, and 2021 dates were January 1, 2020, to October 25, 2021.
>COVID-19 Vaccination Rate 2021. The COVID-19 vaccination rate was gathered from the CDC datasheet from October 25, 2021, for each state. It was defined as the total number of individuals 12 years of age and older fully vaccinated with the second dose of a two-dose vaccine or one dose of a single-dose vaccine [44]. No vaccination information was reported for the state of Idaho.
>COVID-19 Vaccination Mandates 2021. COVID-19 vaccination mandates were recorded in four settings: public schools, universities, hospitals, and places of employment in all 50 states. This study categorized the COVID-19 vaccination mandate active for each state on a scale from 0 to 4 (0 = no vaccination mandate in all 4 settings to 4 = vaccination mandates in all four settings).
>Public school COVID-19 vaccination mandates for each state were collected from Wong et al. [45] which reported secondary COVID-19 vaccination data derived from the CDC with a virtual map display. This study defined public school COVID-19 vaccinations per state with three measures. Responses were scored as (0 = no, and 1 = yes).
>University COVID-19 vaccination was reported by states that required vaccinations for on-campus or residential students for the 2021–2022 academic year but does not identify individual requirements issued by particular academic institutions [46]. Many institutions had separate vaccination guidelines for students and employees. Vaccination requirements issued by universities in this study only applied to student populations. This study defined University COVID-19 vaccination status with a dichotomous coding (0 = no, and 1 = yes).
>Hospital COVID-19 vaccination mandates were collected from the National Academy for State Health Policy [47], which reported state mandates requiring hospital workers and healthcare employees to receive the COVID-19 vaccine. For this study, Hospital COVID-19 vaccination mandates were coded as zero and one (0 = no, 1 = yes).
>Employee COVID-19 vaccination mandates were gathered from a listing of reported mandates by each state of vaccination requirements for employees [48]. This study categorized the employee COVID-19 vaccination mandate between 0 and 3 (0 = no, 1 = yes, state employees).
>Cluster 1: High Number of COVID-19 Deaths, Fewer Political Mitigation Measures, Fewer Vaccinations, and Higher Demographic Risk Factors
>The first cluster, the bigger cluster, is characterized by states that have high number of COVID-19 deaths per 100,000 people, implementing fewer mitigation efforts (e.g., lockdown days, mask mandate in days, and vaccine mandates), lower vaccination rates for ages 12 and up, lower median age, and higher risk factors such as obesity and poverty rate.
>Cluster 2: Low Number of COVID-19 Deaths, More Political Mitigation Measures, More Vaccinations, and Lower Demographic Risk Factors
>The second cluster, the smaller cluster, is characterized by states that have low numbers of COVID-19 deaths per 100,000 people, implementing more mitigation efforts (e.g., lockdown days, mask mandate in days, and vaccine mandates), higher vaccination rates for ages 12 and up, higher median age, and lower risk factors such as low obesity and low poverty rate.
>Regarding race and ethnicity, there were more African Americans and fewer Asian Americans and fewer Hispanics in the cluster with more COVID-19 deaths.
>Comparing cluster membership among blue, purple, and red states (see Fig. 2), blue states fall significantly more often into cluster 2 with fewer COVID-19 deaths, and red states fall significantly more often into cluster 1. Purple states fall almost equally often into cluster 1 and 2. There is a significant relationship between political state affiliation and cluster membership, Cramer’s V = 0.840, p < 0.001.
>To replicate the findings, we also conducted K-means cluster analysis for cumulative COVID-19 cases. Also, convergence was achieved after 5 iterations for 2 clusters. ANOVAs comparing each of the 11 scales (z-scores) among the two final clusters were significant with all ps < 0.04, except for Black population (p = 0.28). The cluster centers and the percentage distribution of the two clusters within each of the three political groups (blue, purple, red) were similar to the ones obtained for the cluster analysis of the COVID-10 deaths.
>Comparing cluster membership among blue, purple, and red states, blue states fall significantly more often into cluster 2 with fewer COVID-19 cases, and red states fall significantly more often into cluster 1 with more COVID-19 cases. Purple states fall almost equally into cluster 1 and 2. There is a significant relationship between political state affiliation and cluster membership (Cramer’s V = 0.843, p < 0.001).
Then there's a bunch of graphs illustrating how red states had higher death rates. Anyway, I'm done quoting from that study.
The closing of so-called "nonessential businesses" has resulted in massive unemployment. In this study, 59% of the participants lost their jobs due to the fake pandemic, which has contributed to their mental problems:
10000 Canadian restaurants shut down forever in 2020. At least 800000 people have lost their jobs as a result.
Due to the job losses, people are forced to rely on soup kitchens for their food:
Loneliness due to school closures and other measures heavily increases depression rates:
Nursing home restrictions make people kill themselves:
Teenage suicide attempts have heavily increased in 2020 compared to 2019:
Lockdowns traumatize teenagers:
Lockdowns contribute to mental disease in adults, too:
It's true that the isolation could be and was bad for people's mental health, and people did lose their jobs. But the alternative, which would be doing nothing to address COVID, would only have been worse.
Lockdowns also kill more directly in very cruel ways:
That's one guy who died and it got a lot of news attention because of the insanity of the situation. This doesn't prove a widespread phenomenon. The excess deaths point to COVID.
Masks decrease the amount of oxygen available to your body:
These are the findings of one study. Others have failed to establish this:
>The principal original findings of this investigation support our hypotheses that wearing either the surgical, flannel or N95 mask at rest and during submaximal and maximal exercise did not induce arterial hypoxemia, compromise maximal cycle exercise capacity nor substantially impact major cardiovascular exercise responses. This was true despite the significant elevation of peak end-expired peri-oral CO2 and depression of O2 within the mask of 0.8–2 %. However, despite the intransigence of arterial O2 saturation, subjects rated their dyspnea significantly higher during mask wearing.[238]
>Among 50 adult volunteers (median age 33 years; 32% with a co-morbidity), there were no episodes of hypoxemia or hypercarbia (0%; 95% confidence interval 0–1.9%). In paired comparisons, there were no statistically significant differences in either CO2 or SpO2 between baseline measurements without a mask and those while wearing either kind of mask mask, both at rest and after walking briskly for ten minutes.[239]
>Mask use did not decrease SpO2 levels in patients with or without asthma, regardless of type worn. Neither duration of mask use nor perceived asthma control correlated with a decreased SpO2 level.[240]
>Long-term use of N95s, when worn alone or with a mask overlay as an outer barrier, did not result in a significant physiologic burden for health care personnel over the course of 2 work shifts. Despite the fact that health care personnel reported subjective symptoms related to wearing N95s and that these complaints increased over time, worker tolerance for long-term N95 usage was high. Nurses’ compliance with wearing N95s was also high, even after long-term use. Findings from this study indicate that many health care personnel can tolerate long-term use of N95s, alone or with an outer barrier. Additional studies are needed to further examine factors that influence intolerance of long-term use of N95s among some health care personnel and the relationship between weight and N95 tolerance and compliance to identify ways to maximize worker tolerance of N95s before another biologic disaster occurs.[241]
>Objective: To assess the physiological impact of the N95 filtering facepiece respirator (FFR) on healthcare workers.
>Methods: Ten healthcare workers each conducted multiple 1-hour treadmill walking sessions, at 1.7 miles/h, and at 2.5 miles/h, while wearing FFR with exhalation valve, FFR without exhalation valve, and without FFR (control session). We monitored heart rate, respiratory rate, tidal volume, minute volume, blood oxygen saturation, and transcutaneously measured P(CO2). We also measured user comfort and exertion, FFR moisture retention, and the carbon dioxide and oxygen concentrations in the FFR's dead space.
>Results: There were no significant differences between FFR and control in the physiological variables, exertion scores, or comfort scores. There was no significant difference in moisture retention between FFR with and without exhalation valve. Two subjects had peak P(CO2) > or = 50 mm Hg. The FFR with exhalation valve offered no benefit in physiological burden over the FFR without valve. The FFR dead-space oxygen and carbon dioxide levels did not meet the Occupational Safety and Health Administration's ambient workplace standards.
>Conclusions: In healthy healthcare workers, FFR did not impose any important physiological burden during 1 hour of use, at realistic clinical work rates, but the FFR dead-space carbon dioxide and oxygen levels were significantly above and below, respectively, the ambient workplace standards, and elevated P(CO2) is a possibility. Exhalation valve did not significantly ameliorate the FFR's P(CO2) impact.[242]
The masks could increase blood CO2 levels though. They did in some studies.
Low peak expiratory flow is very harmful to people with any kind of breathing problems:
COVID will statistically cause more harm to those people than a mask will. COVID will kill them, a mask won't.
Three German kids have even been reported to have died from the masks.
Some guy on Bitchute saying something isn't proof of anything. According to the press in Germany there was a 13 year old girl who died and Schiffmann baselessly claimed that she was wearing a mask and that it killed her. But this was not determined by an autopsy, her cause of death was unclear at the time of her death. He claimed a few other children died as well but there wasn't even any evidence of said deaths.[243] In all likelihood, Schiffmann was lying.
Healthy adults also complain about mask side effects:
That's not as bad as getting hospitalized or dying or causing harm to others. Some of it could be psychosomatic. The studies I cited seem to suggest that, as some of the participants complained about the masks, yet no physical problems were discovered.
It's hypocritical to argue that masks will somehow block so many oxygen molecules from reaching a person's lungs and block so much CO2 from exiting through a person's mouth that they will suffocate, but will also do absolutely nothing to block a virus or virions, which are magnitudes larger than those molecules.
Ventilators are physiologically harmful and 2 / 3 of people on them die.
You get put on a ventilator because you're dying, so the high mortality rate is unsurprising. As for them being harmful: [244]
>Carbogen, a mixture of 5% carbon dioxide in either air or oxygen, has been proven to cure pneumonia in 12 to 24 hours and was routinely used by firefighters, hospitals and rescue crews on emergency patients in the United States in the 1940’s.
>It is an honor to introduce to you a miraculous medical intervention that was once commonly used in medicine but has now been forgotten. It’s safe, highly effective for many disorders, and is proven to cure pneumonia in 12 to 24 hours. Carbogen is the perfect remedy to use in place of mechanical ventilators in emergency medicine, especially for COVID-19.
It feels like someone... wants to sell me something!
>The article Carbon Dioxide by the late Yandell Henderson, discusses the routine use of carbogen by rescue crews in the 1940s generated by a device called an H-H Inhalator. Treat a patient with pneumonia using an H-H Inhalator and a rapid recovery will be induced.
>One of the hallmarks of severe COVID-19 infection is pneumonia and the difficulty breathing (dyspnea) and inflammation-induced damage of the alveoli in the lungs. Severe COVID-19 is pneumonia, and a cure for pneumonia has been known for almost 100 years.
>In the 1930s, Dr. Yandell Henderson reported to completely cure dogs with pneumonia in just 12 to 24 hours through the administration of carbogen.(20). It worked on dogs and on humans.
Yeah... Anyway
The studies this article provides I have cited here.[245][246][247]
They don't seem to suggest that ventilation does not improve a patient's chances of survival. There isn't a contrast between the ventilated and non-ventilated. The standing logic is that people will only be put on ventilation if they need it — if they are dying. It doesn't seem like something very easy to measure the overall efficacy of.
A lot of the article is just copied from this other news article that it cited.[248]
It seems that ventilators may have been overused during the pandemic and could have been harmful to people who did not need them. However, that does not mean that they are fundamentally harmful. They aren't, they have a legitimate function and can save people's lives. Medical professionals weren't calling for ventilator usage to be stopped entirely, they said it should be optimized: that there should be more nuance in who they are given to. That's a near direct quote from a physician interviewed in the livescience article. So again, this does not indicate a conspiracy, but it could be incompetence on behalf of the authorities.
The final proof that the authorities don't give two shits about your health is the fact that they have attacked measures that actually work. From the WHO again:
>FACT: Vitamin and mineral supplements cannot cure COVID-19
>Micronutrients, such as vitamins D and C and zinc, are critical for a well-functioning immune system and play a vital role in promoting health and nutritional well-being. There is currently no guidance on the use of micronutrient supplements as a treatment of COVID-19.
Click here to see this "fact" conclusively refuted and expose the WHO as the enemy of your health!
You didn't refute those, you repeatedly confused correlation with causation because you don't understand the physiological changes humans experience when their body is combating infections. We're going to go over that.
Measures that actually work
What is the proper course of action against infections, then? How about supporting your immune system - which is what has to deal with any kind of virus or bacteria, anyway? Here are some relevant quotes from the excellent book The Wheel of Health:
>These areas of infection due to the same cause were very varied in character and situation. One rat would have something wrong with its ear, another with its stomach, another with its bladder, and so on.
>Actually, 44 percent of the 92 rats had something wrong with their urinary organs; 24 percent with their ears and noses; 38 percent with their eyes; 21 percent with their stomachs and intestines; and 9 percent with their lungs.
>If a source of Vitamin A, such as butter, cod liver oil or egg yolk formed a part of the diet, infective lesions were never seen in rats, the addition of these substances to the deficient diets, generally resulted in rapid improvement and ultimate cure
Rats aren't humans, so this doesn't necessarily mean anything about humans.
So, rats fed shitty diets get infections - but the ones given a good diet don't and can in fact rapidly cure themselves - proving the WHO completely wrong
Rats aren't people. This book was released in 1938 by the way. The author died 70 years ago. This stuff is super outdated. Malnourished animals get sicker than fed animals, that's not a surprise.
Of course, these infections were unspecified, but there's no reason to think COVID-19 would somehow be exempt
There's no reason to not think it would be exempt either. These are rats from a study that is almost 100 years old, let's be serious. They didn't have the technology we have now to physiologically study these types of illnesses.
Vitamin A
The aforementioned Vitamin A works in rats, but how about humans? Sure enough - measles outcomes are better when it's not deficient:
Vitamin A is a treatment for measles in babies deficient in vitamin A, and is also recommended for acute measles cases. As it so happens, most people in developed countries aren't deficient in vitamin A. Babies in developing nations, however, can be deficient, and supplementing them can give them better outcomes. None of this makes vitamin A superior to prevention by vaccination.
Tuberculosis is more common in patients with low vitamin A:
It's true that you're more likely to get tuberculosis if you're deficient in vitamin A. But, in developed countries, very few people are deficient. Tuberculosis plagues impoverished countries where many people are malnourished.
Vitamin A supplementation will not cure tuberculosis. Antibiotics, on the other hand, will. Taking vitamin A also won't make you immune to tuberculosis either, as if this would be necessary for anyone in a developed country.
Sepsis patients are deficient in vitamin C:
The sepsis caused physiological changes in their bodies, lowering vitamin C levels.[249]
>Total vitamin C, ascorbic acid, and dehydroascorbic acid concentrations in plasma of critically ill patients
Vitamin C levels lower with illness and injury.
The vitamin C didn't improve outcomes in this study.[250]
>Intravenous vitamin C administration to patients with septic shock: a pilot randomised controlled trial
Nor did it help in this study.[251]
>The relationship between vitamin C or thiamine levels and outcomes for severe sepsis patients admitted to the ICU
>For the total cohort of 235 patients, there was no statistically significant relationship between a patient’s initial ascorbic acid or thiamine level and either survival or development of shock
>The patients with septic shock had lower vitamin C concentrations and higher C-reactive protein concentrations than the non-septic patients
End quote.
This is despite receiving allegedly adequate amounts (might it be because they are not actually enough, and the authorities have lied again?):
Vitamin C levels will be the least of a sepsis patient's concerns and drinking lemonade certainly won't help them. Sepsis doesn't come on like a common cold. It usually comes from pre-existing infections which get out of control.
Vitamin D
Since vitamin D is well known to bolster immune health, and this is getting boring, I'll only focus on what is patently false.
Vitamin D cures influenza): [252]
>A colleague of mine and I have introduced vitamin D at doses that have achieved greater than 100 nmol/L in most of our patients for the past number of years, and we now see very few patients in our clinics with the flu or influenzalike illness. In those patients who do have influenza, we have treated them with the vitamin D hammer, as coined by my colleague. This is a 1-time 50 000 IU dose of vitamin D3 or 10 000 IU 3 times daily for 2 to 3 days. The results are dramatic, with complete resolution of symptoms in 48 to 72 hours. One-time doses of vitamin D at this level have been used safely and have never been shown to be toxic.8 We urgently need a study of this intervention. The cost of vitamin D is about a penny for 1000 IU, so this treatment costs less than a dollar.
This is just a random anecdote with no scientific basis. It's also not true to say that it's totally safe, there can be a risk of hypercalcemia with prolonged or repeated massive doses of vitamin D, which can lead to calcification, which can in turn cause heart problems, among other things. That wouldn't happen in the span of a couple days, but stupid people might see things like this and decide to take daily vitamin D doses exceeding the recommended daily amount which given enough time could cause serious problems.
Selenium decreases HIV viral load (yes, there is a treatment for HIV unlike what some fearmongers claim):
Yeah, it's called antiretrovirals you idiot. This is insanely dangerous and idiotic advice, seconded only by "Doctor of Herbology", Richard Schulze's advice to have some garlic if a rabid animal mauls you.
Look at the broader literature:
>Several studies investigated the role of selenium in disease progression, morbidity and mortality in HIV infected individuals. Larger studies were conducted in countries with poor economic resources and limited access to HAART. According to the majority of published studies low selenium levels appear to have an association with mortality, and selenium supplementation appears to play a beneficial role on survival or on slowing disease progression among HIV infected individuals. The role of selenium supplementation on preventing hospital admission among HIV outpatients was also noticed. The literature suggests an association between selenium deficiency and development of HIV associated cardiomyopathy and furthermore, selenium supplementation appears to improve the cardiac function in HIV infected individuals with cardiomyopathy. However, there is conflicting evidence regarding the role selenium in modifying HIV viral load and immune status in HIV infection.
>Selenium and sero-status of HIV
>The possible relationship between serum selenium levels and the sero-status of HIV has been analysed in 12 studies.18,30-40 The majority of these reported a significant association between HIV infection and low serum selenium levels.30-38 However, three studies comparing HIV-positive to HIV-negative subjects did not find a significant relationship between HIV-infection and selenium deficiency.18,39-40 It is possible that these studies failed to demonstrate a significant association due to small sample sizes39,40 and the inclusion of severely malnourished subjects in both the HIV-positive and HIV-negative study groups.18
>Selenium and HIV disease stage/disease progression
>An association between selenium levels and HIV disease stage (including CD4 cell counts, opportunistic infections, AIDS-related neoplasm and viral load) has been reported by seven authors.14-17,19-21
>Cirelli et al. measured serum selenium concentration in four groups of HIV-infected patients: symptom-free subjects, persistent generalized lymphadenopathy (PGL), AIDS related complex (ARG) and AIDS. Serum selenium concentrations were significantly higher in symptom-free HIV positive subjects as compared to the other three groups.14 Similarly, Constans et al. observed that serum levels of selenium were lower in patients with a count of CD4 less than 400 cells/mm3.15 Another study reported that opportunistic infections occurred more frequently among patients with lower serum selenium concentration.16 In a cross-sectional study on 104 HIV-infected individuals Look et al. reported that mean serum selenium levels were significantly lower in patients at CDC HIV stage II and III as compared to healthy subjects and to HIV stage I patients.17
>In addition, three clinical trials reported a slower decline in CD4 or an increase in CD4 cell counts in patients receiving oral selenium supplementation and these are briefly described below.19-21
>Burbano et al. conducted a randomized, double-blind, placebo-controlled trial on 186 HIV-infected individuals and showed that the placebo group had a more rapid decline in CD4 count than the selenium-supplemented group.19 A further randomized, double-blind, placebo-controlled supplementation trial (micronutrients + 200 µg/day of selenium) designed by McClelland et al., involving 400 pregnant HIV positive women in Kenya, showed that the selenium-supplemented group had higher CD4 levels than the placebo group.20
>Hurwitz et al. administered either supplementation with selenium (200 µg/day) or placebo to 174 HIV subjects for 9 months. At the end of the follow-up period, an higher increase in CD4 count was observed among selenium responders (individuals whose mean serum selenium concentration changed more than 3 standard deviations above the mean serum selenium concentration change of the placebo group) than that recorded in the placebo and selenium non-responder groups. Authors performed an analysis to examine if the effect on CD4 count was mediated by the viral load change. Interestingly, a model with several covariates (including HIV disease stage, antiretroviral treatment and adherence to it) confirmed that, in this study, selenium treated patients had a significant decrease in HIV viral load.21
>Seven studies did not demonstrate a significant relationship between selenium levels or supplementation and CD4 cell count or disease status.27,41-45 However, Rousseau et al. failed to find a relationship between selenium levels and CD4 cell count or disease status in a study which looked at patients treated with highly active antiretroviral therapy (HAART). This may suggest that the rapid improvement in the immune status of the patients taking anti-retroviral therapy, may be masking any effect of selenium supplementation or adequate plasma selenium levels.46
>The majority of studies that investigated for a relationship between either plasma or serum selenium concentration or selenium supplementation and plasma HIV viral load, failed to find a significant association.20,27,38,44,47 Only one supplementation trial reported that selenium-responders had slower progession of HIV viral burden than the placebo or selenium non-responders group.21
>Selenium and mortality in HIV-infected subjects
>Five studies evaluated the role of selenium on mortality in HIV-infected subjects.15,22,25,26,48
>Allavena et al. analyzed the relationship between serum selenium levels in 80 HIV seropositive patients at stage IV of infection (CDC classification) treated with zidovudine (AZT) and mortality within one year. They observed that the patients who died had significantly lower selenium values.22 In a one-year prospective study on 95 HIV positive subjects, Constans et al. found that death was significantly associated with low serum selenium levels.15 Baum et al. longitudinally evaluated 125 HIV positive intravenous drug users for 3.5 years: selenium deficiency was significantly associated with mortality.25 In another study, Campa et al. observed 24 HIV positive children, for a five-year period and found that selenium deficiency was an independent risk factor for HIV-related mortality.26
>Only one supplementation trial did not observe an effect of selenium on mortality.48
>Selenium and cardiovascular involvement in HIV-infected subjects
>Selenium seems to also play a role in the development of cardiac dysfunction among HIV-positive subjects. Two studies investigated this relationship and are described below.50,51
>Zazzo et al. prospectively evaluated the effect of selenium supplementation in 10 consecutive patients with both acquired immune deficiency syndrome (AIDS) and non-obstructive cardiomyopathy. Each patient received sodium selenite orally, 800 µg/day for 15 days and 400 µg/day for 8 days. Eight of these patients were found to have low plasma selenium levels before treatment yet six showed a return to a normal left ventricular shortening fraction within 21 days. One patient died on the 15th day of treatment and one had a thiamin deficiency.50
>Twagirumukiza et al. conducted a prospective multicenter study of 416 HIV positive Rwandan patients who were not receiving HAART and did not have a previously documented history of cardiovascular disease. Clinical examination, biochemical tests and echocardiography was carried out on all those enrolled in the study. Investigations showed that 71 (17.7%) patients had dilated cardiomyopathy and a low plasma level of selenium was significantly associated with the development of cardiomyopathy.51
>Selenium and hospital admissions in HIV infected subjects
>A randomized, double-blind, placebo-controlled study evaluated the role of selenium supplementation on preventing hospital admission in patients with HIV infection, attending outpatient clinics.19 The trial showed a decrease in total hospital admission rates, percent of hospitalization and cost for hospitalization in the selenium-receiving group compared with the placebo group.19
>Discussion
>Selenium is recognized to have an important role in both immunologic function and antioxidant defense mechanisms. Evidence suggests that oxidative stress contributes to the pathogenesis of HIV infection; in fact several studies have indicated that the apoptosis of CD4 cells contributing to HIV progression does not result solely from HIV infection, but largely from antioxidant imbalances in the host.52-54 It has been reported that selenium supplementation has a positive effect on oxidative stress in HIV-infected individuals.32 Moreover, studies show that selenium is vital to cell-mediated immunity and B-cell function.55
>According to the majority of published studies, HIV infection is associated with lower serum selenium concentration.30-38 Nutritional deficiencies are common in HIV-infected individuals56,57 and are caused by several factors: the oxidative state induced by the virus, malabsorption, altered metabolism, gut infection, altered gut barrier function, and the hypermetabolic state produced by chronic HIV infection.58-60 It has also been suggested that a possible cause of selenium depletion among HIV positive subjects is the utilization of selenium by HIV-1 virus to produce its own selenoen-zymes.61,62
>In our literature review, three studies did not find a significant relationship between blood selenium concentrations when HIV seropositive and HIV seronegative subjects were compared.18,39,40 It is interesting to note that in a study conducted by Look et al., when comparing advanced stage HIV subjects with uninfected subjects, the former group had significant lower selenium levels. Whereas there was no difference in blood selenium levels if asymptomatic HIV-positive subjects were compared with uninfected subjects.17 These findings suggest that HIV infection alone is not the sole factor involved but perhaps it is the stage of disease that has a larger impact on selenium level.
>Many authors report a significant relationship between CD4 cell count, opportunistic infections, HIV stage and selenium levels, whereas the association with HIV viral load is much more controversial.
>Regarding the role of selenium in HIV-HCV co-infection, co-infected subjects usually have a higher levels of oxidative-stress which could explain the progressive lack of endogenous antioxidants and the subsequent decrease in selenium levels. As such, infection with more than one virus may cause an higher selenium depletion.
>Data from the literature, indicates that cardiac tissue selenium levels are lower in AIDS patients with cardiomyopathy as compared to non-AIDS controls.51 Indeed, low plasma levels of selenium are associated with the development of cardiomyopathy in HIV positive individuals who are not receiving HAART.63,64 Two further studies showed an improvement of the patient’s left ventricular shortening fraction after selenium supplementation.50,65
>The role of selenium in the pathogenesis of cardiac diseases has been suggested yet. Selenium deficiency has been strongly implicated in the pathogenesis of Keshan disease, a dilated congestive cardiomyopathy endemic to certain mountainous areas of China.9,29 A similar cardiomyopathy has been described in patients on long-term total parenteral nutrition who became selenium deficient.10,56,57 In conclusion, although HAART has remarkably improved the survival of HIV-infected individuals, selenium supplementation could yet have a role in slowing the disease progression, by reducing the incidence of opportunistic infections and HIV-associated mortality. This may have a particularly useful application in patients living in countries with poor economic resources. However, it is not possible to give an exact indication on the use of selenium in clinical practice.[253]
>Selenium supplementation in HIV-infected individuals: A systematic review of randomized controlled trials
>Background & aim: HIV infection has been linked to selenium deficiency which, in turn, is thought to be associated with a high risk of tuberculosis and mortality in HIV-infected patients. Furthermore, several trials have reported the beneficial effects of selenium supplementation in patients with HIV. However, the evidence remains inconclusive. Our study aimed to investigate whether daily selenium supplementation in patients infected with HIV delays the progression of HIV infection.
>Methods: A systematic review was performed using EMBASE and Medline databases from January 2000 to June 2018. We included randomized clinical trials in adults comparing selenium with placebo and reporting outcomes including its effect on HIV viral load and cluster of differentiation 4 cell count (CD4).
>Results: Six out of the 507 retrieved articles that met the inclusion criteria were used in this review. Reviewed studies show that daily supplementation with 200 μg selenium may improve the rate of cluster of differentiation 4 (CD4) count. The length of selenium supplementation and follow-up varied from 9 to 24 months. Supplements were well tolerated in all reviewed studies. Whether daily selenium supplementation in HIV-infected persons suppresses HIV-infection requires further investigation as existing data are heterogeneous.
>Conclusions: We found some clinical evidence that selenium supplementation can delay CD4 decline in HIV-infected patients, thus prolonging the onset of AIDS. However, we did not find quantifiable evidence that selenium supplementation suppresses or reduces HIV viral load.[254]
Low selenium levels are linked to faster disease progression and worse outcomes, this is true. That's about it. Supplementing selenium is not going to cure you of HIV, nor will it make you immune to HIV. Taking selenium instead of antiretrovirals is a surefire way to die of AIDS, as is taking selenium instead of getting PEP upon exposure to HIV a surefire way to wind up with an irreversible infection. A lot of the data relating to selenium and HIV comes from impoverished parts of African countries where, shocker, people are deficient in selenium, much like vitamin A. Anti-vaxxers and disbelievers of medicine misinterpret the data, as per usual.
I really can't express how insanely idiotic it is to suggest taking fucking selenium instead of antiretrovirals which are proven to treat HIV. You might as well recommend people to stick a loaded .44 magnum up their mouth and pull the trigger. Subjects like this really show just how dangerously delusional digdeeper is.
What all of this suggests is that being deficient in vitamins lowers your immune system. Bolstering vitamin intake can ameliorate some diseases. What it does not suggest is that you are guaranteed protection against diseases, nor does it suggest that vitamins serve as a universal treatment for disease.
Good nutrition cannot guarantee protection against disease. That is where the issues arise. People will still get infected and spread the disease to others. People will die as a result. There are people that take supplements upon infection with disease and it does nothing. For more lethal diseases, some die. Developing drugs that can specifically target pathogens or vaccines that prevent infection from them is never going to be of diminished importance to nutrition. Nutrition is important but it's not an ultimate solution, as you are effectively suggesting.
Acupuncture and cupping therapy
I think digdeeper will accept anything, as long as it isn't mainstream. This article's become a joke at this point. What's next, bloodletting?
Digdeeper cited this study.[255]
>Acupuncture or cupping plus standard care versus standard care in moderate to severe COVID-19 patients: An assessor-blinded, randomized, controlled trial
Reading over the study, it seems that symptoms are self-reported, which could introduce bias. The study is also assessor-blinded, leaving the researchers and patients aware of the scope of the study, which is also a venue for bias. Putting that aside, symptoms were reduced, hospital stay was reduced, the control group had worse oxygen saturation, and the control group had a higher rate of admission to the ICU. However, nobody died. This, again, is one small scale study, which alone isn't definitive proof of anything. In the scope of this study, acupuncture doesn't prove to be a life-saving treatment.
Herbal medicine
Realistically, our immune system should deal with infections with just the basics covered. However, sometimes you need that extra boost, and herbs can provide it in a safe way (unlike medical drugs or vaccines).
Nonsense, herbs can be infected with parasites and disease-inducing pathogens. Nothing is completely safe. Medical drugs designed to target pathogens, and vaccines designed to prevent disease, are categorically more effective than herbs, which may only bolster a person's immune system prior to infection. In the context of their usage to treat disease, by being paired with human stupidity, herbs become unsafe, since they almost never effectively combat dangerous diseases. People can try to treat themselves with herbal medicine and can suffer bad outcomes as a result.
Keep in mind that for the longest time humanity has lived in the wild, being dependent on the plants growing there.
This was also the time that humans were at the mercy of their environment, and routinely died of diseases now easily treated with antibiotics.
Eating those would have given them a constant dose of thousands of bioactive phytochemicals of which some have anti-infective properties. So, just including a variety of plants in your diet is a great way to try to replicate the ancient environment to which we're adapted to. But some plants are particularly effective - and we call the usage of those herbal medicine:
Healthy foods are, well, healthy. They are good for your immune system. Assuming your diet consists largely of healthy foods, they lower your risk of developing chronic diseases. They are not, however, a cure for disease; they definitely do not nullify the significance of modern medicine, like antibiotics and other medications, or vaccines.
Definitely the King of immune supporters that can apparently kill any virus - "Almost every virus tested has not been able to withstand allicin, the active ingredient produced when a fresh clove of garlic is crushed". Here's what the Encyclopedia of Herbal Medicine says about it:
When I initially went to the article being cited, the original page was offline, and internet archive was down. So, I used the mozilla archive, but it linked to a random page about yeast. So, I checked the mozilla archive relating to Schulze, and seemingly found the page. You should fix that.
Let's look at the article.[256] I'm not going to waste time scrutinizing everything. I might quote some especially dumb stuff though.
>“Garlic can protect us from heavy metals and other toxic substances.” Cha, 1987
Garlic can potentially lower absorption and aid in the excretion of some heavy metals, but that's not exactly "protection" in the sense that the typical grifter means. It's not the same protective effect that iodine has for those exposed to nuclear fallout. Don't live life thinking that garlic will protect you from heavy metals, just avoid heavy metals. If you are poisoned, get actual treatment e.g chelation, instead of only taking garlic like a moron.
>"The Chinese use garlic to treat TB with decent results. If I feared that I had been exposed to TB, I would take at least one garlic capsule a day, and I would make sure the label said that each capsule was standardized to the equivalent of at least one gram of fresh garlic." Doctor James A. Duke PhD, Note we know also vitamin D is extremely important for TB both prevention and cure
>Some MANY years ago as a young kid knowing little about health, I came down with a serious flu like condition. I thought I was dying. Although ignorant I knew enough to stay away from "doctors". Hillbillies do learn some of the more important things in life early.
This is who you are taking health i.e _medical_ advice from, by the way.
>“One quick example of garlic's power, is in killing multi-drug resistant tuberculosis (MDR-TB), which the mainstream media has termed the "white plague," roiling the masses with a fear of drug-resistant (but not plant-extract resistant) they are made to believe they are defenseless against. Last year an article was published in a peer-reviewed scientific journal showing that garlic was capable of inhibiting a wide range of multiple drug resistant tuberculosis strains.[ii] The authors concluded "The use of garlic against MDR-TB may be of great importance regarding public health." 5 Food-Medicines That Could Possibly Save Your Life
Multi-drug resistant tuberculosis is not immune to all drugs, just like antibiotic-resistant bacteria are not immune to all antibiotics. It's merely harder to treat, other drugs have to be administered. Those other drugs will cure you. Garlic won't.
>“Almost every virus tested has not been able to withstand allicin, the active ingredient produced when a fresh clove of garlic is crushed.” Planta Medica 58:417–23, 1992
What does this really mean though? Is it killing viruses in vivo?
Here's the study: [257]
>In Vitro Virucidal Effects of Allium sativum (Garlic) Extract and Compounds
Of course, as I expected, in vitro. I suppose they will be using unrealistically high doses of allicin.
>Activity was determined against selected viruses including, herpes simplex virus type 1, herpes simplex virus type 2, parainfluenza virus type 3, vaccinia virus, vesicular stomatitis virus, and human rhino virus type 2
This is six select viruses, a far cry from all viruses, and garlic killing "any virus". The more severe pathogens here are vaccinia virus (smallpox) and vesicular stomatitis virus.
>However, [vaccinia virus], which is also a DNA virus, but which has a more complex envelope than either HSV-1 or 2, was only slightly susceptible to inactivation by allicin
>Finally, results of this study suggest that the activity of both fresh garlic extract and allicin against viruses rested exclusively in their direct virucidal properties and not in any intracellular antiviral mechanism
The levels of exposure and concentration of allicin cited in the study are higher than what is achievable through dietary consumption. When eating garlic, the garlic you eat will not contain enough allicin when spread throughout your system to produce the same effects seen in this study, nor will your body absorb enough allicin and get it into your bloodstream to begin with, nor will metabolize the allicin and distribute it quickly enough to see the same effects. This is an in vitro study.
Could garlic have some properties as a disinfectant of sorts? Maybe. That doesn't make it a cure for smallpox and rabies. Does garlic have some effects in treating mild illnesses, like the common cold, and sinus infections? Yeah. Those diseases don't typically lead to ARDS, or rabies, or smallpox, though. Let's try to not be raving lunatics with how we approach illnesses and things like garlic.
Moving on...
>Garlic has always been esteemed for its healing powers, and before the development of antibiotics it was a treatment for all manner of infections, from tuberculosis to typhoid.
I don't know how anyone can read this segment of the article without bursting out laughing. Garlic was used prior to the advent of ANTIBIOTICS, and was not a reliable, effective treatment. This was back in the day when people regularly died of these diseases which are now treatable with antibiotics. I almost can't believe that I used to be a part of this community.
>Renowned herbalist Richard Schulze (who ran a clinic for decades, curing all kinds of allegedly incurable diseases) heavily praises garlic:
>Garlic destroys many types of bacteria including ... Tuberculosis, Tetanus
>Garlic has been tested against many viruses and is known to destroy on contact the viruses that cause ... Rabies
All of this is said without any basis whatsoever, and so I could just discard this entirely, but for the sake of discussion, I'll give them the benefit of the doubt and assume that garlic could kill _some_ (keyword: some, not all), bacteria and viruses on external surfaces, maybe even internally.
Let's return to what I was saying before.
Rabies is a very delicate virus, which dies upon exposure to things like sunlight, heat, and air. It can only survive in saliva and nerve cells. Bleach kills rabies. Should you drink bleach if you've been bit by a rabid animal? Obviously not. The same can be said for the bacteria that cause tuberculosis and tetanus. This is a completely meaningless point for the supposed effectiveness of garlic.
Garlic isn't going to be a reliable disinfectant for these pathogens either. It might kill some of the bacteria or virus, but not enough, unlike bleach.
Unless Schulze is shilling some kind of garlic disinfectant spray which happens to kill rabies, tetanus, and tuberculosis, just like most other disinfectants, this can't be anything other than a tacit suggestion to take garlic if you've been exposed to these pathogens.
There's only been a couple dozen documented survivors of rabies, less than 30-40 globally, most of whom suffer from debilitating long-term neurological sequelae, out of the tens of thousands of people who die from it annually, and the people who have been dying from it for eons. Statistically speaking, some of those people who died probably ate garlic during the virus' very long incubation period, yet it didn't save them.
Tetanus has a lower mortality rate when compared to rabies. The mortality rate is around 10-20% in developed countries. This is, of course, still a very high risk of death, and the numbers do not give any insight into the brutality of the disease. Tetanic muscle spasms can be so forceful as to cause people to tear muscles and break bones.
Here are some videos of people with tetanus.[258][259][260]
You don't want tetanus.
Schulze is a psychotic crank shilling snake oil to people through his website.[261]
Here we go, right off the front page, a catalog of untested formulas that he's selling to people.[262] I don't see any citations to material proving the effectiveness of his products. I don't see any disinfectants either, only stuff meant to be consumed, so, I guess he is tacitly suggesting people to have some garlic if they've been exposed to rabies or tetanus.
He lures people in with his "Doctorate of Herbology", which is not a real academic qualification, but some phony qualification he obtained from a phony institution.
It seems all he has to offer people is personal anecdotes of his miracle cures in action, and not much in terms of concrete evidence.
Much like the critical thinker he is, digdeeper blindly accepts Schulze and his snake oil, and doesn't come close to applying the same standards to Schulze and his bullshit as he does to the COVID vaccines. Who cares if the products are untested, who cares if we don't know what kinds of potential contaminants could be in them?
Page 32-33 of his catalog gave me a laugh: [262]
>Ascorbic acid is a synthetic chemical and is never used in our products
As it displays a skull and crossbones around some ascorbic acid.
Ascorbic acid is just the chemical name for vitamin C. Be it synthetically-produced, like in a lab, or naturally-occurring, like in a lemon, the chemicals are identical. Ascorbic acid is ascorbic acid, much like water is water, whether it falls from the sky, or is made by reacting hydrogen with oxygen in a tube. The only caveat might be in toxic impurities present in lab-synthesized ascorbic acid, if this should be a threat. Bear in mind, fruits can also contain toxic chemicals from pollution.
>Synthetic Vitamin C, or ascorbic acid, is not found in nature and is not a food. It is a synthetic chemical created in a laboratory from sugar mutated with extremely harsh and powerful toxic substances, like nail polish remover and chlorine bleach. It is a dead, toxic chemical.
This is total nonsense.
Ascorbic acid is vitamin C and it is found in nature e.g lemons, oranges. Furthermore, vitamin C is not a food. It's a vitamin. Vitamins aren't foods.
Synthetic ascorbic acid is not "mutated". That's a biological term that when considered in the context of the collective consciousness has negative implications, often being associated with viruses and cancers, which Schulze, a grifter, I'm sure is aware of, and is deliberately using to characterize synthetic ascorbic acid as harmful, dangerous.
In my experience, nail polish remover is a reference to acetone. Acetone isn't used in the production of ascorbic acid. Also, your own body produces acetone. People undergoing ketogenesis produce a fair amount of it. This is just something Schulze is making up, and doesn't matter anyway, since acetone is not inherently harmful.
Sodium hypochlorite is also not used. And even if it was, it could be extracted.
I might as well say that big chemical companies are selling people the lethal injection as a sodium replacement, because potassium chloride is sold as a replacement for table salt.
>Most well-known research about Vitamin C's amazing healing and health benefits was NOT done using ascorbic acid but instead using natural foods rich in Vitamin C. Don't be misled! The benefits of NATURAL Vitamin C are not supported by chemical ascorbic acid.
"Natural" vitamin C is a chemical. Everything is chemical, dumb fuck. You're made of chemicals. Water (dihydrogen monoxide) is a chemical.
This is why we don't take advice from inbred hicks who think they know more than doctors who had to spend years in university studying medicine.
His statement that "most research uses 'natural' vitamin C" is a meaningless value judgement since the chemicals are the same, synthetic or naturally occurring. It's a patently false claim anyway, a lot of research uses synthetic vitamin C. I'm not going to waste my time analyzing "most" research to formally refute him, because it would be a massive effort, outside the scope of this article. He himself made no effort to back up his claim, to begin with.
This Schulze guy is a joke, and digdeeper taking him seriously speaks to his gullibility. But, digdeeper also thinks Miles Mathis, some idiot who thinks pi = 4, is someone to be taken seriously, so the standards are already at the bottom of the Mariana Trench.
UPDATE October 2023: was somehow compelled to try to seek scientific evidence for garlic's effectiveness specifically against COVID. Turns out, it does exist: [263]
>And so, the same WHO that made an image mocking garlic in particular, is made to eat crow
The WHO image in question: [264]
>Can eating garlic help prevent infection with [COVID]
>Garlic is a healthy food that may have some antimicrobial properties. However there is no evidence from the current outbreak that eating garlic has protected people from [COVID]
The study you just cited has no pertinence to this image. The WHO said that there's no evidence garlic has prevented people from contracting COVID, to which, you cited a study of people already infected with COVID, some of whom took garlic, which potentially alleviated their symptoms. These people were already infected to begin with. The study didn't concern the effectiveness of garlic in protecting people from COVID in the sense of preventing COVID, but in alleviating symptoms. This is very poor reading comprehension on your part.
"May have" when the amount of evidence is massive (versus zero for their useless measures). Ha ha ha.
A complete reversal of the reality. There's a massive evidence base for the effectiveness of vaccines, and only misinterpreted studies when it comes to herbal medicine.
Pandemic-related deaths
I kept this one for later because I felt it was a generally weak section on its own, seeing as I already nullified the supposed international conspiracy angle.
Kary Mullis
Kary Mullis - as mentioned before - invented the PCR test. He was also clear on the fact that it cannot be used to diagnose disease - and it was used exactly for that during the "pandemic".
It was used to track the spread of disease, and often combined with qualitative observations to make diagnoses.
Here's what Mullis supposedly said, according to the article you cited:[265]
>I don’t think you can misuse PCR. [It is] the results; the interpretation of it. If they can find this virus in you at all – and with PCR, if you do it well, you can find almost anything in anybody.”
>It starts making you believe in the sort of Buddhist notion that everything is contained in everything else. If you can amplify one single molecule up to something you can really measure, which PCR can do, then there is just very few molecules that you don’t have at least one single one of in your body.”
>That could be thought of as a misuse: to claim that it [a PCR test] is meaningful. It tells you something about nature and what is there. To test for that one thing and say it has a special meaning is, I think, the problem. The measurement for it is not exact; it is not as good as the measurement for apples. The tests are based on things that are invisible and the results are inferred in a sense. It allows you to take a miniscule amount of anything and make it measureable and then talk about it.”
>PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.”-
Nothing all that radical, in my opinion.
He had a history of criticizing various mainstream narratives - such as the ones about climate change or HIV / AIDS- and surely would not have let slide the COVID one, especially when the misuse of his invention was at the center of it. Unfortunately, he won't get to say anything as he died from pneumonia in August 2019, right before the "pandemic" started. The fearmongers could not have pushed the "pandemic" through if Kary was alive when it began. Therefore he had to be eliminated, and pneumonia can be induced by drugs.
So, in the context of this article, since we're not weighing the value of Mullis' life as a human being but only his value as a conspiracist, one less dumbass to spew lies during a crisis.
You're baselessly asserting that he was assassinated. The guy invented PCR testing, had stupid beliefs regarding AIDS and climate change, which he was criticized for, and died of pneumonia. You, a conspiracist, feel that the elites silenced him. I don't.
pneumonia can be induced by drugs
The article you cited: [266]
>Drug can cause various types of lung damages, with drug-induced pneumonitis (including acute interstitial pneumonia, usual interstitial pneumonia, desquamative interstitial pneumonia, nonspecific interstitial pneumonia, bronchiolitis obliterans with organizing pneumonia, eosinophilic pneumonia and hypersensitivity pneumonitis) being the most important among them. The incidence and the causative agents of drug induced pneumonitis have varied over time. Before 1980, anticancer agents and gold salts were the main drugs, and the number of causative drugs (61) and case reports was small. Recently, pneumonitis has increasingly been caused by Chinese herbal medicines, antibiotics, chemotherapy agents, anti-inflammatory drugs, analgesics, cytokines, and gold salts, and the number of case reports and drugs involved (177) has increased. Drug-induced pneumonitis has characteristics that depend on the causative agent. Review of our patients and reports in Japan revealed the following. Pneumonitis caused by anti-inflammatory drugs, analgesics, and antibiotics generally develops at 1-2 weeks after starting administration, and bronchoalveolar lavage and histologic examination of lung biopsies reveals the features of eosinophilic pneumonia. Such pneumonitis is associated with a high frequency of a positive drug lymphocyte stimulation test (DLST), and has a good outcome. Conversely, with pneumonitis caused by anticancer and immunosuppressive agents, the onset is often delayed and the disease has features of diffuse interstitial pneumonia and pulmonary fibrosis. The frequency of a positive DLST is low, and the outcome is generally poor. Pneumonitis induced by Chinese herbal medicines, gold salts, and antituberculosis agents has intermediate features between the above two types :i.e., it develops after 2-3 months or six months (gold salts), and resembles either eosinophilic pneumonia, BOOP or interstitial pneumonia. For in vitro identification of causative drugs, the DLST and the leukocyte migration inhibition test (LMIT) are generally used. The latter test is superior in sensitivity, suggesting that the mechanism of this test involves cytokines such as IL-1 alpha, IL-1 beta, IL-2, TNF-alpha, and IL-8.
Pneumonitis is not pneumonia. Pneumonitis is an inflammation of the lungs. This could lead to infection, and pneumonia.
Drug induced pneumonitis is characteristic of prolonged usage of specific drugs, typically at high dosages, in addition to old age, pre-existing health conditions, and things like a history of smoking or genetic predisposition to be harmed by certain drugs. The main component is prolonged usage, and/or high dosages of specific drugs. Discontinuing administration of the drug typically alleviates symptoms.
It's not as though there is a pneumonia drug that you can slip into someone's drink to give them pneumonia. Drug-induced pneumonitis is just a condition that arises from lung damage caused by what is usually prolonged, high dosages of certain drugs. Antibiotics, chemotherapies, and other treatments, can cause it.
Pneumonitis can be diagnosed through blood tests, bronchoscopy, X-rays and CT scans, lung biopsies, and lung function tests such as spirometry and oximetry. I'm sure the hospitals in Mullis' vicinity were capable of these diagnostics.
Did Kary Mullis' death fit into the context of drug-induced pneumonitis?
Here's some case reports I found online:
Case #1 [267]
>We report the case of a 45-year-old male who developed fever and cough, and progressed to hypersensitivity syndrome related to drug-induced pneumonia following moxifloxacin therapy. Discontinuation of moxifloxacin led to resolution of fever with significant resolution of pulmonary lesions.
>Moxifloxacin is a fluoroquinolone antibiotic widely used for respiratory tract infections (10). It exerts antimicrobial effects by inhibiting DNA gyrase in Gram-negative bacteria and topoisomerase IV in Gram-positive bacteria, resulting in DNA cleavage and rapid bactericidal activity (11). Although fluoroquinolones are generally regarded as having a favorable safety profile, they are associated with a non-negligible incidence of adverse effects. Common adverse reactions to moxifloxacin include QT interval prolongation (12), hepatic and renal dysfunction, mental behavioral abnormalities, gastrointestinal, central nervous system, and skin reactions (13). Rare side effects such as recurrent tendonitis (14), interstitial nephritis (15), and allergic-like reactions, bilateral acute iridocyclitis (16), and cardiotoxicity have also been reported. Despite these known risks, moxifloxacin-induced pneumonia remains scarcely reported
>A 45-year-old male patient was admitted with a persistent cough of over 10 days. He had no history of hypertension, diabetes, smoking, or alcohol consumption. The patient experienced paroxysmal coughing for over 10 days after catching a cold, with exacerbated symptoms at night, producing a small amount of sticky white sputum that was difficult to expectorate. He did not present with chills, high fever, purulent sputum, night sweats, chest pain, hemoptysis, or respiratory distress. Hospitalization at the local hospital revealed mild lung infection on chest CT (Figures 1A,B) and no significant abnormalities in the complete blood count and renal and liver function tests. He was then treated with moxifloxacin 400 mg IV daily, however, five days later, he developed fever, with a maximum body temperature of 39.6°C, without apparent chills or shivering. Moxifloxacin was discontinued, and the antibiotic was changed to piperacillin-tazobactam sodium 4.5 g IV q8h. Post-antibiotic treatment, a follow-up chest CT revealed infective lesions in the right upper lobe and bilateral lower lobes that were significantly more extensive than before (Figures 1C,D). The patient came to our hospital for further treatment, upon admission, laboratory investigations showed a C-reactive protein (CRP) of 82.9 mg/L and WBC count of 4.5 × 109/L, with a neutrophilic count of 2.4 × 109/L. He was once again administered moxifloxacin 400 mg IV daily for the infection and underwent a bronchoscopy examination 3 days later, yielding no significant findings. Bronchopulmonary biopsy was performed on the posterior segment of the upper right lobe, and pathology revealed chronic inflammation with fibrous tissue hyperplasia (Figure 2). Both the Periodic Acid-Schiff staining and Cytomegalovirus (CMV) tests were negative. During this period, his cough and sputum improved, and his CRP reduced to 6.8 mg/L. However, on the 6th day of admission, the patient developed a fever with a body temperature of 38°C, without chills, shivering, runny nose, sneezing or other symptoms. The lavage Metagenomic next-generation sequencing did not reveal significant bacteria, viruses, or mycobacterium tuberculosis. Symptomatic treatment was administered, and a repeat CRP measurement recorded 114.2 mg/L. The blood routine test showed a WBC count of 4.57 × 109/L, with a neutrophil count of 3.48 × 109/L and a normal eosinophil count (0.3×109/L), with no observed rash. The patient was given piperacillin-tazobactam sodium 4.5 g IV q8h for the infection; however, the fever persisted, and his cough and sputum worsened, with shortness of breath during fever. Acyclovir (0.25 g IV daily) antiviral treatment was added for 3 days, and a follow-up chest CT on the 9th day of hospitalization revealed scattered nodular lesions, ground-glass opacity, and interlobular septal thickening in both lungs (Figures 1E,F). The results of the antinuclear antibody spectrum and anti-neutrophil antibody testing were negative. Moxifloxacin was discontinued on the 10th day of hospitalization, after which the patient remained afebrile and his cough improved. Two days later (January 17, 2022), methylprednisolone 40 mg daily was added for anti-inflammatory treatment, and a follow-up chest CT on the 17th day of hospitalization showed significant resolution and improvement of the lung lesions. Upon discharge, the patient continued to take oral Prednisone 30 mg daily, with a weekly reduction of 5 mg. A follow-up chest CT 1 month later showed complete resolution of the lesions (Figures 1G,H), with no significant coughing or sputum symptoms. During the hospitalization period, the patient took compound licorice oral liquid for cough relief (the patient had used it previously without adverse reactions), with no other special medications.
Case #2 [268]
>INTRODUCTION: Drug-induced pneumonitis is a well-established complication of cancer therapies, and its presence can serve as a negative prognostic factor in patients who develop signs of lung dysfunction. Drug-induced pneumonitis is often difficult to diagnose and is considered a diagnosis of exclusion.
>CASE PRESENTATION: A 62-year-old female with a past medical history of breast cancer (ER/PR+, HER2-) with metastasis to liver, bone and pleura that was refractory to chemotherapy and prior endocrine therapies was admitted for acute hypoxic respiratory failure requiring O2 supplementation with high flow nasal cannula. Her admission chest computed tomography (CT) was consistent with diffuse ground-glass opacities (GGOs) most concerning for infection vs acute pneumonitis. She had a prior history of CTACE grade 4 Palbociclib induced pneumonitis a year ago, that responded completely to steroids. Two weeks prior to this admission, her oncologic regimen had been changed to Sacituzumab (Trop-2 directed antibody and topoisomerase inhibitor drug conjugate). The infectious work-up was negative including a negative bronchioalveolar lavage (BAL) with cell count showing normal differential. Transbronchial biopsies were significant for mild alveolar septal inflammatory cell infiltration with occasional eosinophils. Given these findings, CTCAE grade 4 drug-induced pneumonitis was suspected. She was treated with prednisone 60 mg daily (1mg/kg) and progressed well clinically. A steroid taper was continued for one month, and oxygen requirements continued to improve. Repeat CT chest imaging showed complete resolution of pneumonitis. Due to lack of treatment options, the patient was rechallenged with Sacituzumab under close observation and continues to show good response without any recurrence of pneumonitis.
Case #3 (actually contains two cases) [269]
>Two Cases of Amivantamab-Induced Pneumonitis in Patients With NSCLC: Case Report
>Case 1
>A 57-year-old male individual who had never smoked was diagnosed with stage IVB EGFR exon 19 deletion lung adenocarcinoma. At diagnosis, sites of malignancy included the right middle lung and right pleura. The patient wished to avoid chemotherapy if possible. The patient started osimertinib, but after nine months he experienced a worsening right pleural effusion. Repeat Tempus xT testing of the right pleural fluid revealed EGFR exon 19 deletion (65%), TP53 C135F (57.3%), CCNE1 amplification, tumor mutational burden 3.2 mutations per megabase (thirty-fifth percentile), MET overexpression, CCNE1 overexpression, and ERBB3 overexpression. Subsequently, bevacizumab was added with continued osimertinib. After another four months, imaging revealed increased right pleural nodularity and an enlarging right pleural effusion. Given disease progression and preserved EGFR exon 19 deletion and MET overexpression, tepotinib was added with continued osimertinib. After one year, the patient experienced worsening right pleural metastases.
>The patient remained averse to cytotoxic chemotherapy, and amivantamab was initiated with the continuation of osimertinib. He experienced a grade 2 infusion-related reaction with amivantamab initiation that did not recur with subsequent infusions. Palliative radiation was administered to the right flank one week after the first amivantamab dose. One day later, he presented to the hospital with acute hypoxic respiratory failure. Chest angiography revealed acute pulmonary emboli and extensive bilateral ground glass opacities (Fig. 1). Lovenox and EKOS catheters were used for pulmonary emboli, and broad management with empirical antibiotics, diuretics, and high-dose corticosteroids was initiated. The infectious workup was negative. After several days, no clinical improvement was observed. Suspicion was highest for both amivantamab-related DI- ILD and disease progression contributing to respiratory failure. Ultimately, the patient and family decided to withdraw life-sustaining treatment after 1.5 weeks in the intensive care unit, and the patient died shortly after.
>Case 2
>A 50-year-old female individual who had never smoked was diagnosed with stage IVB EGFR exon 19 deletion lung adenocarcinoma. At diagnosis, sites of malignancy included a right suprahilar mass with mediastinal invasion, osseous metastases with soft tissue extension, and right adrenal gland metastasis. Before molecular testing resulted, the patient was hospitalized for pulmonary infarction of the right upper lobe, right pleural effusion, and pathologic vertebral fracture. While hospitalized, circulating tumor DNA re- sults revealed an EGFR exon 19 deletion. Osimertinib was started and she underwent palliative radiation of bone metastases.
>Her metastatic disease was stable for one year, at which point imaging revealed recurrent cancer in the right upper lobe with adjacent mediastinal lymphade- nopathy. Carboplatin and pemetrexed were initiated with continued osimertinib. Nevertheless, weeks later, she was hospitalized with post-obstructive lung empy- ema complicated by pulmonary emboli. Tempus xF circulating tumor DNA testing revealed EGFR exon 19 deletion (35.4%), MET copy gain, TP53 splice variant (6.5%), and EGFR copy gain. Because of the infectious complication from platinum doublet, the patient preferred to avoid further chemotherapy. Tepotinib was initiated with continued osimertinib.
>Unfortunately, tepotinib was discontinued owing to intolerable gastrointestinal side effects after two months and disease progression occurred one month later. Capmatinib was initiated with continued osimertinib but was only tolerated for two weeks. Amivantamab was subsequently initiated with continued osimertinib. The patient experienced a grade 1 infusion-related reaction with the initial dose which did not recur with subsequent infusions. She tolerated amivantamab ther- apy for one month. Nevertheless, she then presented with acute hypoxic respiratory failure. Imaging revealed diffuse bilateral ground-glass opacities and pericardial effusion (Fig. 2). High-dose intravenous methyl- prednisone, diuretics, and empirical antibiotics were initiated; nevertheless, her respiratory status continually declined. The patient ultimately transitioned to hospice and died after a three-week hospitalization.
Case #4 [270]
>A 66-year-old never-smoker female patient was treated for MAC-PD with RFP, EB, and CAM. Despite multidrug therapy for more than five years, her sputum culture remained positive. Recently, a drug susceptibility test of sputum revealed the resistance to CAM (minimum inhibitory concentration of >64 μg/ml), and thus, ALIS therapy was added to the standard treatment for refractory MAC-PD. However, two weeks after starting ALIS therapy, she presented to our hospital complaining of fever, fatigue, and
Case #5 [271]
>Section snippets
>Case report
>A 74-year-old Japanese woman had been treated with clarithromycin (800mg), faropenem (600mg), ethambutol (500mg), and sitafloxacin (200mg) for the treatment of M. avium and M. massiliense co-infection. ALIS was added to these agents because of the refractory nature of the infection. The patient was diagnosed with non-tuberculous mycobacterial pulmonary disease three years before initiating ALIS, and treatment was started simultaneously. She had a history of intravenous amikacin (AMK) treatment
>Discussion
>We reported the case of a 74-year-old woman with drug-induced organizing pneumonia due to ALIS treatment that was diagnosed based on chest CT imaging and histopathological findings. Discontinuing ALIS therapy and changing to intravenous AMK improved her symptoms and chest CT findings. Intravenous AMK did not affect the clinical course of organizing pneumonia.
I can't find much on Mullis' death besides the fact that he died at home of pneumonia, so I can't entirely compare his case to these people's. Overall, dying at home of pneumonia doesn't sound much like being a cancer patient getting repeated treatments of chemotherapy.
To die like he did, Mullis would probably have to be drip-fed some drug that could induce pneumonia. Bear in mind, it would be a drug that _could_ induce pneumonia. Drug-induced pneumonitis is a relatively rare condition. There's not some drug that will absolutely induce it in a person. You're better off poisoning somebody, if you want to kill them.
Was Kary Mullis having his pneumonia treated and monitored by doctors? If so, they could've picked up on the drug-induced pneumonitis and intervened. Was there an autopsy conducted on Mullis' corpse? I don't know. I can't find anything. You seem to be interested though, so maybe you could bolster this weak spot.
In the New York Times report on his death, his wife said his death was caused by heart and respiratory failure, inflicted by pneumonia.[272]
>Kary B. Mullis, a biochemist who won the 1993 Nobel Prize in Chemistry for discovering a way to analyze DNA easily and cheaply and thus pave the way for major advances in medical diagnostics, molecular biology and forensic science, died on Aug. 7 at his home in Newport Beach, Calif. He was 74.The cause was heart and respiratory failure brought on by pneumonia, his wife, Nancy Cosgrove Mullis, said.
For her to say this sounds like there was an autopsy of sorts.
What did Kary Mullis' family think of his death? Are they suspicious? I haven't seen anything to suggest suspicion from them.
Overall, this an almost-completely baseless assertion. "Maybe it was drug-induced pneumonia", says the person who didn't even read the article they cited about drug-induced pneumonitis. "You can't prove me wrong, therefore this is a theory worth considering."
Jovenel Moïse
Digdeeper presents his ahistoric, made-up telling of history:
The president of Haiti, who refused the donation of 756 000 vials of AstraZeneca's COVID non-vaccine in April 2021, and was killed 3 months later:
“An unidentified group of individuals, some of whom were speaking in Spanish, attacked the private residence of the President of the Republic and mortally wounded him,”
A week after the killing, his country received a "gift" of 500 000 vials of the poison. This situation is unique in that we have clear proof that he was actually murdered. Totally unrelated to his rejection of the vaccines though, I'm sure.
What actually happened:
Moïse rejected AstraZeneca vaccines on the basis of vaccine safety and logistics, asking for any other COVID vaccine instead, but later, around February 2021 (5 months before his death) agreed to receive a shipment of 860k vaccines through COVAX. This webpage documents the scheduled shipment in February, months prior to his death.[273] Here is the shipment schedule on internet archive, dated 3 February 2021, months prior to Moïse's death.[274]
The articles that I am going to present document that the government was not categorically refusing any and all vaccines. We'll start with factcheck.afp, which I'm sure digdeeper will hate for its name. They document that the government wanted any vaccine other than AstraZeneca, like Moderna or J&J.[275]
>By February 2021, the COVAX vaccine distribution scheme had allocated 876,000 vaccine doses to reach Haiti, but this was delayed due to manufacturing issues in India.
>According to the statement, Haitian health minister Greta Roy Clément confirmed that she had written to the Gavi Alliance (Global Alliance for Vaccines and Immunisation) to reject the WHO donation of AstraZeneca vaccines. She asked for it to be replaced with another vaccine more suited to the country, such as Moderna, or the Janssen vaccine by Johnson & Johnson.
This finding is upheld by an article from opendemocracy.[276]
>Instead, Haiti asked for any other drugmaker’s vaccine – an impractical request because the country lacks a national ‘ultra-cold chain’, which limits the choice to AstraZeneca or the Johnson & Johnson vaccine, neither of which need to be stored at extremely low temperatures.
It is also upheld by haitilibre.com.[277]
>Haiti - Health : The Minister of Health wants another vaccine than AstraZeneca
>10/04/2021 11:35:41
>Following the announcement on April 6 in the media of Haiti's refusal to accept a donation of 756,000 doses of AstraZeneca vaccine proposed by the World Health Organization (WHO) via the Covax mechanism, https://www.haitilibre.com/en/news-33423-haiti-flash-haiti-refuses-a-donation-of-756-000-doses-of-the-who-astrazeneca-vaccine.html Lauré Adrien the Director General of the Ministry of Health declared "This is false, Haiti has not rejected any vaccine" while admitting that the authorities were analyzing the best option to immunize the population, taking into account the peculiarities of Haiti.
>However, Wednesday April 7, during the Council of Government, the Minister of Health, Greta Roy Clément, confirmed to the Ministers and to the Prime Minister Jouthe, to have written to the Gavi Alliance (global alliance for vaccines and immunization) in order to reject the WHO donation of AstraZeneca vaccines and ask them to replace this with another vaccine more suited to the country, mentioning that there are other vaccines citing the Janssen vaccine (Ad26.COV2.S) by Johnson & Johnson, or that of Moderna...
>At the origin of this refusal, about ten cases of thrombosis (out of more than 20 million injections) which would be linked to the AstraZeneca vaccine but whose link with the vaccine has not been formally demonstrated.
>It should be noted that the Johnson & Johnson vaccine favored by Haiti (a single injection and storage at temperatures that do not require a special freezer and also the most expensive of the vaccines) is not immune to adverse effects. The European Medicines Agency (EMA) announced on Friday the launch of an in-depth study on this vaccine produced by the American group after 4 suspected cases of thrombosis, including one fatal, in the United States (the vaccine produced by Johnson & Johnson is designed on the same principle as the AstraZeneca serum).
Here is haitilibre's previous reporting.[278]
>07/04/2021 09:43:56
>Haiti - FLASH : Haiti refuses a donation of 756,000 doses of the WHO AstraZeneca vaccine
>Haiti, refused a donation of 756,000 doses of AstraZeneca vaccine proposed by the World Health Organization (WHO) via the Covax mechanism, reported Tuesday April 6, according to the Spanish news agency EFE who quotes a high-ranking source requesting the anonymity within the Haitian Government.
>According to this source the Haitian Government refused to receive the AstraZeneca vaccine, manufactured under license by "Serum Institute of India" because of "the global unrest surrounding this vaccine", considering that the population of Haiti "would not accept it".
>The Haitian authorities have asked the WHO to send vaccines from other laboratories to Haiti, including the vaccine from Johnson & Johnson laboratories which requires only one injection and which can be stored at temperatures between 2 and 8 degrees Celsius. But the World Health Organization is "reluctant" to accept Haiti's demands, reminding Haitian authorities that "the deadlines are running out".
Moïse and his government did not initially accept the AstraZeneca vaccines, due to concerns about their safety, and logistics. But, they did not categorically reject the vaccines. They were willing to accept the Johnson & Johnson vaccines (which had safety issues as well), or other vaccines like the Moderna vaccines.
You've omitted the evidence showing his government's willingness to accept vaccines, and ultimate acceptance of the AstraZeneca vaccines months prior to his death, creating an ahistoric image of a man who staunchly rejected the vaccines, and was possibly killed because of it.
Do you, internet conspiracy guy who thinks the Moon landing was faked, really want to delve into a discussion on the politics of Haiti, and how they relate to Moïse's assassination? You don't have the literacy to do this.
So far, some of the suspects in Moïse's assassination have been identified, but nothing about COVID vaccines involving the conspiracy to kill him have been discovered yet.
John Magufuli
It's true that he spread lots of misinformation about COVID.
He went missing on February 27, 2021:
Meaning, he disappeared from the public eye.
He finally died on March 17:
Dying specifically of a chronic heart condition he suffered.
This was just a little over a month after The Guardian called to "rein in" the president. But remember that he has gone "missing" (likely captured) much earlier - less than 3 weeks after the unfortunate article.
Are you alleging that The Guardian had him whacked? You're also alleging that he was abducted. The president of a country was abducted in total silence, without anyone raising the alarm? On what basis is this being alleged? No basis, obviously. Just another baseless assertion. The elites abducted a country's president, and none of his advisors, or subordinates asked any questions about it, or even wondered where he was. They then silently returned him to a hospital, to die, after poisoning him.
The new president predictably did a 180 in terms of the COVID response:
He was then replaced by a new president who was smarter than him.
Therefore, it was actually an assassination.
Or, alternatively, he died of a heart condition that he was known to have suffered from for years, and in his final years spread a lot of misinformation.
The CIA has a heart attack gun. Why would you conduct a weeks-long operation to kill someone when you can just shoot them with a virtually untraceable toxin and have them die within a couple hours to days? I don't know.
Moving on...
Pierre Nkurunziza
Burundi's president died from a heart attack on June 8, 2020:
Mr. Nkurunziza, 55, had shown no sign of illness until he was admitted to hospital in the town of Karuzi on Saturday. After appearing to recover on Sunday, his health worsened “to very great surprise” on Monday and he could not be revived, despite several hours of effort, a government statement said.
Recovering, then suddenly getting worse and dying. Nothing suspicious here /s. He didn't care to have any kind of COVID restrictions:
Burundi was one of the few countries worldwide that refused to ban sports events or take other restrictive measures. It also allowed mass campaign rallies of tens of thousands of people during the election campaign last month. Face masks were rarely seen.
And kicked out "experts" from the WHO:
Four experts from the World Health Organization, who had reportedly questioned the government’s response to the pandemic, were expelled from Burundi last month.
Not even a month later, the new president did a 180 about COVID (of course):
While swearing in his new cabinet on 30 June, President Ndayishimiye declared the pandemic would be “the biggest enemy of Burundians.”
Funnily enough, Burundi still has only 38 COVID deaths (December 2022). Truly the biggest enemy, this COVID. Despite the extremely low COVID death rate in Burundi, Western media jumped to claim that Nkurunziza was one of the few people to have died from COVID (it would mean he was literally the first COVID death there - how likely is that?!).
This is a really weak argument. Burundi is a tattered third world country with an ineffective healthcare system. They did not have the resources to track COVID, so their low COVID death count shouldn't be much of a surprise. The government also, as you say, wasn't taking it seriously to begin with.
Nkurunziza seemingly died of heart failure. Reuters reported the following: [279]
>It was unclear exactly when Nkurunziza died. The government statement said the president, a keen sports enthusiast often photographed playing football, watched a game of volleyball on Saturday but fell ill that night and was taken to hospital in Karuzi in central Burundi.
>His health improved on Sunday but "surprisingly, on morning of Monday June 8, 2020, his health suddenly deteriorated and he had a heart attack".
>Doctors provided "cardiopulmonary resuscitation" for hours but were unable to save him.
The BBC's reporting was largely the same.[280]
>He was admitted to hospital on Saturday after feeling unwell, his condition improved but on Monday he had a cardiac arrest and efforts to revive him were unsuccessful, officials say.
>The official statement announcing the president's death said he was taken ill in the evening after helping out at a volleyball match in Ngozi, northern Burundi, on Saturday.
>He went to hospital, but appeared to be recovering on Sunday and was able to communicate with the people surrounding him, the government says.
>His condition, however, rapidly changed on Monday.
As was The Africa Report's reporting.[281]
>The government of Burundi announced on Tuesday the “unexpected death” of Pierre Nkurunziza, outgoing president of Burundi, who died on Monday 8 June at the Fiftieth Anniversary Hospital in Karuzi, following a “cardiac arrest”.
And AP News'.[282]
>NAIROBI, Kenya (AP) — Burundi’s President Pierre Nkurunziza has died of a heart attack at age 56, the government announced Tuesday, ending a 15-year-rule marked by deadly political violence and a historic withdrawal from the International Criminal Court.
>The statement posted on social media said the president was admitted to a hospital overnight Saturday after not feeling well. He appeared better Sunday but “to very great surprise” his health abruptly worsened Monday morning, and several hours of effort failed to revive him.
Nkurunziza died months before the COVID vaccines were ever released. Are you saying that he was killed solely because he had a lax approach to COVID? Why then wasn't anyone in Sweden killed? Or Belarus, for that matter? As you yourself said, they didn't do much of anything about COVID. They have similar population sizes.
There's not much information about the circumstances around his death, so not much can be said. But, people undergoing care for heart issues can rapidly decompensate and die. It's not something that irrefutably indicates homicide.
Andry Rajoelina (attempted assassination)
6 people (including 3 foreigners) tried to kill Madagascar's president on July 23, 2021 - but failed. In April 2020, he had launched a herbal remedy for COVID - which the WHO promptly shat on:
So, he launched an herbal remedy for COVID, and over a year later there was an assassination plot against him. Okay...
The wording "tried to kill" makes it seem as though there was a failed attempt on his life, which isn't what happened. There was reportedly a plot to kill him, which was discovered by the government, and foiled.
I spent some time reading about the case. The bottom line is that they had emails and audio recordings of the conspirators discussing the plot. To this date, no information suggesting it to be motivated by his response to COVID, particularly at the behest of some shadowy cabal of elites, has been uncovered. Some of the conspirators were sent to prison.[283][284][285]
Interestingly, recently Andry Rajoelina pardoned some of the conspirators involved in his own assassination plot. Although, the plot was also meant to kill other politicians besides Rajoelina. Per Le Monde's reporting: [286]
>Paul Rafanoharana Maillot was freed by Madagascar's president, Andry Rajoelina, who then fled the country. 'I don't want to be used as a pawn,' he told Le Monde in an interview.
France News also reported on the pardons.[287]
>Malagasy President Allegedly Pardoned Two Former French Officers Involved in 2021 Coup Attempt: Document
>A copy of a document circulating online includes the names of two agents, Paul Maillot Rafanoharana and Philippe Marc François, sentenced to 20 and 10 years, respectively.
>Earlier in the day, French media reported that Andry Rajoelina, facing an unprecedented protest, had been evacuated by a French military plane.
The whole situation seems very shady and dirty, Andry Rajoelina to me seems to be a crooked, authoritarian politician doing nothing to redistribute wealth in his impoverished nation. The people who allegedly tried to kill him certainly weren't altruistic operatives either, they were a group of mostly wealthy people, some had ties to the French government, which of course actively destabilizes African countries. A supposed link to an oil company (Madagascar Oil) came up during the investigation.[288] There might've been a motivation to get rid of Rajoelina in order to stabilize Madagascar's economy, so Western capitalists could extract its natural wealth more efficaciously.
And now he's pardoning them, probably as part of some crooked backroom deal in order to remain in power, or not wind up dead. I can't say I'm terribly knowledgeable on Madagascar's politics, I have half an opinion on it, which is still more than what digdeeper has. I'd prefer to keep this to a discussion about COVID, because things are getting pretty far off topic now. The bottom line, as I said, is nothing about this relates to COVID at all.
Anyway, to backtrack to what we were meant to be discussing, digdeeper brings up Rajoelina's snake oil.
In response to the launch of Covid-Organics, the WHO said, in a statement sent to the BBC, that the global organisation did not recommend "self-medication with any medicines... as a prevention or cure for Covid-19".
As you can see, the WHO hates the idea of you being your own doctor - you just got to take the jab and stay home. This could provide context for why Andry was targeted later. And hey, guess which remedy turned out better?
>Several extracts as well as Covid-Organics inhibited SARS-CoV-2 and FCoV infection at concentrations that did not affect cell viability.
Another study:
>Hot-water leaf extracts based on artemisinin, total flavonoids, or dry leaf mass showed antiviral activity with IC50 values of 0.1-8.7 μM, 0.01-0.14 μg, and 23.4-57.4 μg, respectively.
Let's see
Here is first study cited: [289]
>In vitro efficacy of Artemisia extracts against SARS-CoV-2
Another in vitro study. I wonder if this will alter the implications of the study in how digdeeper presented it.
>Background
>Traditional medicines based on herbal extracts have been proposed as affordable treatments for patients suffering from coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Teas and drinks containing extracts of Artemisia annua and Artemisia afra have been widely used in Africa in efforts to prevent SARS-CoV-2 infection and fight COVID-19.
>Methods
>The plant extracts and Covid-Organics drink produced in Madagascar were tested for plaque reduction using both feline coronavirus and SARS-CoV-2 in vitro. Their cytotoxicities were also investigated.
>Results
>Several extracts as well as Covid-Organics inhibited SARS-CoV-2 and FCoV infection at concentrations that did not affect cell viability.
>Conclusions
>Some plant extracts show inhibitory activity against FCoV and SARS-CoV-2. However, it remains unclear whether peak plasma concentrations in humans can reach levels needed to inhibit viral infection following consumption of teas or Covid-Organics. Clinical studies are required to evaluate the utility of these drinks for COVID-19 prevention or treatment of patients.
So, the researchers don't even know if this herbal remedy will do anything in a real world scenario. They specifically state that clinical studies are required. Did digdeeper read the study? This is not definitive proof.
The second study cited: [290]
>Artemisia annua L. extracts inhibit the in vitro replication of SARS-CoV-2 and two of its variants
This is yet another in vitro study, which should be followed up with clinical trials.
The full text of the second study can be found here: [291]
>A. annua extracts inhibit SARS-CoV-2 infection, and the active component(s) in the extracts is likely something besides artemisinin or a combination of components that block virus infection at a step downstream of virus entry. Further studies will determine in vivo efficacy to assess whether A. annua might provide a cost-effective therapeutic to treat SARS-CoV-2 infections.
I looked and so far haven't found clinical trials.
This is, again, not evidence of a reliable treatment for COVID.
These could suggest artemisia can treat COVID, but actual clinical trials are needed in order to make such a determination. It's been five years, and I can't seem to find any.
Even if Covid-Organics did nothing (which is contradicted by the above studies), it would still be better than the WHO's measures which are actually negative - while the herbal remedy isn't going to hurt you.
Wrong. You can overdose on those herbs. Probabilistically speaking, stupid people will take massive doses in order to cure themselves of COVID, and overdose. Additionally, the potentially false sense of security one may have thinking that they have a treatment for COVID could cause them to act recklessly, and endanger their health, or the health of others, by spreading/contracting COVID. You're just reversing the reality of the sitution, as per usual.
And so, we have 3 cases (plus one almost-case) of presidents who heavily disagreed with the WHO / NWO prescription for the "pandemic" and died during it. Those who died were promptly replaced by pro-WHO / NWO ones. Why did none of this happen to all the cucked European / Asian / USA presidents that went full speed into the restrictions?Trump infamously had a delayed response to COVID which killed many people, and also gave a lot of dumb advice. Salon magazine reported that Trump said COVID was going to disappear over 40 times.[292]
>Trump’s time in the White House during the pandemic was fraught with stream-of-consciousness sound bites that often contradicted national or global health advisories. He suggested injecting bleach to fight COVID, recommended people take the anti-malaria drug hydroxychloroquine, which had not shown to be safe, and encouraged people to protest social distancing restrictions. In the early months, he denied the threat of the pandemic, saying some iteration of the fact that the COVID pandemic was “going to disappear,” over 40 times.
>Prior to the pandemic, Trump dismantled a pandemic preparedness initiative that Barack Obama had started in his presidency. During the pandemic, he fired top public health officials and withdrew funding to the World Health Organization (WHO). Overall, he responded in a political manner rather than one based on science, which created an opposition to public health among many of his supporters, said Dr. Angela Rasmussen, a virologist at the Vaccine and Infectious Disease Organization (VIDO) at the University of Saskatchewan.
All he did was authorize Warp Speed to rapidly produce vaccines, which most of his supporters didn't even want to take anyway. Need I mention Belarus and Sweden again, which you yourself cited.
Maybe Thomas Matthew Crooks was dispatched by Bill Gates to kill Donald Trump? After all, Trump told people to take HCQ for COVID, and a mere 4 years later was nearly killed in two assassination plots. One of his assassins was in a Black Rock commercial. It can't be a coincidence.
If it's not about your health, then what?
Travel / flight bans
Obviously a way to deny people the ability to meet their families in other countries. Also teaches you that you are limited in your movements to a certain area at all times - that is, unless you get the permissions of your masters.
Or, a way to lower the spread of the disease.
Shutting down businesses
Thank our capitalist government for permitting monopolies to swoop in and devour the weaker, small businesses.
Quarantines / curfews
It's how you curb an outbreak of disease. They've been used routinely throughout history.
And don't you dare defy them!
Dystopian Footage: Quarantine Breaker Subdued And Arrested By Swarm Of Police In Hazmat Suits
You can thank police militarization for this.
Oh, it happened in Israel — an inherently fascist, militaristic, poisonous society, what a shock.
Mask mandates
Masks have a symbolic meaning of shutting your mouth, so it teaches you that you don't have a say. Also, much of human communication is through facial expressions, and the masks destroy that. You now have no idea whether the person next to you is angry, scared, serious or making a joke, etc. which surely isn't good for social connections. The authorities really need you to wear your muzzle, you good doggie you:
It's an interesting metaphorical analysis, but they also lower the amount of droplets containing virions one can exhale and inhale, which can lower one's risk of infecting others.
Contact tracing
Or they're just trying to track the spread of disease instead of letting it run wild.
They already track everything else electronically. People knew about XKeyscore and PRISM for almost a decade prior to COVID, but they didn't care then. They knew about the FBI's massive network of undercover informants deployed during the War on Terror to entrap Muslim teenagers, several times larger than the forces deployed during COINTELPRO, but they didn't care. Now we have AI powered surveillance systems on highways. We have a TAO-style unit operating out of ICE, surveilling social media, with access to Pegasus spyware — Pegasus spyware which is already used by many governments worldwide, by the way. The government is openly targeting people who are "anti-American", "anti-capitalist". Wanting to not be left to die in your hospital bed because of insurance companies is "anti-capitalist". The government is now arbitrarily executing random non-white fishermen in the Carribean with drones, while mounting a massive invasion of Venezuela and other Latin American countries as part of the Monroe Doctrine, while also using secret police to round up and deport American citizens and residents on the basis of them appearing Hispanic or Latino. Nobody cares, because Americans are pathetic, slovenly, imperialist worms. They pretend to hate imperialism, and capitalism, but deep down, they love these things, and only wish to minimize how these things cause harm to theirselves (imperial boomerang). You can see it in American "leftists" reverence for Graham Platner, an American mass murderer. Whoops, I meant to write American combat veteran and former Blackwater mercenary. Platner relished in murdering Iraqis and Afghans, because he's a psychopath. American "leftists" are overlooking and even justifying this, because Platner is offering them socialized medicine. Europeans are hardly any better. America offloads CIA blacksites onto them, in your very own country of Poland actually, and they willingly accept them, because they're limp-wristed, pathetic, cucks, who benefit from American imperialism. They willingly host American military bases. They participated in such atrocities as the invasion of Iraq. Watch as Europe becomes a fascist shithole as its material conditions worsen due to the forces of American capitalists.
Social distancing / bans on gathering
Destroy friendships, families, social connections in general. Create a world where everyone is suspicious of the other person.
People do this to themselves. Sometimes it's even necessary to cut ties with people.
Censorship / opinion manufacture
Simple - can't have people doing independent research. All must buy into the fearmongering narrative! These headlines should say it all:
These problems, again, predate COVID, and have extended far beyond it to this day. Look at how Britain and America treat pro-Palestine protestors.
Deprecation of cash
This didn't happen.
Forced vaccines
By looking at the punishments for not being vaccinated, we can see that this issue is really important to the ruling class:
These examples are not forced, more so coerced. And is it unjustifiable? In order to participate in social gatherings, they compel you to receive a vaccine so as to prevent the transmission of the pathogen. I don't think that's unreasonable. People were completely free to abstain from the vaccine, but as a result they'd miss out on social events. That's their price to pay for refusing a safe, easily accessible vaccine. Forced vaccination has been the norm throughout history. They've done it in America, and they've done it around the world. The authorities would physically compel people to take a vaccine if they tried to refuse. They'd go around vaccinating everybody, with no choice of abstaining. This was how countries eradicated things like smallpox. This time around people were spared this sort of authoritarian action and given an actual choice, but of course, it's not enough for the conspiracist. It speaks to their entitlement.
If this was not a PSY-OP
It would have happened naturally, instead of being predicted a few weeks earlier (Event 201).
Well, it did, so there's no issue there. Already went over Event 201.
They - upon the discovery of the genetic sequence of the virus - would have actually first proven that it (alone) caused the ailments that were attributed to it. Instead - whenever someone gets "sick with COVID-19" - they just assumed it was the virus that did it, while ignoring contributors such as their chronic diseases, environmental hazards, etc.
No, they determined that it was COVID which killed them. You didn't bother to understand how this determination was made. They accounted for the other diseases that contributed, there was a distinction between deaths caused by COVID and deaths involving COVID.
They would have actually developed a test with a good enough accuracy before releasing infection statistics based on a weak test or no test at all.
You misinterpreted the utility of the COVID tests.
The hospitals would have put COVID-19 as the cause of death only if it could have actually been shown.
Which is what happened.
The media would have made clear all the caveats about the death rates (instead, they spread "the number" like gospel).
The media would have used only real footage and stories that actually support the stated conclusions (instead we were flooded with fake news about burning corpses, crowded hospitals, or young healthy people getting sick).
I only saw those stories around conspiracy websites. Nonetheless, the media does fearmonger. Wakey wakey, read a news headline some time. That doesn't mean there's a conspiracy. The mainstream media abandoned reliable and responsible reporting decades ago.
The media would have run things as usual with a few brief updates on the current situation, instead of fearmongering pretty much 24 / 7.
Fearmongering is profitable. You have an article about the profit motive, add this to it. Better yet, read some books on the subject, instead of sitting in your conspiracy bubble thinking you know everything, as though you don't have an overlap in opinion with millions of other people, and have isolated yourself from them by believing stupid things.
The governments would have implemented only the policies for which there was evidence of being helpful to lessen the damage of the pandemic.
They did. Quarantining, social distancing, using masks, lockdowns, vaccinating people. All of those measures served to lower transmission. Even if some were not effective, you still can't blame the government for trying when those measures have been proven to work in the past. In such a scenario, they would have had no way of knowing the measures would be ineffective.
The health authorities would have jumped on the opportunity to enhance the people's immune systems by proven means such as vitamins - instead, those were actually attacked.
Nobody is telling people to not care for their nutrition, in fact, it's common knowledge that bad nutrition increases your risk of illness. All people said was that it's not the be all end all of things, it's not a cure, it's not a universal treatment.
People would actually be able to voice their concerns, instead they're being banned from the social platforms, fined for spreading alleged fake news and even prevented from reading contrary information.
People were spreading false information. Assuming there is a virus that is spreading around harming people and the measures taken against it worked, and a person said those measures didn't work and encouraged people to oppose those measures, then they could be contributing to the spread of disease. If people followed their advice to oppose the measures, then they did contribute to the spread. I don't agree with the response by some governments, but again, that only speaks to the misgivings of some governments, it doesn't mean there's a grand conspiracy to fake everything. The authoritarian responses of governments are emblematic of a greater rot, predating COVID.
The overall conclusions of this article are almost completely false. You took scant bits of inflammatory, sensational evidence to make sweeping, absolutist conclusions.
You did this with the Pfizer vaccine trials, with the safety and effectiveness of the vaccines, with hospitals supposedly not being overrun with COVID patients, with deaths being wrongly attributed to COVID, with the virus originating from a lab, and more.
It's sensible to be concerned with all of these things and investigate them, but you instead jumped to conclusions about the nature of the pandemic off of these bits of evidence. When considered in full context, the discrepancies you've displayed are not indicative of a conspiracy. They indicate the cherrypicking of evidence to make a case that would otherwise not hold up.
Without evidence of a conspiracy to create a virus and inflate the specter of the pandemic, most of the actions of the establishment — corporations, media, and government — lose the appearance of unusual malice, negligence, and incompetence.
The media, for instance, fearmongered with the pandemic. This worsened people's fears and likely caused real harm to them. It also backfired in ways, causing people who saw their fearmongering and concluded that it must be part of an overarching conspiracy, which in turn drove people's suspicions of the harmfulness of the virus and effectiveness of the vaccines. This probably prolonged the pandemic and its harm.
But this sort of malice is not unusual, unfortunately. The media does this all of the time. It's not unusual for them to have leapt onto the pandemic crisis for profit.
Some governments took advantage of the pandemic in order to censor people and lock them up. But again, governments do these sorts of things around crises. It's the perfect time for them to seize power. It's not an usual sort of malice. The fact that much of this power was relinquished undermines the notion of the pandemic serving as some event to cement a global tyranny.
Some authorities could have implemented lockdown measures which were ineffective, and when evidence of this became known, either stubbornly persisted in maintaining those measures, or failed to recognize this evidence, or some combination of the two. Both of these kinds of things happen around crises. Governments and other authorities sometimes refuse to admit that they were wrong about certain things, to the detriment of the public. Other times, they fail to see the errors of their ways, due to some sort of disconnect. It's not an usual sort of malice.
It is important for us to be measured and nuanced in our analysis of our institutions.
Careless analysis, credulously depending upon people who do not know what they're talking about, or are liars, leaves us vulnerable to manipulation by conmen.
It steals away people's focus from real issues, in their relation to perceived conspiracy events.
It can be seen with COVID.
COVID lead people to financial ruin, it drove people to homelessness, many small businesses closed down forever.
In the case of America, many deaths could have been prevented had there been universal healthcare. We could interrogate why our government permitted corporations to bleed us dry in the midst of a pandemic, while doing little to assist us, and why these corporations would seize upon the opportunity to exploit us. It would lead to the conclusion that corporations are ultimately vessels for extracting and aggregating wealth, and nothing more, such that they will do this to deleterious effect, and ultimately profit further off of the socially deleterious ramifications of their actions. Politicians are merely put in place to oversee the processes of these corporations, while ensuring that society does not completely break down. Over the passage of time, the government itself exercises greater control over the populace, and it permits corporations to also exercise greater control over the populace; often they engage in joint ventures to control the populace. This has implications for the global population, XKeyscore and PRISM being an example. A mass surveillance program authorized by the politicians of one nation, permitted to survey virtually everyone on earth. The politicians occasionally make concessions to the general populace, minutely increasing the standard of living in isolated parts of the country with localized legislation, but in recent history they cannot be said to have done anything more.
This has not happened here though, digdeeper has spent his time raving about how all of the governments on earth, and most influential institutions, have conspired to hoax a global pandemic, for the sake of... Well, doing what they've already been doing for decades. In spite of this, every control placed upon citizens was ultimately lifted. And plenty of inconsistencies could be seen when examining responses to COVID on a global scale. Belarus' government chose to ignore the pandemic, while Russia's did not. Sweden chose to have a weak response to the pandemic. NATO-controlled Sweden, a participant in western intelligence sharing networks, also often loathingly characterized by conspiracists as an authoritarian nation. It forces a more nuanced analysis of these governments, which is nonexistent among conspiracists.
The perception is such: Yes, governments and the capitalist class do all of these things, but they also hoax events like the COVID pandemic or the Moon landings, and this is important too.
I don't doubt from the perspecive of a delusional, true-believer of these conspiracy theories, that they are very important to "expose". But, none of it is true. These things really did happen.
So, why does any of this matter then, if our institutions are corrupt and largely evil?
Because you're denying the reality of a pandemic that killed millions of people worldwide.
It caused untold levels of human suffering.
The virus did this by killing people, and by creating economic instability through its hazardousness, which destroyed the lives of countless mostly-poor people.
You crusaded against any measures to try and stamp out the virus, the most effective of them being the vaccines, which reliably prevented infections and deaths from COVID. The very thing that offered to end the pandemic is what you crusaded against. You wanted to open society back up, which would have been to the detriment of everyone, yourself included, all because you weren't content living life behaving as though there was a deadly pandemic going on.
You feigned concern for the wellbeing of others when mentioning how lockdowns could cause harm to people, especially young people's, mental health, but at the same time you couldn't care less about those who actually died because of COVID, going as far to say that their deaths were outright fraudulent, solely because they were old or sick. It was very callous and quite disturbing.
This sort of callousness will drive people away from you and from people like you. It's deranged. It only serves to impede substantive, positive political change. So much time and effort is wasted upon nonsense that actively causes people to harm themselves and others, in this case by spreading disease, while real issues get sidelined.
In the vein of COVID and vaccines, vaccine hesitancy in America, which had been established long before COVID and was steadily rising, exploded during and after the pandemic. And thanks to America's worldwide cultural dominance, vaccine hesitancy is beginning to rise in European countries. This is causing children to contract easily-preventable diseases, killing them, and leaving survivors with long-term sequelae, which in the case of diseases like measles could kill them later in life.
Digdeeper reveals in the conclusion of his article his displeasure with the limitations of real medicine, in its ability to "cure" chronic diseases, like cancers. He wrongly blames modern medicine for its inability to treat everyone on earth.
He perceives modern medicine as being linked to "the establishment", and dismisses its importance and validity on this basis.
This blanket categorization of all medicine as being part of "the establishment", or anything produced by "the establishment", like research into climate change, as being inherently bad, breaks down trust within society, and leaves people vulnerable to predators. This entire article is a testament to that fact, with just how many idiots and liars I've mowed over in my analysis, all of whom digdeeper has fallen for.
When it reaches a collective level, this sort of mentality allows people like RFK Jr. to step in and virtue signal to people about the harmfulness of processed foods, and spread conspiracies about the harmfulness of vaccines, like with the non-existent autism link, in order to build a movement.
It leads people to whitewash the psychology of individuals like RFK. If you point out all of the wrong things he says, others will point out the things he says which may be somewhat valid, like the prevalence of chronic diseases in society. They don't see any other political figures or institutions taking such a stance, and in their desperation for one, they try to legitimize such fools as RFK.
Legitimate health-related issues in society are then hijacked by these conmen, in service of further eroding the health of society, to the enrichment of those in power.
RFK Jr., while spreading his lies about vaccines, and tylenol, and promoting nonsense like cod liver oil and methylene blue and whatever else, has ultimately spearheaded a movement which has scuttled government programs studying child cancer, and developing vaccines for diseases like pancreatic cancer, which were beginning to show results.
All the while, the government is now moving to loosen regulations on PFAS.
It lays bare the whole conspiracy. There is no care given for the health of society whatsoever by individuals like RFK Jr., concern is merely feigned for the sake of mobilizing a movement that will shrink the government, in order to lessen taxation of the rich, all while making the populace sicker, by depriving them of potentially life-saving treatments, dare I say cures, for cancer, and regulations designed to keep carcinogens out of their water.
Digdeeper no doubt has fallen for some of the lies of RFK Jr. himself, seeing how he cited his drama with Peter Hotez as a meaningful event. As though RFK is not a person to have been ignored prior to his ascension to power.
He begins to pontificate upon his dissatisfaction with modern medicine with the paragraph:
According to this timeline of medical history, "the first successful appendectomy" had been performed in the year 1763. I'll mark that as the start of modern medicine, as it seems like the first incidence of a truly "modern" medical procedure. So, 261 years of existence and yet the only diseases that are claimed to have been cured are the infectious ones. And yet, if you actually read the article, most of those diseases still exist and keep wreaking havoc:
>Even with proper antibiotic treatment, diphtheria kills about 10 percent of the people who contract it.
A vaccine for diptheria exists. Because of widespread childhood vaccination, which produces herd immunity, there are virtually no cases in developed countries. People who develop the illness are usually unvaccinated and impoverished. This is an issue with the accessibility of a vaccine, if anything.
According to the CDC, pertussis causes 10 to 20 deaths each year in the United States, and there were 25,000 cases reported in 2004. Worldwide, the disease causes far more damage -- about 50 million people around the world are infected annually, and WHO estimates around 294,000 deaths each year.
This is also preventable by vaccination. It used to be rare in developed countries like the USA, but it's becoming more common thanks to anti-vaxxers. Most cases occur in the developing world, because access to vaccines in those countries is limited. The unequal exchange these countries suffer from, alongside the destabilization from foreign powers, deprives them of the resources and organization to develop their own infrastructure to provide themselves with an adequate supply of vaccines. This has nothing to do with medicine itself, it's politics.
WHO estimates that annually pneumococcal disease is responsible for 1 million fatal cases of respiratory illness alone; most of these cases occur in developing countries.
This is the same as above, although not all pneumococcal diseases leading to death are vaccine-preventable, lack of access to vaccines is a contributor. A significant factor is a lack of access to adequate care. There can be a scarcity of medications used to treat illnesses, and people can be kept in unsanitary conditions at hospitals or treatment centers. In the developed world, we see far less mortality because we have enough resources for these problems to not manifest at the same scale.
This is blaming medicine for the ills of capitalism.
There is also the question of whether modern medicine actually had anything to do with the decreased incidence of the infectious diseases, and for many, it seems that the answer might be no, or at most a very small percentage contribution. But even if we treated those few infectious diseases as success stories of modern medicine, the full picture is still quite pathetic as not a single chronic disease has been cured during its 261 years of reign and in fact more and more new ones keep popping up. That's despite plenty of data already being available in scientific journals - "PubMed® comprises more than 36 million citations for biomedical literature from MEDLINE, life science journals, and online books". I think if this "more data" approach was supposed to work, we'd already be seeing some effects, but there are literally none in terms of actual cures
It really is incredible just how moronic digdeeper is. To call the eradication of diseases like smallpox and polio pathetic and insignificant. Smallpox, a disease which ravaged every human civilization, killing hundreds of millions over the course of human history, killing up to 300 million in the 20th century alone.[293] It really gives insight into how illiterate digdeeper is, and how his illiteracy causes him to have such little appreciation for modern medicine.
Or alternatively polio, another ancient disease, which in the 20th century killed hundreds to thousands of people every year in America, and paralyzed many more.[294]
His appreciation for this is completely blinded by his inability to grapple with the fact that the antiquated notion of a cure does not actually exist. When people have a disease, you treat them, and they can be cured. But, there's no guarantees that they will be cured. You can alternatively vaccinate people against some diseases, which prevents them from ever falling ill/seriously ill. That's about as far as it goes. If someone has a condition like scurvy, you might "cure" them with vitamins, but scurvy isn't an infectious disease.
He links off to another article of his on the profit motive which contains more supposed evidence to support his disdain for modern medicine, which I would like to discuss as part of my conclusion.
It discusses the cancers of capitalism and the profit motive, and is named "How money and the profit motive destroy everything".[295]
In his article on the profit motive, after discussing the harmfulness of junk food, digdeeper introduces "other health-destroying things", most of the 'things' being unproven to be harmful in his presentation of their harmfulness, some of the 'things' even beneficial in ways.
Air pollution and second-hand smoking, as mentioned by digdeeper, are definitely very harmful and kill countless people every year, but basically everything else he brings up is not inherently harmful.
Water fluoridation:
https://fromthetrenchesworldreport.com/fluoride-in-tap-water-how-toxic-is-it/38975
>23) Fluoride may lower IQ. There have now been 33 studies from China, Iran, India and Mexico that have reported an association between fluoride exposure and reduced IQ. One of these studies (Lin 1991) indicates that even just moderate levels of fluoride exposure (e.g., 0.9 ppm in the water) can exacerbate the neurological defects of iodine deficiency. Other studies have found IQ reductions at 1.9 ppm (Xiang 2003a,b); 0.3-3.0 ppm (Ding 2011); 1.8-3.9 ppm (Xu 1994); 2.0 ppm (Yao 1996, 1997); 2.1-3.2 ppm (An 1992); 2.38 ppm (Poureslami 2011); 2.45 ppm (Eswar 2011); 2.5 ppm (Seraj 2006); 2.85 ppm (Hong 2001); 2.97 ppm (Wang 2001, Yang 1994); 3.15 ppm (Lu 2000); 4.12 ppm (Zhao 1996). In the Ding study, each 1 ppm increase of fluoride in urine was associated with a loss of 0.59 IQ points. None of these studies indicate an adequate margin of safety to protect all children drinking artificially fluoridated water from this affect. According to the National Research Council (2006), “the consistency of the results [in fluoride/IQ studies] appears significant enough to warrant additional research on the effects of fluoride on intelligence.” The NRC’s conclusion has recently been amplified by a team of Harvard scientists whose fluoride/IQ meta-review concludes that fluoride’s impact on the developing brain should be a “high research priority.” (Choi et al., 2012). Except for one small IQ study from New Zealand (Spittle 1998) no fluoridating country has yet investigated the matter.[296]
https://fluoridealert.org/studies/brain01/
>Fluoride & IQ: 76 Studies [297]
Mulling over the studies they cite, you'll quickly notice that they are examining people from developing countries who are exposed to very high levels of fluoride, many of them suffering fluorosis.
There are several reasons why these people aren't comparable to people in developed countries. The reasons can vary slightly from region to region.
The main unifying reason is that they are exposed to very high levels of fluoride. Chronic exposure to high levels of fluoride can lower intelligence. Most people in the developed world don't suffer this, as the fluoride levels people are exposed to through municipal water is kept at safe levels.
Given that they are from developing countries, there could be other toxic chemicals in their environment which could be contributing to IQ lowerage. In some cases, this is explicitly mentioned, e.g: "in coal-burning fluorosis area of Dafang County, Guizhou Province". Do you think those people are equal to people living in a rich town in North America? Most of these studied people who experienced lowered IQ are from developing parts of China, Iran, India, and Southeast Asia, where they are exposed to toxins and high levels of naturally-occurring fluoride in their water.
When you look at people from developed countries, where they aren't exposed to high levels of fluoride, and various toxic chemicals, you don't notice lowered IQ.
In this study from New Zealand, which spanned three decades, no lowered IQ was observed. In fact, there was a one or so point increase correlated with community water fluoridation, though that could be coincidence or other elements of the environment of those in fluoridated areas, maybe higher standards of living or education. They also saw fewer cavities in those with fluoridated water.[298]
In this Swedish study, out of over 80,000 people examined, fluoridated water had no effect on cognitive ability, but was beneficial to oral health. They also correlated exposure to fluoride with greater monetary earnings later in life.[299][300]
This Australian study also did not link fluoride exposure in childhood to lowered IQ.[301]
Many observational studies find that water fluoridation prevents dental caries by up to around 25%. But, a lot of studies do tend to be flawed. A lot of them are old and have methodological issues which undermine their veracity. To this day, fluoridation is correlated with lower incidences of dental caries, however.[302][303][304]
This could shift the discussion of water fluoridation from its harmfulness to how beneficial it is. It may not be extremely beneficial, depending on the context, but it doesn't seem to be inherently harmful, besides being a "waste of tax dollars".
Cell phone radiation:
>The Interphone Study is the granddaddy of all the study findings into cell phone radiation and the safety of cellphones for humans. At a cost of $25 million, this is the largest study of cell phone use and tumor risk conducted to date. It found that “regular use of a cell phone by adults can significantly increase the risk of gliomas by 40% with 1640 hours or more of use.” This equates to about 30 minutes per day over ten years.[305]
Notice how it is always deeply flawed studies these people cite?
This study examined cancer patients by serving them questions relating to cell phone usage. This is prone to bias, and in no way definitively shows a link between phones and cancer. They could be causing people to falsely recall information in their desire to rationalize their situation. Memory recall is not a great foundation to base the claim that phones cause brain cancer off of. It could prompt further study, but definitely isn't proof in and of itself.
There are many other problems with the Interphone Study, but I don't need to get into them to refute the claims that the study made.
There are decades worth of statistics on cancers in several countries, including countries with robust reporting systems for disease like America, Norway, Sweden, and Finland. Analysis of these statistics reveals generally stable incidence rates of glioma. In some cases, decreases can be observed.
Surely there would have been an increase by now? Cancer may develop slowly, but if there was a carcinogen practically ever-present among the majority of developed countries for 20-30 years, I would think that it would have produced evidence of its existence by now. Yet it hasn't.
Sweden: minute decrease in glioma cases observed over course of 30 years[306] [307]
>No Evidence for Increased Brain Tumour Incidence in the Swedish National Cancer Register Between Years 1980-2012 >Background/aim: The main objective of this study was to evaluate if there was an increased incidence of brain tumours between years 1980-2012, a time period when mobile phone usage has increased substantially. >Materials and methods: From the Swedish Cancer Registry, cases of meningiomas, low-grade gliomas (LGG) and high-grade gliomas (HGG) were identified in patients between 1980-2012. Direct age-standardised incidence rates were used to calculate incidence trends over time. >Results: A total of 13,441 cases of meningiomas, 12,259 cases of high-grade gliomas and 4,555 cases of LGG were reported to the register during the study period. The results suggest that there may be a negative development in the trend for LGG of -0,016 cases per 100,000 and year, corresponding to a mean reduction of approximately 1% per year. >Conclusion: The present study was not able to demonstrate an increased incidence of glioma during the past 30 years in Sweden.
No significant increase in glioma case rates in Finland, Sweden, and Norway: [308]
>Time trends in mobile phone use and glioma incidence among males in the Nordic Countries, 1979–2016
>Introduction
>In the Nordic countries, the use of mobile phones increased sharply in the mid-1990s especially among middle-aged men. We investigated time trends in glioma incidence rates (IR) with the perspective to inform about the plausibility of brain tumour risks from mobile phone use reported in some case-control studies.
>Methods
>We analysed IR of glioma in Denmark, Finland, Norway, and Sweden among men aged 40–69 years, using data from national cancer registries and population statistics during 1979–2016, using log-linear joinpoint analysis. Information on regular mobile phone use and amount of call-time was obtained from major studies of mobile phones in these countries. We compared annual observed incidence with that expected under various risk scenarios to assess which of the reported effect sizes are compatible with the observed IR. The expected numbers of cases were computed accounting for an impact of other factors besides mobile phone use, such as improved cancer registration.
>Results
>Based on 18,232 glioma cases, IR increased slightly but steadily with a change of 0.1% (95 %CI 0.0%; 0.3%) per year during 1979–2016 among 40–59-year-old men and for ages 60–69, by 0.6 % (95 %CI 0.4; 0.9) annually. The observed IR trends among men aged 40–59 years were incompatible with risk ratios (RR) 1.08 or higher with a 10-year lag, RR ≥ 1.2 with 15-year lag and RR ≥ 1.5 with 20-year lag. For the age group 60–69 years, corresponding effect sizes RR ≥ 1.4, ≥2 and ≥ 2.5 could be rejected for lag times 10, 15 and 20 years.
>Discussion
>This study confirms and reinforces the conclusions that no changes in glioma incidence in the Nordic countries have occurred that are consistent with a substantial risk attributable to mobile phone use. This particularly applies to virtually all reported risk increases reported by previous case-control studies with positive findings.
Norway: stable case rates of glioma [309]
>Stable glioma incidence and increased patient survival over the past two decades in Norway: a nationwide registry-based cohort study
>Background
>Surveillance of incidence and survival of central nervous system tumors is essential to monitor disease burden and epidemiological changes, and to allocate health care resources. Here, we describe glioma incidence and survival trends by histopathology group, age, and sex in the Norwegian population.
>Material and methods
>We included patients with a histologically verified glioma reported to the Cancer Registry of Norway from 2002 to 2021 (N = 7,048). Population size and expected mortality were obtained from Statistics Norway. Cases were followed from diagnosis until death, emigration, or 31 December 2022, whichever came first. We calculated age-standardized incidence rates (ASIR) per 100,000 person-years and age-standardized relative survival (RS).
>Results
>The ASIR for histologically verified gliomas was 7.4 (95% CI: 7.3–7.6) and was higher for males (8.8; 95% CI: 8.5–9.1) than females (6.1; 95% CI: 5.9–6.4). Overall incidence was stable over time. Glioblastoma was the most frequent tumor entity (ASIR = 4.2; 95% CI: 4.1–4.4). Overall, glioma patients had a 1-year RS of 63.6% (95% CI: 62.5–64.8%), and a 5-year RS of 32.8% (95% CI: 31.6–33.9%). Females had slightly better survival than males. For most entities, 1- and 5-year RS improved over time (5-year RS for all gliomas 29.0% (2006) and 33.1% (2021), p < 0.001). Across all tumor types, the RS declined with increasing age at diagnosis.
>Interpretation
>The incidence of gliomas has been stable while patient survival has increased over the past 20 years in Norway. As gliomas represent a heterogeneous group of primary CNS tumors, regular reporting from cancer registries at the histopathology group level is important to monitor disease burden and allocate health care resources in a population.
Norway: no noticeable time trend in glioma cases [310]
>Incidence trends of adult glioma in Norway and its association with occupation and education: A registry-based cohort study
>Background: Gliomas constitute 75 % of all malignant primary adult brain tumors. Being the most frequent histologic subtype, glioblastomas (GBMs) cause substantial morbidity and mortality worldwide and the Nordic countries have some of the highest incidence rates in the world. Therefore, we investigated the incidence of gliomas in Norway including time trends and associations with education and occupation.
>Methods: We retrieved individual-level data from databases at Statistics Norway containing information on education and occupation and linked them to data on adult glioma patients diagnosed during 2004-21 from the Cancer Registry of Norway. Age-standardized incidence rates (ASIRs) (World Standard Population) were calculated and analyzed with regards to sex and morphology. Poisson regression was used to test for time-trends, and to analyze the associations between education, occupation and glioma incidence, adjusted for age, sex, and calendar year. Estimates were reported as incidence rate ratios (IRRs) with 95 % confidence intervals (CIs).
>Results: The overall ASIR of gliomas (per 100,000 person-years) was 7.1 (95 % CI 6.9-7.3), with no specific time trend during the study period. The incidence increased with age. Compared to the other subtypes, GBMs were diagnosed at older ages. The risks of developing glioma overall and GBM were associated with occupation but not with educational level. The relative risk of glioma and GBM were respectively 1.17 (95 % CI 1.05-1.31) and 1.17 (95 % CI 1.02-1.35) among high-skilled white-collar workers compared to blue-collar workers.
>Conclusions: The overall and sex-specific ASIRs of gliomas and GBMs did not show any noticeable time trends. The higher risk of developing glioma overall and GBM in high-skilled white-collar workers compared to blue-collar workers calls for further investigations.
Finland: 1.6% increase in glioma observed from 2000-2013, patients becoming older as time passes [311]
>Background
>We assessed population-level changes in glioblastoma survival between 2000 and 2013 in Finland, with focus on elderly patients (>70 y) in order to assess if changes in treatment of glioblastoma are reflected also in population-based survival rates.
>Methods
>We identified all patients (age ≥18 y) from the Finnish Cancer Registry (FCR) with a histopathological diagnosis of primary glioblastoma in 2000–2013. Patients were followed up until December 2015. The accuracy of register-based search of glioblastoma patients was internally validated. We report age-standardized relative survival ratios and relative excess risks (RERs) of death in 2000–2006 (pre-period) and 2007–2013 (post-period).
>Results
>We identified 2045 glioblastoma patients from the FCR. The accuracy of the FCR-based search was 97%. Median age was 63.3 years, and 42% were women. Incidence increased on average by 1.6% (P = 0.004) and median age by 0.4 years per calendar year. Between the pre- and post-periods, the proportion of patients >70 years increased from 24% to 27%. In >70-year-old patients, the median survival time increased from 3.6 months in 2000–2006 to 4.5 months in 2007–2013 (RER 0.82, 95% CI: 0.68–0.98). In ≤70-year-old patients, the median survival time increased from 9.3 months in 2000–2006 to 11.7 months in 2007–2013 (RER 0.74, 95% CI: 0.67–0.82).
>Conclusion
>Despite the increased proportion of elderly glioblastoma patients, population-level survival of glioblastoma patients has improved since the year 2000. However, increasing incidence, increasing age of patients, and poor survival in elderly are alarming, and future studies should perhaps focus more on elderly.
Finland: 1990-2016, stable case rate in time span observed [312]
>Incidence trends of adult malignant brain tumors in Finland, 1990–2016
>Background: Several studies have reported increased incidence trends of malignant gliomas in the late 1900s with a plateau in the 2000s, but also some recent increases have been reported. The purpose of our study was to analyze incidence trends of malignant gliomas in Finland by morphology and tumor location.
>Material and methods: Data on 4730 malignant glioma patients were obtained from case notifications to the nationwide, population-based Finnish Cancer Registry (FCR), and less detailed data on 3590 patients up to 2016. Age-standardized incidence rates (ASR) and average annual percent changes (APCs) in the incidence rates were calculated by histological subtype and tumor location.
>Results: The incidence rate of gliomas was 7.7/100,000 in 1990–2006 and 7.3 in 2007–2016. The incidence of all gliomas combined was stable during both study periods, with no departure from linearity. In an analysis by age group, increasing incidence was found only for ages 80 years and older (1990–2006). During both study periods, incidence rates were increasing in glioblastoma and decreasing in unspecified brain tumors. In 1990–2006, rates were also increasing for anaplastic oligodendroglioma, oligoastrocytoma and unspecified malignant glioma, while decreasing for astrocytoma. As for tumor location, incidence in 1990–2006 was increasing for frontal lobe and brainstem tumors, as well as those with an unspecified location, but decreasing for the parietal lobes, cerebrum and ventricles.
>Conclusions: No increasing incidence trend was observed for malignant gliomas overall. An increasing incidence trend of malignant gliomas was found in the oldest age group during 1990–2006.
USA: 1975-2018, decrease in glioma case rates and mortality [313]
>Purpose
>Glioma incidence in the US seems to have stabilized over the past 20 years. It’s also not clear whether changes in glioblastoma incidence are associated with glioma mortality trends. Our study investigated trends in glioma incidence and mortality according to tumor characteristics.
>Methods
>This study obtained data from the Surveillance, Epidemiology, and End Results-9 (SEER-9) registries to calculate glioma incidence and mortality trends. Annual percent changes (APC) and 95% CIs were calculated using the Joinpoint program.
>Results
>62,159 patients (34,996 males and 55,424 whites) were diagnosed with glioma during 1975-2018, and 31,922 deaths occurred from 1995-2018. Glioblastoma (32,893 cases) and non-glioblastoma astrocytoma (17,406 cases) were the most common histologic types. During the study period, the incidence of glioma first experienced a significant increase (APC=1.8%, [95% CI, 1.3% to 2.3%]) from 1975 to 1987, and then experienced a slight decrease (APC=-0.4%, [95% CI, -0.5% to -0.3%]) from 1987 to 2018, while the APC was 0.8% for glioblastoma, -2.0% for non-glioblastoma astrocytoma, 1.1% for oligodendroglial tumors, 0.7% for ependymoma and -0.3% for glioma NOS during the study period. Glioblastoma incidence increased for all tumor size and tumor extension except for distant. From 1995 to 2018, glioma mortality declined 0.4% per year (95% CI: -0.6% to -0.2%) but only increased in patients older than 80 years [APC=1.0%, (95% CI, 0.4% to 1.6%)].
>Conclusion
>Significant decline in glioma incidence (1987-2018) and mortality (1995-2018) were observed. Epidemiological changes in non-glioblastoma astrocytoma contributed the most to overall trends in glioma incidence and mortality. These findings can improve understanding of risk factors and guide the focus of glioma therapy.
Phones don't seem to cause glioma. Unless they do so at a virtually undetectable level. This then opens up the possibility of phones being more beneficial than harmful, when considering the harm they might cause by very rarely causing glioma. How many lives are saved by the ability to immediately call for emergency services, from just about anywhere, compared to the lives lost to glioma. I won't hold my breath.
>In a landmark study carried out by Professor Lai at the University of Washington in the mid 1990s, it was established that RF radiation exposures can cause DNA single strand breaks. Subsequent studies have found single and double-strand DNA breaks.
The findings of this study are true, but they don't necessarily translate into the real world. They experimented upon rats. The strength and doses of radiation in the lab and real world will vary, likely differing significantly. Given that the rates of cancers inculpated by the claimants are stable, these findings are of seemingly no significance to this discussion, and I won't waste my time on them.
5G WiFi:
>A 1992 Russian study found that frequencies in the range 53-78GHz (that which 5G proposes to use) impacted the heart rate variability (an indicator of stress) in rats. Another Russian study on frogs who’s skin was exposed to MMWs found heart rate changes (arrhythmias).
They were using extremely high power levels on rats. This doesn't translate to the real world.
>An experiment conducted by the Medical Research Institute of Kanazawa Medical University found that 60GHz “millimeter-wave antennas can cause thermal injuries of varying types of levels. The thermal effects induced by millimeterwaves can apparently penetrate below the surface of the eye.”
This is a documented effect of powerful microwave radiation. Crowd-control weapons utilizing such technology exist. Some active defense systems also use such technology.
Why do we have water and air pollution? Because the capitalists must dump their waste products somewhere. 5G WiFi and the widespread usage of cellphones are just the result of blindly following the capitalist notion of progress. People smoke due to the stress of living in a capitalist society and even non-smokers have to suffer with them. So, as we can see, capitalism ruins our health in many ways. Note: some of those items listed might also have causes other than the profit motive; namely the numbing of people by fluoride and the addictive substances makes people easier to control and less likely to revolt against oppressive governments. But again, profit is still at least partially involved. This is easy to see when you realize what's offered for sick people - "modern" medicine, whose record is abysmal:
You're not entirely wrong, but you're mixing neutral and/or beneficial things with objectively harmful things like chemical pollution and second-hand smoke. Fluoride reduces the incidence of dental caries and cavities. In a country like America, which has abysmal healthcare systems, especially relating to dentistry, this is undoubtedly beneficial.
You can try to pivot to the issue of universal healthcare, and make me out to be an opponent of socialized medicine for my opposition to the removal of fluoride from water, but this would be misguided. In the current political environment, the political entities interested in removing fluoride from the water are thoroughly uninterested in establishing universal healthcare. By supporting the removal of fluoride from municipal water, motivated by the false idea of fluoride lowering IQ in all contexts, you merely lend your support to these conmens' mission to lower the quality of life for average citizens.
The failure of medicine
Medical Errors: STILL the Third Leading Cause of Death - https://articles.mercola.com/sites/articles/archive/2016/05/18/medical-errors-death.aspx [314]
https://archive.ph/VYh3z [315]
>Dr. Barbara Starfield was the author of that JAMA study, published in 2000, and her research documented how a staggering 225,000 Americans die from iatrogenic causes, meaning their death is caused by a physician's or hospital's activity, manner, or therapy. Her statistics showed that each year:
>12,000 die from unnecessary surgery
>7,000 die from medication errors in hospitals
>20,000 die from other errors in hospitals
>80,000 die from hospital-acquired infections
>106,000 die from the negative side effects of drugs taken as prescribed
>Back then, few people believed it, but in recent days headlines echoing my original 2000 article have made the rounds in many of the major media outlets
>Starfield's findings 16 years ago still stand today. In fact, recent research suggests matters have only gotten worse, and the reason for this is because no affirmative action was ever taken to address and correct the situation.
>According to a new study8 published in the British Medical Journal (BMJ), medical errors now kill an estimated 250,000 Americans each year, an increase of about 25,000 people annually from Starfield's estimates.
>That means medical errors are STILL the third leading cause of death, right after heart disease and cancer. These numbers may actually be vastly underestimated, as deaths occurring at home or in nursing homes are not included.
>As shown by Starfield's research, side effects from drugs, taken as prescribed, account for the vast majority of iatrogenic deaths. Research9 published in 2013 estimated that preventable hospital errors kill 210,000 Americans each year — a figure that is very close to the latest statistics.
>However, when they included deaths related to diagnostic errors, errors of omission, and failure to follow guidelines, the number skyrocketed to 440,000 preventable hospital deaths each year. This too hints at the true enormity of the problem.
>In all, preventable medical mistakes may account for one-sixth of all deaths that occur in the U.S. annually
>According to a report by the Institute of Medicine, an estimated 30 percent of all medical procedures, tests and medications may in fact be unnecessary,15 at a cost of at least $750 billion a year
Credulous acceptance of sensationalist reporting is the norm for this website. The figures proposed by Starfield have been heavily criticized, and only seem to be accepted by know-nothing "journalists" in the mediaf.
I found a rather comprehensive refutation of Starfield's case, which I will present. In essence, Starfield erroneously combined two overlapping categories of death together, leading to double counting of deaths, which inflated the numbers. Other sources Starfield cited relied upon upper estimates of deaths. One source used by Starfield, the IOM report, with its reported 44,000 deaths, was not replicable, and could have been erroneous.
https://skeptics.stackexchange.com/questions/59159/does-allopathy-kill-225-783-thousand-people-in-the-us-per-year [316]
The 225,000 figure
The 225,000 figure comes from a commentary article by Barbara Starfield in the Journal of the American Medical Association titled Is U.S. Health Really the Best in the World? (2000) with a publicly available reprint available via Public Citizen.
Barbara's first supported claim draws from a report published that same year, that estimated the number of deaths attributable to systemic failures in the U.S. healthcare system could be between 44,000 and 98,000 (Barbara Starfield, 2000, pg. 483):
>In addition, with the release of the Institute of Medicine (IOM) report "To Err Is Human,"2 millions of Americans learned, for the first time, that an estimated 44000 to 98000 among them die each year as a result of medical errors.
The IOM has since rebranded as the U.S. National Academy of Medicine (NAM), but its report did make this claim in its executive summary (To Err Is Human, IOM, 2000, pg. 1):
>When extrapolated to the over 33.6 million admissions to U.S. hospitals in 1997, the results of the study in Colorado and Utah imply that at least 44,000 Americans die each year as a result of medical errors.3 The results of the New York Study suggest the number may be as high as 98,000.4
The full title of the "Colorado and Utah" study is the Incidence and Types of Adverse Events and Negligent Care in Utah and Colorado (Eric J. Thomas et al., 2000) and was published in the Journal of Medical Care and authored by a multidisciplinary team of medical professionals, public health researchers and statisticians.
They randomly sampled 15,000 nonpsychiatric discharges from 1992 and reported the amount of adverse events as a percentage of hospital admissions (Eric J. Thomas et al., 2000, abstract):
>Adverse events occurred in 2.9±0.2% (mean±SD) of hospitalizations in each state. In Utah, 32.6±4% of adverse events were due to negligence; in Colorado, 27.4±2.4%. Death occurred in 6.6±1.2% of adverse events and 8.8±2.5% of negligent adverse events.
The IOM report estimated 44,000 deaths based on "33.6 million U.S. hospital admissions in 1997", with 2.9% experiencing adverse events. Using a midpoint negligence rate of 30% (between 32.6% and 27.4%), 70% of events were non-negligent. Of these, 6.6% led to death, yielding 45,017 deaths.
Barbara then inflates this 44,000 figure to create a figure that represents a "combined effect" of illness caused by medical examination or treatment (Barbara Starfield, 2000, pg. 483):
>The health care system also may contribute to poor health through its adverse effects. For example, US estimates8-10 of the combined effect of errors and adverse effects that occur because of iatrogenic damage not associated with recognizable error include:
This "combined effect" figure of 225,000 ultimately draws from five sources, though only three are directly cited (Notes 8–10). The other two rely on unstated assumptions (Barbara Starfield, 2000, pg. 483):
Condition Deaths (approx.) Deaths (actual) Author unnecessary surgery 12,000 11,900 Lucian L. Leape medication errors 7,000 7,391 David P. Phillips et al. other errors 20,000 25,000 Assumed to be a supplement to bridge the gap to the full 44,000. nosocomial infections 80,000 88,000 Assumed to be Robert A. Weinstein nonerror, adverse effects of medications 106,000 106,000 Jason Lazarou et al. 225,000
The 225,000 total seems to subsume a portion of the 44,000 estimate, reclassified as "other errors" and reduced to 39,000, subsequently apportioned between "unnecessary surgery" and "medication errors". Barbara’s suggestion that the final total should be approximately 5,000 higher lends further support to this interpretation. (Barbara Starfield, 2000, pg. 484):
>Third, the estimates of death due to error are lower than those in the IOM report.1 If the higher estimates are used, the deaths due to iatrogenic causes would range from 230000 to 284000.
A problem arises when Barbra adds 80,000 "nosocomial infections" which is unsourced but assumed to be from the CDC’s National Nosocomial Infections Surveillance (NNIS) system and later renamed the National Healthcare Safety Network (NHSN) which reported 88,000 deaths in 1995 (Robert A. Weinstein, 1998, pg. 416):
>It is estimated that in 1995, nosocomial infections cost $4.5 billion and contributed to more than 88,000 deaths—one death every 6 minutes.
The problem being that this now includes a duplication since the "Colorado and Utah" study referenced by the IOM report already included infections for which nosocomial would have been a subcategory (Eric J. Thomas et al., 2000, pg. 266):
>Bleeding was second most common, followed by wound infections, non-wound infections, and deep venous thrombosis.
Finally, the 106,000 "nonerror, adverse effects of medications" deaths came from a meta-analysis published in The Journal of the American Medical Association titled Incidence of Adverse Drug Reactions in Hospitalized Patients (Jason Lazarou et al., 1998, abstract):
>We estimated that in 1994 overall 2216000 (1721000-2711000) hospitalized patients had serious ADRs and 106000 (76000-137000) had fatal ADRs, making these reactions between the fourth and sixth leading cause of death.
Within their methodology, they state they "have chosen the World Health Organization definition for ADR" (Jason Lazarou et al., 1998, pg. 1200) which was defined by the WHO in 1969 as harm within therapeutic doses (WHO, 1969, pg. 6):
>An adverse reaction is defined, for the purposes of this report, one which is noxious and unintended, and which occurs at doses used man for prophylaxis, diagnosis or therapy.
Meanwhile, the "Colorado and Utah" study referenced in the IOM report already accounted for "adverse drug events" (Eric J. Thomas et al., 2000, pg. 261):
>Adverse drug events were the leading cause of nonoperative adverse events (19.3% of all adverse events; 35.1% were negligent, and 9.7% caused permanent disability).
The issue being ADRs are a subset of ADEs, where ADEs encompass harm from both inside and outside of therapeutic contexts as explained in the book Medication Dispensing Errors and Prevention (Rayhan A. Tariq et al., 2024):
>An Adverse drug event is a broader term encompassing any harm resulting from medication, including harm from the drug at a standard dose and harm due to inappropriate dosage or overdose
Moreover, if the 44,000 figure reflects non-negligent adverse events, it brings the ADE definition closer to that of ADR, since events like overdoses, which some doctors might consider negligent, would be excluded.
In summary, the estimate of 225,000 deaths per year is based on a conservative figure of 39,000 from the IOM report (covering infections and non-negligent adverse drug events), to which 80,000 additional nosocomial infections and 106,000 adverse drug reactions are added. This approach produces an invalid total by double-counting overlapping categories.
The 783,936 figure
The 783,936 figure comes from a 2003 self-published article titled Death by Medicine by Gary Null and four others. Just like in Barbara's case, Gary's figure also suffers from incompatible studies being used together (Gary Null, 2003, pg. 1):
Condition Deaths (approx.) Deaths (actual) Author Adverse Drug Reactions 106,000 106,000 Jason Lazarou et al. Medical error 98,000 98,000 IOM Bedsores 115,000 115,000 Gary Null via Cheryl A.Barczak et al. Infection 88,000 88,000 Robert A. Weinstein Malnutrition 108,800 108,800 Gary Null via Sarah G. Burger et al. Outpatients 199,000 198,815 Jeffrey A. Johnson et al. Unnecessary Procedures 37,136 37,136 Gary Null via Eugene G. McCarthy et al. Surgery-Related 32,000 32,591 Chunliu Zhan 783,936
You might have noticed that Gary decided to use the the upper range from the IOM report that used the "New York Study", otherwise known as of Incidence of Adverse Events and Negligence in Hospitalized Patients (Study I, 1991) which was broken down into two parts and published in The New England Journal of Medicine by a multidisciplinary team of nine people.
They randomly sampled 30,121 nonpsychiatric discharges from New York State hospitals in 1984 and reported the amount of adverse events as a percentage of hospital admissions (Study I, Troyen A. Brennan et al., 1991, abstract)
>Adverse events occurred in 3.7 percent of the hospitalizations (95 percent confidence interval, 3.2 to 4.2), and 27.6 percent of the adverse events were due to negligence (95 percent confidence interval, 22.5 to 32.6). Although 70.5 percent of the adverse events gave rise to disability lasting less than six months, 2.6 percent caused permanently disabling injuries and 13.6 percent led to death.
The IOM report seems to have again based the 98,000 estimate on deaths from non-negligent adverse events. This figure was derived from "33.6 million hospital admissions in 1997" by applying a 3.2% lower bound for adverse events, the non-negligent portion (100% - 32.6% = 67.4%), and a 13.6% death rate, resulting in 98,557 deaths.
The second part of the “New York Study,” titled The Nature of Adverse Events in Hospitalized Patients (Study II, 1991) , provides a more detailed analysis of the findings, indicating that “Drug Reactions,” “Infection,” and “Surgery-Related” events were already accounted for (Study II, Lucian L. Leape et al., 1991):
>Drug complications were the most common type of adverse event (19 percent), followed by wound infections (14 percent) and technical complications (13 percent). Nearly half the adverse events (48 percent) were associated with an operation.
Gary clarifies that "Unnecessary Procedures" refers to deaths due "Unnecessary Surgical Procedures" (Garry Null et al., 2003, pg. 11) which is simply a subcategory of all deaths "associated with an operation" (Study II, Lucian L. Leape et al., 1991).
He also clarifies that "Malnutrition" refers to deaths due to "nursing home residents who are malnourished" (Garry Null et al., 2003, pg. 17). In this case, treatment would involve increasing caloric intake and has nothing to do with allopathy, which is generally defined as the use of "drugs or surgery" (Himel Mondal et al., 2022).
The "New York Study" does not explicitly mention "Bedsores", but its methodology of randomly selecting hospital discharges would likely capture cases coded as "Chronic ulcer of skin" (ICD-9-CM, Code 707) in the hospital's medical classification system. This condition could be recorded as a cause of death in discharge documents.
The inclusion of "Outpatients" deaths is from a study titled Drug-related morbidity and mortality and the economic impact of pharmaceutical care (1997) published in the American Journal of Health-System Pharmacy (Jeffrey A. Johnson et al., 1997):
>In the study reported here, we estimated the economic impact of providing pharmaceutical care to ambulatory care patients in the United States.
Fifteen pharmacists contributed to a probability pathway model. The model estimated three paths patients would take if "10% of prescriptions are never filled, leading to treatment failures or new medical problems or both" (Jeffrey A. Johnson et al., 1997). For each path, seven exact branches could be followed, including admission to hospital or long-term care or death.
Ignoring the fact that this is not an empirical study, two other issues arise. First, the death could occur in a hospital, meaning it would be a subcategory of the "New York" study. Secondly, not having your prescriptions filled could be considered negligence and not a result of allopathy, indeed, it might represent the absence of allopathic care.
In summary, using the "New York Study" as the primary reference renders the seven other studies redundant, as they either pertain to non-allopathic care or double-count deaths already accounted for in the primary reference study.
Conclusion
While the 2016 Before It’s News article accurately repeated death estimates from its references, those references were based on flawed methodologies or had nothing to do with allopathic care.
The "New York Study" remains the strongest source for estimating deaths related to allopathic care, as its random sampling of hospital discharges offered the most comprehensive view of hospital deaths.
Since that 1991 "New York Study", a more recent study has been published using data from 2018 (The Safety of Inpatient Health Care, David W. Bates et al., 2023):
>Adverse events during hospitalization are a major cause of patient harm, as documented in the 1991 Harvard Medical Practice Study. Patient safety has changed substantially in the decades since that study was conducted, and a more current assessment of harm during hospitalization is warranted.
After randomly selecting 2,809 admissions from 11 Massachusetts hospitals they ultimately found "There were seven deaths, one of which was deemed to be preventable." (The Safety of Inpatient Health Care, David W. Bates et al., 2023). Marking an incredible improvement since 1984.
In the conclusion of that refutation, they mentioned a recent study which, in the state of Massachusetts, found very few deaths. It can be read in full here.[317]
Here's another study, which also investigated the rate of death from medical errors. It was around 3.1%, and mostly confined to people who were already dying of disease: [318]
>Background
>The number of preventable inpatient deaths in the USA is commonly estimated as between 44,000 and 98,000 deaths annually. Because many inpatient deaths are believed to be preventable, mortality rates are used for quality measures and reimbursement. We aimed to estimate the proportion of inpatient deaths that are preventable.
>Methods
>A systematic literature search of Medline, Embase, Web of Science, and the Cochrane Library through April 8, 2019, was conducted. We included case series of adult patients who died in the hospital and were reviewed by physicians to determine if the death was preventable. Two reviewers independently performed data extraction and study quality assessment. The proportion of preventable deaths from individual studies was pooled using a random-effects model.
>Results
>Sixteen studies met inclusion criteria. Eight studies of consecutive or randomly selected cohorts including 12,503 deaths were pooled. The pooled rate of preventable mortality was 3.1% (95% CI 2.2–4.1%). Two studies also reported rates of preventable mortality limited to patients expected to live longer than 3 months, ranging from 0.5 to 1.0%. In the USA, these estimates correspond to approximately 22,165 preventable deaths annually and 7150 deaths for patients with greater than 3-month life expectancy.
>Discussion
>The number of deaths due to medical error is lower than previously reported and the majority occur in patients with less than 3-month life expectancy. The vast majority of hospital deaths are due to underlying disease. Our results have implications for the use of hospital mortality rates for quality reporting and reimbursement.
...
>Lastly, our study is limited only to preventable mortality and does not include estimates of preventable morbidity, another critical aspect of patient safety. While the rate of preventable mortality in hospitalized patients is lower than is often reported, it still represents what would be the 15th leading cause of death in the USA40 and deserves the continued attention of clinicians, hospital administrators, and policy makers.
>In conclusion, we found that 3.1% of inpatient deaths are judged by physician review to have been preventable. This rate is lower than previous estimates and implies that the vast majority of inpatient deaths are due to underlying disease and not due to variation in quality of care. This has implications for the use of hospital mortality rates for quality reporting and reimbursement.
As mentioned in the comprehensive refutation in the skeptics page on stackexchange, people at the time tried to replicate the 44k death figure in the IOM, but failed: [319]
>Context: The Institute of Medicine (IOM) report on medical errors created an intense public response by stating that between 44,000 and 98,000 hospitalized Americans die each year as a result of preventable medical errors.
>Objective: To determine how well the IOM committee documented its estimates and how valid they were.
>Methods: We reviewed the studies cited in the IOM committee's report and related published articles.
>Results: The two studies cited by the IOM committee substantiate its statement that adverse events occur in 2.9% to 3.7% of hospital admissions. Supporting data for the assertion that about half of these adverse events are preventable are less clear. In fact, the original studies cited did not define preventable adverse events, and the reliability of subjective judgments about preventability was not formally assessed. The committee's estimate of the number of preventable deaths due to medical errors is least substantiated. The methods used to estimate the upper bound of the estimate (98,000 preventable deaths) were highly subjective, and their reliability and reproducibility are unknown, as are the methods used to estimate the lower bound (44,000 deaths).
>Conclusion: Using the published literature, we could not confirm the Institute of Medicine's reported number of deaths due to medical errors. Due to the potential impact of this number on policy, it is unfortunate that the IOM's estimate is not well substantiated.
The rate of death from medical errors may have been higher in the past, but in the current era it seems to be quite low.
I can't claim to know exactly how many deaths are caused by medical errors, but it seems to be lesser than the reported figures reaching into the hundreds of thousands. Those numbers were based upon flawed analyses, which were subsequently circulated through sensationalist reporting.
Fatal medical errors are not common, but some figures suggest them to be the fifteenth leading cause of death. They are a problem which could be addressed through reform of the medical system. Greater accountability for those causing errors, higher standards put upon medical practicioners to ensure that we do not have people causing harm. Generalized standards to be implemented throughout the nation, such that you do not have a massive disparity in patients' quality of care between jurisdictions. These are ideas that I, a layperson, can throw out.
Unfortunately, digdeeper, like a toddler, throws a tantrum and demands humanity to rollback its centuries of progress in medicine instead of seeking out reform.
Note how they report in these studies that often times the majority of these deaths due to medical errors are people who are terminally ill. I cannot know the intentions of these scientists with certainty, but statements such as this can be seen undoubtedly as a tacit minimization of these deaths. "The people were already dying anyway, after all." they may say.
There's a few issues here. And bear in mind, I am speaking of America, as all of these statistics concern America.
For one, just because a person is dying doesn't mean they do not deserve to be cautiously cared for, such that they don't have some dumb-fuck killing them.
But, some may reply that the frail condition of the terminally ill people made them more likely to be killed by error, and this may be true for some, or many cases.
To this we can ask how many of these terminally ill people were made to be terminally ill due to the indignities of our medical system in America. You can learn about plenty of cases of people who had cancer, and did not get access to quality care from their doctors, ultimately dying because of it. I have heard of people who had slow-progressing cancers, who got trapped in a years-long cycle of abominable doctors that did not give them the attention they deserved, and had their cancer become terminal because of it, when it easily could have been dealt with through surgical intervention. People of this sort could be made to be terminally ill, and could die to medical error. They are effectively being killed by the medical system.
>Cholesterol Drugs Are Dangerous And Ineffective, Medical Researchers Say [320]
>By Konstantin Eriksen
>Over the last 10 to 15 years, the drug companies have gotten so greedy that they are not happy with the profits they are making from ill people, they actually want healthy people to take prescription drugs for "preventative" reasons. One of the most prevalent methods that the have used, and one that makes them several billion dollars a year, is to popularize the fable that the general healthy population will have better health outcomes in the future if they take statin drugs to keep their cholesterol levels low today.
The only people I've ever known to take cholesterol-lowering drugs are people with chronically high cholesterol, usually due to genetic conditions. Continuing:
>The Cochrane Library has published a new study on cholesterol-lowering drugs. What this study found is that almost all studies claiming that cholesterol-lowering drugs are safe have been done by the pharmaceutical companies that sell them. The researchers collected data from 14 such drug trials. The drug trials involved over 34,000 patients. The conclusion was that there is no evidence proving that it is safe for healthy people with no history of heart disease to take cholesterol-lowering drugs.
>One of the researchers in the study, Professor Shah Ebrahim from the London school of hygiene and tropical medicine, was quoted as saying that the researchers "found that evidence that potential harm is not being taken seriously. The adverse effects are not included in the trials."
>Furthermore, a study published in the British medical Journal in 2010 concluded that for every heart attack allegedly prevented by cholesterol-lowering drugs, two people suffer liver damage, kidney failure, cataracts or extreme muscle weakness as a direct result of taking the statin drugs. The researchers concluded that statin drugs hurt more people than they help.
>Cholesterol only becomes a problem when there is too much cholesterol going into your blood vessels compared to the amount of cholesterol leaving your blood vessels. This is what the ratio LDL to HDL refers to. If your ratio LDL to HDL is lower than 2 then you should be okay. Even better news is that there is a natural product called concentrated fish oil which actually raises HDL and lowers LDL, thereby improving your ratio with no side effects whatsoever.
I dislike people who do not adequately cite their sources in contexts such as this. Eriksen did not even bother to so much as name the study in question, leaving me to try and find it.
I looked into Shah Ebhrahim and the quote of him. I could not find the quote anywhere.
I found a profile of one Shah Ebhrahim, from the "London School of Hygiene and Tropical Medicine", just like the one mentioned by Eriksen.[321] I skimmed through all 606 of his publications, and did not find anything relating to a Cochrane review as described by Eriksen. It's possible that I missed it, or that researchgate didn't list it. They don't always list all of a scientist's publications.
I did find publications of Shah Ebhrahim in favor of the use of statins for reducing the risk of cholesterol-induced conditions like cardiovascular disease. How interesting that the man being quoted in opposition of statins makes favorable publications of them.
Here is the first example that I stumbled upon. In the text, Ebrahim critiques other scientists questioning the efficacy of statins in women.[322][323]
>Evidence to support the use of statins for preventing recurrent cardiovascular disease (CVD) is strong, derived from individual patient data meta-analysis1 and from systematic reviews of randomized trials.2 This evidence underpins the use of statins in clinical guidelines internationally as an uncontroversial treatment for secondary prevention that is both cost-effective and safe.
It becomes so contradictory in the second example that I literally found myself questioning my reading comprehension as I was reading, beginning to wonder if my interpretation of the author's stance on statins was merely a delusion, and that he was actually against them, but I was failing to realize this. Here is the name of the paper: [324]
Statins for all by the age of 50 years?
It is comical.
In this text, Ebrahim suggests that it could be beneficial to society to broaden the use of statin drugs, in favor of aiding older people. I mean, this is a direct contradiction of the thesis of Eriksen, who believes that fewer people should be using statins.
So, then I looked for the Cochrane study.
A person named Shah Ebrahim is a co-author of a Cochrane review similar to the one mentioned by Eriksen.[325]
>Fiona Taylor 1 , Mark D Huffman, Ana Filipa Macedo, Theresa H M Moore, Margaret Burke, George Davey Smith, Kirsten Ward, Shah Ebrahim
Here's the abstract:
>Background: Reducing high blood cholesterol, a risk factor for cardiovascular disease (CVD) events in people with and without a past history of CVD is an important goal of pharmacotherapy. Statins are the first-choice agents. Previous reviews of the effects of statins have highlighted their benefits in people with CVD. The case for primary prevention was uncertain when the last version of this review was published (2011) and in light of new data an update of this review is required.
>Objectives: To assess the effects, both harms and benefits, of statins in people with no history of CVD.
>Search methods: To avoid duplication of effort, we checked reference lists of previous systematic reviews. The searches conducted in 2007 were updated in January 2012. We searched the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library (2022, Issue 4), MEDLINE OVID (1950 to December Week 4 2011) and EMBASE OVID (1980 to 2012 Week 1).There were no language restrictions.
>Selection criteria: We included randomised controlled trials of statins versus placebo or usual care control with minimum treatment duration of one year and follow-up of six months, in adults with no restrictions on total, low density lipoprotein (LDL) or high density lipoprotein (HDL) cholesterol levels, and where 10% or less had a history of CVD.
>Data collection and analysis: Two review authors independently selected studies for inclusion and extracted data. Outcomes included all-cause mortality, fatal and non-fatal CHD, CVD and stroke events, combined endpoints (fatal and non-fatal CHD, CVD and stroke events), revascularisation, change in total and LDL cholesterol concentrations, adverse events, quality of life and costs. Odds ratios (OR) and risk ratios (RR) were calculated for dichotomous data, and for continuous data, pooled mean differences (MD) (with 95% confidence intervals (CI)) were calculated. We contacted trial authors to obtain missing data.
>Main results: The latest search found four new trials and updated follow-up data on three trials included in the original review. Eighteen randomised control trials (19 trial arms; 56,934 participants) were included. Fourteen trials recruited patients with specific conditions (raised lipids, diabetes, hypertension, microalbuminuria). All-cause mortality was reduced by statins (OR 0.86, 95% CI 0.79 to 0.94); as was combined fatal and non-fatal CVD RR 0.75 (95% CI 0.70 to 0.81), combined fatal and non-fatal CHD events RR 0.73 (95% CI 0.67 to 0.80) and combined fatal and non-fatal stroke (RR 0.78, 95% CI 0.68 to 0.89). Reduction of revascularisation rates (RR 0.62, 95% CI 0.54 to 0.72) was also seen. Total cholesterol and LDL cholesterol were reduced in all trials but there was evidence of heterogeneity of effects. There was no evidence of any serious harm caused by statin prescription. Evidence available to date showed that primary prevention with statins is likely to be cost-effective and may improve patient quality of life. Recent findings from the Cholesterol Treatment Trialists study using individual patient data meta-analysis indicate that these benefits are similar in people at lower (< 1% per year) risk of a major cardiovascular event.
>Authors' conclusions: Reductions in all-cause mortality, major vascular events and revascularisations were found with no excess of adverse events among people without evidence of CVD treated with statins.
The issue though is that this study doesn't match the description given by Eriksen. It drew data from more trials than the 14 trials mentioned by Eriksen, and examined about 20,000 more people than the trials mentioned by Eriksen. It also was published in 2013. The article written by Eriksen was first archived in 2012. Furthermore, the study concluded that the statins were more beneficial than harmful, in contradiction of the stance of Eriksen.
I looked further, and found this article, again co-authored by one Shah Ebrahim.[326]
>Background
>Reducing high blood cholesterol, a risk factor for cardiovascular disease (CVD) events in people with and without a past history of coronary heart disease (CHD) is an important goal of pharmacotherapy. Statins are the first-choice agents. Previous reviews of the effects of statins have highlighted their benefits in people with coronary artery disease. The case for primary prevention, however, is less clear.
>Objectives
>To assess the effects, both harms and benefits, of statins in people with no history of CVD.
>Search methods
>To avoid duplication of effort, we checked reference lists of previous systematic reviews. We searched the Cochrane Central Register of Controlled Trials (Issue 1, 2007), MEDLINE (2001 to March 2007) and EMBASE (2003 to March 2007). There were no language restrictions.
>Selection criteria
>Randomised controlled trials of statins with minimum duration of one year and follow-up of six months, in adults with no restrictions on their total low density lipoprotein (LDL) or high density lipoprotein (HDL) cholesterol levels, and where 10% or less had a history of CVD, were included.
>Data collection and analysis
>Two authors independently selected studies for inclusion and extracted data. Outcomes included all cause mortality, fatal and non-fatal CHD, CVD and stroke events, combined endpoints (fatal and non-fatal CHD, CVD and stroke events), change in blood total cholesterol concentration, revascularisation, adverse events, quality of life and costs. Relative risk (RR) was calculated for dichotomous data, and for continuous data pooled weighted mean differences (with 95% confidence intervals) were calculated.
>Main results
>Fourteen randomised control trials (16 trial arms; 34,272 participants) were included. Eleven trials recruited patients with specific conditions (raised lipids, diabetes, hypertension, microalbuminuria). All-cause mortality was reduced by statins (RR 0.84, 95% CI 0.73 to 0.96) as was combined fatal and non-fatal CVD endpoints (RR 0.70, 95% CI 0.61 to 0.79). Benefits were also seen in the reduction of revascularisation rates (RR 0.66, 95% CI 0.53 to 0.83). Total cholesterol and LDL cholesterol were reduced in all trials but there was evidence of heterogeneity of effects. There was no clear evidence of any significant harm caused by statin prescription or of effects on patient quality of life.
>Authors’ conclusions
>Reductions in all-cause mortality, major vascular events and revascularisations were found with no excess of cancers or muscle pain among people without evidence of cardiovascular disease treated with statins. Other potential adverse events were not reported and some trials included people with cardiovascular disease. Only limited evidence showed that primary prevention with statins may be cost effective and improve patient quality of life. Caution should be taken in prescribing statins for primary prevention among people at low cardiovascular risk.
The article is dated back to 2011, it involved 34,000 people, and drew from 14 trials. This is probably the study that Eriksen mentioned. As you can see, the authors' conclusions are far more measured than those of their 2013 publication, given the fact they did not have data which could suggest statins to be all that beneficial to people at low risk of cardiovascular issues. Continuing:
>Adverse effects of lowering cholesterol with statins
>There has been some concern that low levels of blood cholesterol increase the risk of mortality from causes other than coronary heart disease, including cancer, respiratory disease, liver disease and accidental/violent death. Several studies have now demonstrated that this is mostly, or entirely, due to the fact that people with low cholesterol levels include a disproportionate number whose cholesterol has been reduced by illness - early cancer, respiratory disease, gastrointestinal disease and alcoholism, among others (Iribarren 1997; Jacobs 1997). Thus it appears to be the pre-existing disease which causes both the low cholesterol and raised mortality (Davey Smith 1992).
>The potential adverse effects of statins among people at low risk of CVD are poorly reported and unclear (Jackson 2001) but, among those with pre-existing CVD, the evidence suggests that any possible hazards are far outweighed by the benefits of treatment. Two reviews of 18 and 35 trials respectively found that there were similar rates of serious adverse events with statins as compared to placebo (Kashani 2006; Silva 2006) and a further review of 26 RCTs concluded that there was no effect on risk of cancer with statins (Dale 2006). Other adverse events have been investigated and may be causal, for example rhabdomyolysis - break down of muscles - which can be serious if not detected and treated early (Beers 2003). However, in a systematic review of statins with about 35,000 people and 158,000 person years of observation in both treated and placebo groups, rhabdomyolysis was diagnosed in eight treated and five placebo patients, none with serious illness or death (Law 2003). One RCT of 621 adults found that statins did not adversely affect self reported quality of life, mood, hostility psychological well being or anger expression (Wardle 1996). Small decrements in scores on tests of psychomotor speed and attention were found by Muldoon et al in an RCT of 209 adults, but Muldoon concluded that more research is needed to fully evaluate this (Muldoon 2000). In addition, a systematic review of five statin trials (N = 30,817) found no evidence that statins increased risk of death from non-illness mortality (accidents, violence or suicide) (Muldoon 2001).
>Limitations of the reviews of the effects of statins
>A major limitation of the evidence summaries to date is the emphasis of the use of statins in secondary prevention of CVD without distinguishing between findings in primary prevention trials. More recently, however, a number of systematic reviews have focused their attention of the use of statins in primary prevention but they differ in their interpretation of the evidence to date (Brugts 2009; Ebrahim 1999; Mills 2008; NICE 2006; Thavendiranathan2006; Vrecer, 2003; Ward 2007). This is largely due to the differing inclusion criteria of the reviews and differences in reporting of outcomes. Where the most recent systematic review (Baigent 2005, Brugts 2009; Mills 2008) promote the use of statins in the primary prevention of CVD (the latter team of authors received industry sponsorship), the evidence remains less clear leading other authors to conclude that the assumed benefits of statin therapy in secondary prevention trials should not be extrapolated to primary prevention populations and that current cholesterol treatment guidelines based on this assumption need to be revised (Abramson 2007). Corporate funding of studies is mentioned, but not as an immediate diaqualifier. According to the authors, liver disease may actually not be due to statins but pre-existing illness.
>The funnel plot for all cause mortality showed no sign of publication bias (Figure 3). Only one trial was funded from taxation (Ministery of Health) whilst the authors of nine trials reported having been sponsored either fully or partially by pharmaceutical companies (five by Bristol Myers and Squibb; two by Pfizer).
There's even a plain-language summary of their article:
>Cardiovascular disease (CVD) is ranked as the number one cause of mortality and is a major cause of morbidity world wide. Reducing high blood cholesterol which is a risk factor for CVD events is an important goal of medical treatment. Statins are the first-choice agents. Since the early statin trials were reported, several reviews of the effects of statins have been published highlighting their benefits particularly in people with a past history of CVD. However for people without a past history of CVD (primary prevention), the evidence is less clear. The aim of this systematic review is to assess the effects, both in terms of benefits and harms of statins for the primary prevention of CVD. We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE and EMBASE until 2007. We found 14 randomised control trials with 16 trial arms (34,272 patients) dating from 1994 to 2006. All were randomised control trials comparing statins with usual care or placebo. Duration of treatment was minimum one year and with follow up of a minimum of six months. All cause mortality. coronary heart disease and stroke events were reduced with the use of statins as was the need for revascularisations. Statin treatment reduced blood cholesterol. Taking statins did not increase the risk of adverse effects such as cancer. and few trials reported on costs or quality of life. This current systematic review highlights the shortcomings in the published trials and we recommend that caution should be taken in prescribing statins for primary prevention among people at low cardiovascular risk.
Their opinion that caution should be taken in prescribing statins to those without a history of cardiovascular issue is motivated by the quality of their evidence. The evidence they worked with would not support prescribing statins to those people, as the safety of this could not be adequately determined.
I'm not here to advocate in favor prescribing statins to people without a history of cardiovascular disease. But, we should not forget that their later study in 2013 investigated the risks of prescribing statins to individuals without a history of CVD, and didn't find meaningful risk.
It seems that, because Eriksen did not bother to cite his sources properly, and only mentioned sources in a sort of nebulous manner, he has made it appear as though he has misrepresented and fabricated evidence.
Who is Shah Ebrahim? A scientist who seems to research the safety and effectiveness of drugs like statins and lifestyle changes such as lowering salt intake, and seems to be favorable towards the administration of statins. Eriksen's quote of Ebrahim citing concerns with respect to the safety of statins could not be found by me. I won't say that Eriksen fabricated this quote, but, I can't find it anywhere, and like I said, Ebrahim seems to favor statins.
What did Shah Ebrahim and his partners discover? That statins are not significantly dangerous to people who are prescribed them, and that the benefits of taking them outweigh the risks.
This contradicts Konstantin Eriksen's flagrant characterization of statins as "dangerous pharmaceuticals". Eriksen opposes statins, and favors fish oil capsules for the lowering of cholesterol over statins.
Eriksen says that triglycerides are much more conclusively linked to heart disease, which isn't true. They are linked to it, but not more so than LDL. Fish oils can lower triglycerides, but they don't lower LDL as effectively as statins do. When LDL is a risk for someone, statins will help them more than some fish oil supplement.
I'm becoming tired with constantly venturing off into long tangents where I debunk nonsense, so I will leave this tangent here. Statins seem to be safe, for the most part. That doesn't mean you shouldn't take them without good cause, as prescribed by a medical professional. It doesn't mean there aren't risks either. There are, I've heard of horrific drug interactions between statins and other drugs, leading to fatal rhabdomyolysis. These are documented interactions though, which one will be warned of if they should take statins. Online databases cataloging drug interactions will document these risks. There are also probably inherent risks to statins outside of drug interactions, but these exist with all drugs.
It is ultimately up to digdeeper to provide a convincing case against statins. I'm not staunchly opposed to them, so I don't feel compelled to attack them.
I've become increasingly irritable as my review of digdeeper's site has continued because of his atrocious quality of evidence. He hardly puts any effort into establishing the veracity of his evidence. This disturbs me, as I try to put effort into establishing the veracity of my evidence. In writing that I'll never publish here, for reasons I've already given, I often spend weeks to months trying to determine what may seem to be relatively basic things. It amounts to hundreds, sometimes thousands of pages read, from various sources. Legal documents, books, news articles, videos which have to be watched and parts of them transcribed. While it might seem needless or pedantic to certain people, it is anything but so. It's how you establish the veracity of your beliefs. It's not a simple process, it's very time consuming. This sort of intellectual rigor is lacking on digdeeper's site. When I've spoken to him, he never saw the utility in it, because he figured that if what he feels he knows is true, there's no need to go about building a case supporting his beliefs. We have a fundamental philosophical difference in how we come to believe in things to be true.
"Cholesterol Drugs Are Dangerous And Ineffective, Medical Researchers Say"
I mean what is this but a purely sensationalist, misleading headline. This is what is being used to build a case against MODERN MEDICINE, an incredibly complex practice, involving multiple scientific fields and all which that entails, which saves countless lives annually. It is really egregious.
When it comes to informing others, the burden is not upon the reader to validate/invalidate your claim. The burden is upon you to adequately support your claim, which the reader can study, and if they will, research and formulate their own opinion around. By throwing out vague headlines, you are leaving the reader to essentially research an entire topic, which is usually quite complicated, on their own. You're telling them to "do [their] own research". It's very lazy. It's not at all conducive to convincing argumentation. This is not how you bring people to feel caring passion for a particular issue. You bring people to feel caring passion for a particular issue by making your own case in relation to that issue. In my case, all I've done is do my own research, and come to completely different conclusions, at your behest.
>Sleeping Pills Are Addictive, Unsafe, and Ineffective - https://www.rehabs.com/pro-talk-articles/sleeping-pills-are-addictive-unsafe-and-ineffective/ [327]
This article on the other hand is more measured and reasonable than the prior one.
Sleeping pills might be overprescribed, and they do carry risks. Obviously, they are inferior to genuine, restful sleep.
My issue with the author is that they take a somewhat libertarian approach to personal health, by suggesting people make personal changes in order to improve their sleep.
Stress often induces insomnia. When speaking of stress relating to finances, with respect to one's job security, one's income, one's rent, one's utility bills, in America, the health of one's car, and other things, there is only so much an individual to do to mediate these things. Individuals are being crushed by the systems they inhabit, and are largely powerless to meaningfully alter their health in as much as their health is affected by these systems. If your financial situation is stressing you out, I suppose that you could "just choose" to not worry about it, but how realistic of a prospect is this? I'd say it's extremely unrealistic. And given how unstable the economy is, your hope in reducing your level of personal stress by downsizing, if you even have anything left in your life to downsize, is heavily dictated by luck. You could try to get a simpler job, try to live more simply, like by moving into a cheaper place, but in many places this is not even an option. There's no jobs, or the job market is so volatile that a job you could switch over to might get eliminated in a few months time. There's hardly any housing, particularly affordable housing. The cost of living is rising just about everywhere on earth, which complicates the option of outright abandoning one's home country for greener pastures. And it makes these libertarian suggestions for us to "just" do whatever we can to take personal responsibility for how our capitalist system saps away at our vitality fall flat. There are many things one can do to improve their health by changing their diet and exercising, but there are serious limitations in the context of this insomnia article. You can be physically fit, with a good diet, but trapped in a financially precarious situation, which can drive to you insomnia.
>Chemotherapy Kills more people than it helps - https://www.cureyourowncancer.org/chemo-kills.html [328]
https://web.archive.org/web/20210608170035/https://www.cureyourowncancer.org/chemo-kills.html
>Treating cancer is BIG business in America -- in fact, it's a $200 billion a year business. Yet 98 percent of conventional cancer treatments not only FAIL miserably, but are also almost guaranteed to make cancer patients sicker.
They always seem to approach this from the paradigm of big business, while at the same time almost invariably shilling you some kind of supplement or dietary regimen that you need to pay for. In the context of this website, it's particularly insane, as they're telling you to reject treatment for _cancer_. But, we've already encountered a psycho who thinks garlic will "kill" rabies.
The big business trope is a particularly hollow line of argumentation, because the alternative medicine and wellness industries are also worth billions of dollars.
On a global scale, the wellness industry is worth trillions: [329]
>The global wellness industry was worth $6.32 trillion in 2023, according to a new report from the Global Wellness Institute, a leading industry group. That’s 25% larger than it was in 2019, making it bigger than the sports and pharmaceutical industries.
To continue quoting the article:
>Did you know that 9 out of 10 oncologists would refuse chemotherapy if they had cancer? That's up to 91% -- a huge percentage that clearly shines a light on the truth: chemotherapy kills.
Wow. I believe this, especially when there's absolutely no source to back up the claim.
>Not shocked enough yet? A rigorous review of chemotherapy revealed that it fails for 98% of people. And when chemotherapy was tested against no treatment, no treatment proved the better option. What's more is only two to four percent of cancers respond well to chemotherapy.
Glad I was sitting in my heroin chair before I began to read this article.
>In a German study of women over age 80 with breast cancer, those who received no treatment lived 11 months longer on average than those who received conventional cancer treatments.
>A 14-year study by two oncologists in Australia reported in the film "A Shocking Look at Cancer Studies" that conventional treatment such as chemotherapy for all of our major cancers is totally ineffective -- far below a 10% success rate.
>Chemotherapy is a barbaric and pointless procedure. It attacks and kills not just cancer, but also all the living, healthy cells in the body and completely cripples the body's immune system. While this extreme treatment has been called effective against testicular cancers and lymphocytic leukemia, in many cases it's hard to tell which the supposed "therapy" will kill first -- the cancer or the patient. In fact, it wouldn't be a stretch to say most people, who die from cancer, actually die from cancer TREATMENTS.
>Mammograms do more damage than good (and preventive mastectomies are pointless)The $4 billion-a-year mammogram industry urges women to rely on these x-ray tests to "protect" their health. However, what they don't tell you is mammograms are a highly unnecessary and harmful treatment. In fact, mammograms harm ten women for every one the procedure helps.
>A study by researchers from the Nordic Cochrane Center in Demark reviewed both the benefits and negative effects of seven breast cancer screening programs on 500,000 women.
>For every 2,000 women who received mammograms over a 10-year period, only one would have her life prolonged, but ten would be harmed. This is because mammograms can actually INCREASE a woman's risk of developing breast cancer by as much as 3% a year by irradiating the breast cells and triggering breast cancer.
>Statistics show that there is no proof preventive mastectomy -- removal of the whole breast -- extends the life of breast cancer patients, yet oncologists go right on doing it on a regular basis. Preventative mastectomies are pointless procedures, and many patients are led to believe they have cancer due to false positive cancer screenings. This means they are pressured into having breasts removed for no reason whatsoever. The women undergoing these treatments are scarred for life.
>CT scans, or computed tomographies, are a common testing procedure for most cancer types, but the irony is that this CT scan radiation is highly dangerous and can lead to cancer itself.
Typically you aren't going to get a CAT scan unless you have a serious issue, likely detected by a less intensive imaging test when speaking of cancers.
>The radiation from a CT scan actually has been shown to cause a substantial amount of cancer. A recent report published in the New England Journal of Medicine suggests that the radiation from current CT-scan use (estimated at more than 62 million CT scans per year in the US) may cause as many as 1 in 50 future cases of cancer. This is nothing to be taken lightly. Radiation from medical devices is a huge and under-estimated contribution to the growing incidence of breast and other forms of cancer.
>According to an article in Time Health, other studies prove doctors are performing too many unwarranted CT scans, exposing a countless amount of patients to cancer-causing radiation. Many mammograms are also miscalibrated, so they end up churning out far too much radiation to be safe. If a woman begins getting routine mammograms at age 40, then by age 60 it is almost certain she will have breast cancer.
>It's no wonder so many women end up with this form of cancer - they begin getting frequent screenings starting in middle age at the urging of doctors everywhere. The health and cancer industries know about the connection between CT scan radiation and mammograms and cancer statistics, yet they keep pushing patients to perform these "preventive" procedures. The outrageous truth is frequent mammograms purposely bring repeat business to the corrupt cancer industry by creating cancer tumors over time.
>There is actually a little-known test for breast cancer that exists, and this method yields no false positive or negatives: a saliva test. Researchers from the University of Texas Health Science Center in Houston discovered that women with breast cancer carry different proteins than women with no cancer; this can be tested by a saliva test so simple a dentist could do it.
>Big Pharma lies to convince us that their so-called cancer "cures" workOncologists and Big Pharma use clever tricks to promote their cancer treatments such as using relative numbers to supposedly prove the effectiveness of their cancer treatments. For example, if you or a loved one has breast cancer, doctors will likely recommend the drug Tamoxifen. They'll tell you it reduces the chances of breast cancer recurring by 49%, which sounds fairly impressive.
>However, based on absolute numbers, Tamoxifen reduces the risk of breast cancer returning by 1.6% -- 30 times less than advertised. Relative numbers instead of cold, hard statistics are often used by oncologists because relative numbers can be manipulated in many ways. Any relative statistic that allows the percentages to be spun in a false positive light could be used in these situations.
>Perhaps you have heard through the major media that treating early stage breast cancer creates a 91% cure rate over five years. This statement is absolutely ridiculous -- you could get the same cure rate by doing nothing at all (breast cancer is a very slow growing cancer).
>Drug companies pay oncologists to promote (expensive) ineffective and toxic cancer drugs. Most oncologists don't make their money by treating patients, but by selling cancer drugs. In fact, according to the Journal of the American Medical Association, as much as 75% of the average oncologist's earnings come from selling chemotherapy drugs in his or her office -- and at a substantially marked-up price.
>Pharmaceutical companies not only hire charismatic people to charm doctors, exaggerate drug benefits and underplay side effects, but they also pay oncologists kickbacks to push their drugs. For example, Astra Zeneca, Inc. had to pay $280 million in civil penalties and $63 million in criminal penalties to the federal government after it paid kickbacks to doctors for promoting its prostate cancer drug.
>Many oncologists are criminals and bullies, not doctorsOncologists not only bully patients into taking the destructive route of chemotherapy, toxic drugs and surgery, but they also don't tell their patients the whole truth about the danger of these treatments, other available options, cancer survival statistics, and much more. An innumerable number of cancer patients have suffered needless at the hands of these so-called doctors, who are often really corrupt and immoral human beings that could care less about the healing process of their patients. Many of these shameless oncologists deserve to be arrested and prosecuted immediately for the crimes they commit, yet they keep on sending patients down the same treacherous and painful road that has resulted in too many deaths to keep track of.
>More and more patients are waking up to the truth about cancer treatment and educating themselves on the power of whole food nutrition and supplements -- they are choosing doctors that educate and heal them rather than bully them into surgery and chemotherapy. The staggering documentary Cancer is Curable mentioned earlier interviews doctors who tell you how patients are often pressured by conventional oncologists; sometimes they're even hustled onto the operating table the day after their diagnosis -- without having any of their other choices explained to them.
>What's worse is that no matter how effective a treatment could be, conventional patients are still being killed by the food they are fed in hospitals. All the doctors in Cancer is Curable unanimously explain that sugar is the No. 1 killer for every cancer patient -- and although every medical doctor should know that fact, they still continue to give their patients tootsie rolls and candies in the chemotherapy room.
>Many oncologists are also telling their cancer patients to stop taking antioxidant supplements while they're undergoing treatment. Why? Because they're saying there is a possibility that antioxidants could be lowering the effectiveness of cancer treatments like radiation treatment and chemotherapy.
>In spite of what you might have been told or led to believe, chemo is hardly the exact science that it pretends to be. And yet, on the mere hunch that antioxidants could be protecting the cancer cells that chemotherapy seeks to destroy, oncologists feel justified in telling their patients to forfeit antioxidant supplements.
>There are a ridiculous number of false positives in cancer screeningsAmong 1,087 individuals participating in a cancer screening trial who received a battery of tests for prostate, ovarian, colorectal and lung cancer, 43 % had at least one false positive test result, according to a study published in an issue of Cancer Epidemiology, Biomarkers & Prevention (http://www.newmaterials.com/Customisation/News/Research_&_Development...). That's almost half of the patients who were tested!
This article makes a tsunami of claims, while most of its claims are either unsourced, lead to dead, unarchived webpages, or lead to a static webpage with somebody rambling about something without any basis. But, I did find two sources.
Much of the article's claims come from this page, almost plagiarized, only this article also shills snake oil.
https://web.archive.org/web/20100413194559/http://sirpabs.ilahas.com/cancer_facts.htm [330]
>The forbidden fruit extract that programs cancer cells to "self destruct"...
>The powerful natural "Pac-Man enzyme" that eats cancer cells alive...
>The natural anti-cancer vitamin banned in the U.S., but still available to you...
>The real life miracle of one woman's escape from terminal breast cancer!
>To a small group of terminal cancer patients, the discovery of cesium chloride, a naturally occurring alkaline mineral, was a ray of hope.
>After all, these patients had been told to go home, make out their wills and start arranging for their funerals.
>Then they discovered this remarkable mineral "starves" cancer cells... quells cancer pain in hours... extends survival rates from weeks to years... and costs just $1 a day.
>But guess what? Powerful new cancer cures like this one are being suppressed, even censored today in America—even though they could save countless lives.
>A former drug rep from Eli Lily testified before Congress saying, "Pharmaceutical companies hire former cheerleaders and ex-models to wine and dine doctors, exaggerate drug benefits and underplay side effects."
>Worse, they pay oncologists kickbacks to push their drugs. For example, AstraZeneca, Inc. had to pay $280 million in civil penalties and $63 million in criminal penalties to the federal government because it paid kickbacks to doctors for promoting its prostate cancer drug.
>Michael Cutler, M.D.
The presumed author.
Here is one of the few sources that I did find. It was an article from sciencedaily which concerned positive cancer screenings and their financial burden to individuals: [331]
>False Positive Screening For Cancer Found To Be Frequent And Costly
>Date: December 30, 2004
>Source: American Association For Cancer Research
>PHILADELPHIA -- Cancer screening tests can frequently produce false positive outcomes that may result not only in anxiety but also additional economic costs as well, according to research conducted by scientists at the Henry Ford Health System, Detroit, Mich., and published in the December issue of Cancer Epidemiology, Biomarkers & Prevention.
>Among 1,087 individuals participating in a cancer screening trial who received a battery of tests for prostate, ovarian, colorectal and lung cancer, 43 percent had at least one false positive test result, according to Jennifer Elston Lafata, Ph.D., director of the Center for Health Services Research at the Henry Ford Health System and the lead author on the study.
>"As new cancer screening tests are developed it is important to consider not only their potential clinical benefits, but also their potential for adverse effects," said Lafata, director of the Center for Health Services Research at the Henry Ford Health System. "One such adverse effect is the medical care costs associated with false positive cancer screening test results. Although such costs are often overlooked, we've shown they can be quite substantial."
>Specifically, men who incurred a false positive result for either prostate, lung or colorectal cancer averaged $1,171 in additional medical care expenditures compared to men with all negative screens. More than half, 51 percent, of the men in the study had at least one false positive test.
>For women, 36 percent had false positive screening results. Women with a false positive screen for ovarian, colorectal or lung cancer experienced $1,024 more in follow-up medical care expenses compared to women with all negative results.
>The study was funded by the National Cancer Institute and is part of a larger trial of the effectiveness of screening for prostate, lung, colorectal and ovarian cancers.
>"The results of this smaller study add to the growing body of evidence highlighting the importance of understanding not only the likely benefits of cancer screening, but also how the accuracy of screening tests impacts patients and medical care expenditures, and thus the overall cost-effectiveness of different screening alternatives," Lafata said.
>"Although the clinical evidence for the use of these and many other new screening tests is still being developed, many such screening tests are already widely used in practice thereby resulting in what can be substantial additional medical care costs without known benefits."
A study covering 1,000 people, which occurred two decades ago. It wasn't large enough to make sweeping statements about entire nations, but certainly should have prompted further investigation. Either way, two decades have passed. This is no longer relevant today.
Most of the claims are completely baseless. Brandolini's law ensures that I could spend a few days researching, to ultimately refute these asinine claims. However, at this point, I've realized that this is unnecessary, as there are simpler ways to refute such lies.
They campaign against anything to prevent cancer. Preventative screening, surgery, chemotherapy, any sort of treatment. These are the very things that have driven cancer deaths down over the past decades.
We can prove this by simply looking at how survival rates have historically improved for many cancers, and the mortality rates for people who opted for alternative medicine over conventional cancer treatments.
Let's start with the historic improvements. Across the board, there have been improvements in the survival rates of many cancers, credited to screening and improved treatment.
This report concerns improvements in cancer treatment in America. It pulled data from SEER, which is an American government program that has compiled cancer statistics for decades: [332]
>Data Source
>SEER Program, National Cancer Institute, 1975–2017 with follow-up through 2022.
>Background
>Advances in the ways that cancer is diagnosed and treated have increased the number of people who live for long periods of time after a cancer diagnosis. This report looks at trends in 5-year survival rates for cancer, a common timeframe used by statisticians to measure survival rates. It is important to note that while many people may live without evidence of cancer during and beyond this period, some people may live long-term with their cancer, or experience a recurrence or progression of their cancer.
>Measure
>Five-year relative cancer survival: The proportion of patients surviving cancer 5 years after diagnosis calculated in the absence of other causes of death. The relative survival ratio is defined as the observed survival in the patient group divided by the expected survival of a comparable group from the general population. This ratio represents survivors that are expected if cancer were the only cause of death in the cohort.
>Characterizing changes in cancer survival over time: The JPSurv (Joinpoint Survival Model) software (1,2) has been developed to analyze trends in survival with respect to year of diagnosis. The software finds the location and number of joinpoints (years of diagnosis at which survival trends have changed) that best fit the data. The estimates in this report use annual relative survival data with up to 5 years of follow-up for cancer patients diagnosed at each calendar year from 2000 through 2018. To summarize the trends in each segment between joinpoints, we use the average absolute change in survival (AAC_S). The AAC_S represents the average percentage points difference of cancer survival for people diagnosed in one calendar year compared to the prior year. For example, a 5-year survival increase from 50% to 60% for people diagnosed in 1980 versus 1990, represents a total increase of 10 percentage points in 10 years and an AAC_S of 1 percentage (survival) points for people diagnosed in a year compared to the previous between 1980 and 1990. The AAC_S depends on the follow-up survival time.
Here's another paper that pulled data from SEER: [333]
>Background:
>Improvements in cancer survival are usually assessed by comparing survival in grouped years of diagnosis. To enhance analyses of survival trends, we present the joinpoint survival model webtool (JPSurv) that analyzes survival data by single year of diagnosis and estimates changes in survival trends and year-over-year trend measures.
>Methods:
>We apply JPSurv to relative survival data for individuals diagnosed with female breast cancer, melanoma cancer, non–Hodgkin lymphoma (NHL), and chronic myeloid leukemia (CML) between 1975 and 2015 in the Surveillance, Epidemiology, and End Results Program. We estimate the number and location of joinpoints and the trend measures and provide interpretation.
>Results:
>In general, relative survival has substantially improved at least since the mid-1990s for all cancer sites. The largest improvements in 5-year relative survival were observed for distant-stage melanoma after 2009, which increased by almost 3 survival percentage points for each subsequent year of diagnosis, followed by CML in 1995–2010, and NHL in 1995–2003. The modeling also showed that for patients diagnosed with CML after 1995 (compared with before), there was a greater decrease in the probability of dying of the disease in the 4th and 5th years after diagnosis compared with the initial years since diagnosis.
>Conclusions:
>The greatest increases in trends for distant melanoma, NHL, and CML coincided with the introduction of novel treatments, demonstrating the value of JPSurv for estimating and interpreting cancer survival trends.
And another paper that pulled data from SEER: [334]
>Abstract
>Background: It is often assumed that increases in cancer survival reflect true progress against cancer. This is true when these increases are accompanied by decreased burden of disease: Fewer people being diagnosed or dying from cancer (ie, decreased incidence and mortality). But increased survival can also occur even when incidence is increasing and mortality is unchanged.
>Objective: To use trends in cancer burden-incidence and mortality-to illustrate when changes in survival reflect true progress.
>Methods: Using data from 1975 to 2010 collected by the Surveillance, Epidemiology, and End Results Program (incidence, survival) and the National Center for Health Statistics (mortality), we analyzed US trends in five-year relative survival, age-adjusted incidence, and mortality for selected cancers to identify patterns that do and do not reflect progress.
>Results: Among the nine common cancers examined, survival increased in seven, and changed little or not at all for two. In some cases, increased survival was accompanied by decreased burden of disease, reflecting true progress. For example, from 1975 to 2010, five-year survival for colon cancer patients improved (from 48% to 68%) while cancer burden fell: Fewer cases (incidence decreased from 60 to 41 per 100,000) and fewer deaths (mortality decreased from 28 to 16 per 100,000), a pattern explained by both increased early detection (with removal of cancer precursors) and more effective treatment. In other cases, however, increased survival did not reflect true progress. In melanoma, kidney, and thyroid cancer, five-year survival increased but incidence increased with no change in mortality. This pattern suggests overdiagnosis from increased early detection, an increase in cancer burden.
>Conclusions: Changes in survival must be interpreted in the context of incidence and mortality. Increased survival only represents progress when accompanied by a reduction in incidence, mortality, or ideally both.
For the most part, cancer survival has been improving. This is being credited to advancements in treatment. If treatment didn't work, or outright "killed", this wouldn't be happening.
This study from Poland tracks the increase in the survival rate of pediatric acute lymphoblastic leukemia at a treatment center over the course of 60 years. It went from 1.2% to 90%. Why did this happen if the big pharma treatments are snake oil? [335]
>Abstract.
>Background: A retrospective analysis was performed to investigate the survival outcomes in pediatric acute lymphoblastic leukemia (ALL) based on time period. We hypothesized that improvement has been obtained with the time-dependent therapeutic era and rise in the gross domestic product (GDP) and Human Development Index (HDI).
>Materials and Methods: Data from 710 children who were treated for ALL between 1958 and 2018 at a single pediatric center were analyzed for probability of 5-year overall survival (pOS), event-free survival (pEFS) and relapse risk (pRR). Time periods were defined by the treatment protocols used in seven consecutive therapeutic eras.
>Results: Over the 60-year period analyzed, pOS increased from 1.2% to 90.7%, pEFS from 1.2% to 86.6%, and pRR decreased from 98.8% to 9.9% for patients treated in the past decade. Risk of mortality for patients who received chemotherapy and hematopoietic cell transplant was reduced to 9.9% in the recent era, however, no statistically significant survival difference was found between patients treated with stem cell transplant and those not.
>Conclusion: The therapeutic era, related to improved GDP and HDI, was a statistically significant predictor of increased OS from ALL.
>Over the analyzed 60-year period, a steady improvement in the cure rate was observed in children with ALL admitted to our center. When compared to outcomes obtained in the USA (6, 7, 12, 15), Germany (8, 10, 11) and Scandinavian countries (9), OS results of patients treated at our center were lower by about 15-20% up until 1995, however, although still worse afterward, the difference was no more than 10%. The long-term survival rate increased from 1.2% in the 1960s to 90% in the current era.
Here's a similar study tracking the improvement of childhood cancer: [336]
>Purpose
>To examine population-based improvements in survival and the impact of clinical covariates on outcome among children and adolescents with acute lymphoblastic leukemia (ALL) enrolled onto Children's Oncology Group (COG) clinical trials between 1990 and 2005.
>Patients and Methods
>In total, 21,626 persons age 0 to 22 years were enrolled onto COG ALL clinical trials from 1990 to 2005, representing 55.8% of ALL cases estimated to occur among US persons younger than age 20 years during this period. This period was divided into three eras (1990-1994, 1995-1999, and 2000-2005) that included similar patient numbers to examine changes in 5- and 10-year survival over time and the relationship of those changes in survival to clinical covariates, with additional analyses of cause of death.
>Results
>Five-year survival rates increased from 83.7% in 1990-1994 to 90.4% in 2000-2005 (P < .001). Survival improved significantly in all subgroups (except for infants age ≤ 1 year), including males and females; those age 1 to 9 years, 10+ years, or 15+ years; in whites, blacks, and other races; in Hispanics, non-Hispanics, and patients of unknown ethnicity; in those with B-cell or T-cell immunophenotype; and in those with National Cancer Institute (NCI) standard- or high-risk clinical features. Survival rates for infants changed little, but death following relapse/disease progression decreased and death related to toxicity increased.
>Conclusion
>This study documents ongoing survival improvements for children and adolescents with ALL. Thirty-six percent of deaths occurred among children with NCI standard-risk features emphasizing that efforts to further improve survival must be directed at both high-risk subsets and at those children predicted to have an excellent chance for cure.
Those who opt for alternative medicine instead of conventional treatment have greatly diminished rates of survival: [337]
>There is limited available information on patterns of utilization and efficacy of alternative medicine (AM) for patients with cancer. We identified 281 patients with nonmetastatic breast, prostate, lung, or colorectal cancer who chose AM, administered as sole anticancer treatment among patients who did not receive conventional cancer treatment (CCT), defined as chemotherapy, radiotherapy, surgery, and/or hormone therapy
>Following 2:1 matching (CCT = 560 patients and AM = 280 patients) on Cox proportional hazards regression, AM use was independently associated with greater risk of death compared with CCT overall (hazard ratio [HR] = 2.50, 95% confidence interval [CI] = 1.88 to 3.27) and in subgroups with breast (HR = 5.68, 95% CI = 3.22 to 10.04), lung (HR = 2.17, 95% CI = 1.42 to 3.32), and colorectal cancer (HR = 4.57, 95% CI = 1.66 to 12.61). Although rare, AM utilization for curable cancer without any CCT is associated with greater risk of death.
Going off of a 5 year survival rate, those who went with alternative medicine were about 25% more likely to die overall, as opposed to those who went with conventional treatments.
People who relied on alternative medicine had higher rates of death, and further disease progression.[338]
>Background. The use of complementary and alternative medicine (CAM) has escalated over the past decade, despite the fact that clinical studies validating the efficacy of CAM remain sparse. Clinicians frequently encounter patients who reject standard treatment, but data on outcomes of patients choosing CAM as primary treatment for breast cancer are also lacking.
>Materials and Methods. Breast cancer patients who refused/delayed standard treatments in favor of alternative therapies were identified in a community surgical practice over a 10-year period. A retrospective chart review was performed with telephone interviews when possible. Estimated 10-year survival given recommended treatment was calculated.
>Results. A total of 61 patients was identified; median age was 53. Median follow-up was 54 months. Patients were stratified into 2 subgroups: those who omitted/delayed surgery (SSG, n = 26) and those who were nonadherent to adjuvant therapy recommendations (ASG, n = 35). In the SSG, 96.2% experienced disease progression; 50% died of disease. Mean stage at initial presentation was II; mean stage at re-presentation after primary treatment with alternative therapies was IV. Disease progression occurred in 86.2% of those in the ASG; 20% died of disease. The mean 10-year survival calculated for those omitting surgery was 69.5%; observed survival for this group was 36.4% at a median follow-up of 33 months.
>Conclusions. Alternative therapies used as primary treatment for breast cancer are associated with disease progression and increased risk of recurrence and death. Diminished outcomes are more profound in those delaying/omitting surgery. Reviewing these results with our patients may help bridge the gap between CAM and standard treatments.
The people who had some of the worst outcomes in this study were those who rejected chemotherapy/radiation/endocrine therapy.
>In the ASG [nonadherent to adjuvant therapy], the median tumor size at presentation was 2 cm. The mean calculated 10-year relapse-free survival at initial presentation was 59.2%. Had recommended adjuvant therapy been followed, relapse-free survival would have improved to 74.3%; however, observed relapse-free survival was only 13.8%.
This study also shows a photo of a patient with a tumor. I have never seen something so horrific. They said that at initial presentation her tumor was 2cm. Instead of getting surgery, she opted for dieting and herbal therapies. In the photo they display, it looks like something out of a sci-fi movie. There's this horrific tumor that has engulfed the right side of her upper torso. If you want to undergo some sham cancer treatments, you ought to see what you may suffer as a result.
People who went with complementary (alternative) medicine died at twice the rate of people who went with conventional treatment in this study: [339]
>Key Points
>Question What patient characteristics are associated with use of complementary medicine for cancer and what is the association of complementary medicine with treatment adherence and survival?
>Findings In this cohort study of 1,901,815 patients, use of complementary medicine varied by several factors and was associated with refusal of conventional cancer treatment, and with a 2-fold greater risk of death compared with patients who had no complementary medicine use.
>Meaning Patients who received complementary medicine were more likely to refuse other conventional cancer treatment, and had a higher risk of death than no complementary medicine; however, this survival difference could be mediated by adherence to all recommended conventional cancer therapies.
>Abstract
>Importance There is limited information on the association among complementary medicine (CM), adherence to conventional cancer treatment (CCT), and overall survival of patients with cancer who receive CM compared with those who do not receive CM.
>Objectives To compare overall survival between patients with cancer receiving CCT with or without CM and to compare adherence to treatment and characteristics of patients receiving CCT with or without CM.
>Design, Setting, and Participants This retrospective observational study used data from the National Cancer Database on 1 901 815 patients from 1500 Commission on Cancer–accredited centers across the United States who were diagnosed with nonmetastatic breast, prostate, lung, or colorectal cancer between January 1, 2004, and December 31, 2013. Patients were matched on age, clinical group stage, Charlson-Deyo comorbidity score, insurance type, race/ethnicity, year of diagnosis, and cancer type. Statistical analysis was conducted from November 8, 2017, to April 9, 2018.
>Exposures Use of CM was defined as “Other-Unproven: Cancer treatments administered by nonmedical personnel” in addition to at least 1 CCT modality, defined as surgery, radiotherapy, chemotherapy, and/or hormone therapy.
>Main Outcomes and Measures Overall survival, adherence to treatment, and patient characteristics.
>Results The entire cohort comprised 1 901 815 patients with cancer (258 patients in the CM group and 1 901 557 patients in the control group). In the main analyses following matching, 258 patients (199 women and 59 men; mean age, 56 years [interquartile range, 48-64 years]) were in the CM group, and 1032 patients (798 women and 234 men; mean age, 56 years [interquartile range, 48-64 years]) were in the control group. Patients who chose CM did not have a longer delay to initiation of CCT but had higher refusal rates of surgery (7.0% [18 of 258] vs 0.1% [1 of 1031]; P < .001), chemotherapy (34.1% [88 of 258] vs 3.2% [33 of 1032]; P < .001), radiotherapy (53.0% [106 of 200] vs 2.3% [16 of 711]; P < .001), and hormone therapy (33.7% [87 of 258] vs 2.8% [29 of 1032]; P < .001). Use of CM was associated with poorer 5-year overall survival compared with no CM (82.2% [95% CI, 76.0%-87.0%] vs 86.6% [95% CI, 84.0%-88.9%]; P = .001) and was independently associated with greater risk of death (hazard ratio, 2.08; 95% CI, 1.50-2.90) in a multivariate model that did not include treatment delay or refusal. However, there was no significant association between CM and survival once treatment delay or refusal was included in the model (hazard ratio, 1.39; 95% CI, 0.83-2.33).
>Conclusions and Relevance In this study, patients who received CM were more likely to refuse additional CCT, and had a higher risk of death. The results suggest that mortality risk associated with CM was mediated by the refusal of CCT.
A small study which found those who opted for alternative medicine died at higher rates: [340]
>Background
>Some breast cancer patients opt for alternative treatments in place of conventional treatments. The lack of published data on the outcome of this strategy may contribute to this trend.
>Methods
>A chart review was performed of breast cancer patients who refused or delayed standard surgery, chemotherapy, and/or radiation therapy. Prognosis was calculated for recommended and actual therapy.
>Results
>Thirty-three patients were included in the analysis. Of 11 patients who initially refused surgery, 10 developed disease progression. Of 3 patients who refused adequate nodal sampling, 1 developed nodal recurrence. Of 10 patients who refused local control procedures, 2 developed local recurrences and 2 died of metastatic disease. By refusing chemotherapy, 9 patients increased their estimated 10-year mortality rate from 17% to 25%.
>Conclusions
>Alternative therapies used as primary treatment for breast cancer are associated with increased recurrence and death. Homeopathy instead of surgery resulted in disease progression in most patients. These data may aid patients who are considering alternative therapies.
It's simply a ludicrous claim that chemotherapy or other cancer treatments kill, and it's an extremely dangerous one at that. Rejecting treatment for cancer can easily turn cancer into a death sentence, when it otherwise wouldn't be. Treatment can still cause harm to the patient in the process of killing the cancer, it can still be ineffective, and it can even kill people sometimes, but the alternative is almost certainly dying of cancer by refusing treatment.
>Too high: Side effects hamper many blood pressure medications - https://scopeblog.stanford.edu/2017/10/19/too-high-side-effects-hamper-many-blood-pressure-medications/ [341]
The thesis of this article is that blood pressure medications are very beneficial, and reduce deaths from things like strokes and heart attacks, but their side effects can cause people to cease their usage of them. It's bad that those medications have side effects which lower people's quality of life, but if nothing else will keep someone from dying of hypertension, what can you do? Chemotherapy also has horrific side effects, sometimes lethal, but it can cure people.
>FAIL: Diabetes Medication Isn't Working. So What Does? - http://www.greenmedinfo.com/blog/fail-diabetes-medication-isnt-working-so-what-does [342]
>Written By: Linda Woolven & Ted Snider
>9.3% of Americans and 6.5% of Canadians suffer from diabetes. There is a lot of agreement about the medical treatment. But does the treatment work? At least 5 crucial studies have found that it doesn't
>People with type 2 diabetes are 2-4 times more likely to die from heart disease. But when the authoritative Cochrane group did a systematic review of 20 studies of type 2 diabetics, they found that there was no significant benefit to intensely targeting blood sugar control with drugs for either cardiovascular death or death from any cause. While it did reduce the risk of amputation, retinopathy and nephropathy, it also increased the risk of hypoglycaemia by 30% (Cochrane Database Syst Rev 2011 Jun 15;(6):CD008143).
>The same year, a meta-analysis of 13 controlled studies confirmed that there was no significant benefit of drug treatment for cardiovascular death or death from any cause. While at first it looked like drugs may reduce the risk of nonfatal heart attacks, when only the high quality studies were included, that apparent benefit disappeared; however, what now appeared was a 47% increase in the risk of congestive heart failure. So, diabetes drugs did not reduce the risk of death from heart disease, they increased them. They also doubled the risk of severe hypoglycaemia (BMJ 2011 Jul 26;343:d4169).
>A third systematic review and meta-analysis included 14 studies of type 2 diabetics. Its negative findings went even further. Not only did diabetes meds confer no benefit for fatal or nonfatal heart attack or stroke nor for death from any cause, this study also found insufficient evidence of reduced risk of retinopathy or nephropathy. This study also found a 30% increased risk of severe hypoglycaemia (BMJ 2011;343:d6898).
>And if you're wondering why 3 studies published in 2011 that showed little or no benefit, but significant risk, of using diabetes drugs didn't send tremors through the medical community, it wasn't even news. Three years earlier, the ACCORD study of 10,251 type 2 diabetics who were at high risk of heart attack or stroke found that intensively targeting blood sugar reductions with drugs did not significantly reduce the risk of major cardiovascular events like fatal or nonfatal heart attack or stroke. Shockingly, it did find that diabetes drugs increase the risk of death from any cause by 22% and from cardiovascular disease by 35% (NEJM 2008; 358:2545-2559).
>Researchers at the Mayo Clinic compared the research published in the top journals between 2006 and 2015 to the recommendations made in medical guidelines. They included all the meta-analyses and systematic reviews of randomized trials. What they found was surprising and disturbing. Though most published statements (77%-100%) and guidelines (95%) still "unequivocally endorsed" medical glycemic control, the evidence from the actual research found "no significant impact" of the medical approach. Controlling blood sugar by the medical approach did not significantly improve the risk of complications due to diabetes, including dialysis, kidney transplant, renal death, blindness or neuropathy. As far as the cardiovascular risks associated with diabetes, though there was a 15% improvement in risk of nonfatal heart attack, there was no significant benefit for all-cause mortality, cardiovascular mortality or stroke. The researchers concluded that there is a great "discordance" between the actual evidence based on research and the recommendations made supposedly based on that research (Circ Cardiovasc Qual Outcomes 2016,doi: 10.1161/ CIRCOUTCOMES.116.002901).
Linda and Ted go on to promote various herbs and spices one can take to mediate their diabetes.
Let's see some of the claims they made in relation to studies that they cited.
>High fiber diets work better than the American Diabetic Association diet and as well as drugs (NEJM 2000;342:1392-98).
The study they cited did not support this claim whatsoever.
NEJM 2000;342:1392-98
This was a small study examining 13 people which says nothing of the efficacy of "drugs" [343]
>Background: The effect of increasing the intake of dietary fiber on glycemic control in patients with type 2 diabetes mellitus is controversial.
>Methods: In a randomized, crossover study, we assigned 13 patients with type 2 diabetes mellitus to follow two diets, each for six weeks: a diet containing moderate amounts of fiber (total, 24 g; 8 g of soluble fiber and 16 g of insoluble fiber), as recommended by the American Diabetes Association (ADA), and a high-fiber diet (total, 50 g; 25 g of soluble fiber and 25 g of insoluble fiber), containing foods not fortified with fiber (unfortified foods). Both diets, prepared in a research kitchen, had the same macronutrient and energy content. We compared the effects of the two diets on glycemic control and plasma lipid concentrations.
>Results: Compliance with the diets was excellent. During the sixth week, the high-fiber diet, as compared with the the sixth week of the ADA diet, mean daily preprandial plasma glucose concentrations were 13 mg per deciliter [0.7 mmol per liter] lower (95 percent confidence interval, 1 to 24 mg per deciliter [0.1 to 1.3 mmol per liter]; P=0.04) and mean median difference, daily urinary glucose excretion 1.3 g (0.23; 95 percent confidence interval, 0.03 to 1.83 g; P= 0.008). The high-fiber diet also lowered the area under the curve for 24-hour plasma glucose and insulin concentrations, which were measured every two hours, by 10 percent (P=0.02) and 12 percent (P=0.05), respectively. The high-fiber diet reduced plasma total cholesterol concentrations by 6.7 percent (P=0.02), triglyceride concentrations by 10.2 percent (P=0.02), and very-low-density lipoprotein cholesterol concentrations by 12.5 percent (P=0.01).
>Conclusions: A high intake of dietary fiber, particularly of the soluble type, above the level recommended by the ADA, improves glycemic control, decreases hyperinsulinemia, and lowers plasma lipid concentrations in patients with type 2 diabetes.
Their next claim
>Fiber supplements are also effective (Am J Clin Nutr 1999;70:466-73; J Diab Comp 1998;12:273-78; J Ethnopharmacol 2005;102:202-7; Eur J Clin Nutr 2002;56:830-42; Am J Clin Nutr 1992;56:1061-65; Am J Clin Nutr 1988;48:1413-17; Am J Clin Nutr 1995;61:379-84).
What does "effective" mean? What were they "effective" at doing?
>A meta-analysis of 35 controlled studies of type 2 diabetics found that supplementing psyllium significantly improves fasting glucose and HbA1c, which is the best measure of long term blood sugar and diabetes control (Am J Clin Nutr 2015;doi:10.3945/ajcn.115.106989).
I looked, and the evidence was all mixed. The studies looked at significantly different people. Some people who took fiber as part of a dietary plan. Some people who took medications, and also added fiber to their diet. None of it concerned the supposed superiority of fiber towards "drugs".
Am J Clin Nutr 1999;70:466-73;
Another small scale study examining 34 males, which investigates the effectiveness of psyllium husk fiber in reducing LDL cholesterol and glucose levels. Reported p values weren't great. Study says nothing about effectiveness of "drugs". Page 2 of the full text states that the men were not using medication to treat their diabetes In page five they state that the fiber could be used adjunctively in a diabetes diet plan.[344][345]
>Background: Water-soluble dietary fibers decrease postprandial glucose concentrations and decrease serum cholesterol concentrations. This study examined the effects of administering psyllium to men with type 2 diabetes.
>Objective: The objective was to evaluate the safety and effectiveness of psyllium husk fiber used adjunctively to a traditional diet for diabetes in the treatment of men with type 2 diabetes and mild-to-moderate hypercholesterolemia.
>Design: After a 2-wk dietary stabilization phase, 34 men with type 2 diabetes and mild-to-moderate hypercholesterolemia were randomly assigned to receive 5.1 g psyllium or cellulose placebo twice daily for 8 wk. Serum lipid and glycemic indexes were evaluated biweekly on an outpatient basis and at weeks 0 and 8 in a metabolic ward.
>Results: In the metabolic ward, the psyllium group showed significant improvements in glucose and lipid values compared with the placebo group. Serum total and LDL-cholesterol concentrations were 8.9% (P < 0.05) and 13.0% (P = 0.07) lower, respectively, in the psyllium than in the placebo group. All-day and postlunch postprandial glucose concentrations were 11.0% (P < 0.05) and 19.2% (P < 0.01) lower in the psyllium than in the placebo group. Both products were well tolerated, with no serious adverse events related to treatment reported in either group.
>Conclusion: The addition of psyllium to a traditional diet for persons with diabetes is safe, is well tolerated, and improves glycemic and lipid control in men with type 2 diabetes and hypercholesterolemia.
J Diab Comp 1998;12:273-78;
I couldn't find this one.
J Ethnopharmacol 2005;102:202-7;
In the abstract, the authors explicitly state their intent to study psyllium as an adjunct to diet or drug therapy. Overall, the study is small and doesn't report great p values.[346]
>Psyllium decreased serum glucose and glycosylated hemoglobin significantly in diabetic outpatients
>Psyllium is a bulk-forming laxative and is high in both fiber and mucilage. The beneficial effect of dietary fiber in the management of type II diabetes, has not been totally demonstrated. The purpose of this study was to determine the plasma-lowering effects of 5.1g b.i.d. of psyllium husk fiber, as an adjunct to dietary and drug therapy on lipid and glucose levels, in patients with type II diabetes. Patients were randomly selected from an outpatient clinic of primary care to participate in a double-blind placebo-controlled study in which Plantago ovata Forsk., or placebo was given in combination with their anti-diabetic drugs. Forty-nine subjects were included in the study that were given diet counseling before the study and then followed for 8 weeks in the treatment period. Fasting plasma glucose (FBS) was measured every 2 weeks, and total plasma cholesterol (TC), LDL-cholesterol (LDL-C), HDL-cholesterol (HDL-C), triglyceride (TG), and insulin levels were measured every 4 weeks. Glycosylated hemoglobin (HbA1c) was also measured at the beginning and ending of the study. The test products (psyllium or placebo) were supplied to subjects in identically labeled foil packets containing a 5.1g dose of product, to consume two doses per day, half an hour before breakfast and dinner. Both products were well tolerated, with no serious adverse events related to treatment was reported in either. Better gastric tolerance to metformin was recorded in the psyllium group. FBS, and HbA1c, showed a significant reduction (p<0.05), whereas HDL-C increased significantly (p<0.05) following psyllium treatment. LDL/HDL ratio was significantly decreased (p<0.05). Our results show that 5.1g b.i.d. of psyllium for persons with type II diabetes is safe, well tolerated, and improves glycemic control.
Eur J Clin Nutr 2002;56:830-42;
I may have found ths study, but I don't know for sure.[347] It's from the same journal.
It's a small study examining the effectiveness of Coenzyme Q10 in lowering blood pressure in diabetic people, among other things. COQ was still less effective than drugs designed to lower blood pressure.
>Coenzyme Q10 improves blood pressure and glycaemic control: a controlled trial in subjects with type 2 diabetes
>Objective: Our objective was to assess effects of dietary supplementation with coenzyme Q10 (CoQ) on blood pressure and glycaemic control in subjects with type 2 diabetes, and to consider oxidative stress as a potential mechanism for any effects.
>Subjects and design: Seventy-four subjects with uncomplicated type 2 diabetes and dyslipidaemia were involved in a randomised double blind placebo-controlled 2x2 factorial intervention.
>Setting: The study was performed at the University of Western Australia, Department of Medicine at Royal Perth Hospital, Australia.
>Interventions: Subjects were randomly assigned to receive an oral dose of 100 mg CoQ twice daily (200 mg/day), 200 mg fenofibrate each morning, both or neither for 12 weeks.
>Main outcome measures: We report an analysis and discussion of the effects of CoQ on blood pressure, on long-term glycaemic control measured by glycated haemoglobin (HbA(1c)), and on oxidative stress assessed by measurement of plasma F2-isoprostanes.
>Results: Fenofibrate did not alter blood pressure, HbA(1c), or plasma F2-isoprostanes. There was a 3-fold increase in plasma CoQ concentration (3.4+/-0.3 micro mol/l, P<0.001) as a result of CoQ supplementation. The main effect of CoQ was to significantly decrease systolic (-6.1+/-2.6 mmHg, P=0.021) and diastolic (-2.9+/-1.4 mmHg, P=0.048) blood pressure and HbA(1c) (-0.37+/-0.17%, P=0.032). Plasma F2-isoprostane concentrations were not altered by CoQ (0.14+/-0.15 nmol/l, P=0.345).
>Conclusions: These results show that CoQ supplementation may improve blood pressure and long-term glycaemic control in subjects with type 2 diabetes, but these improvements were not associated with reduced oxidative stress, as assessed by F2-isoprostanes.
Am J Clin Nutr 1992;56:1061-65;
Nothing I found relating to this pertained to diabetes exclusively. I probably couldn't find the actual study.
Am J Clin Nutr 1988;48:1413-17;
I again found nothing pertinent here. Probably out of a failure to find the study.
Am J Clin Nutr 1995;61:379-84
Examined here are people with high cholesterol, not diabetes.[348] It says nothing of diabetes medication. For brevity, I won't quote the study. Perhaps, this is not the study that they cited. If they had been a little more specific with their citations, this wouldn't have happened.
Am J Clin Nutr 2015;doi:10.3945/ajcn.115.106989
A meta analysis which examines people already being treated for diabetes. It concerns psyllium as an adjunctive, not as a treatment in and of itself.[349]
>Psyllium fiber improves glycemic control proportional to loss of glycemic control: a meta-analysis of data in euglycemic subjects, patients at risk of type 2 diabetes mellitus, and patients being treated for type 2 diabetes mellitus
>Background: A number of health benefits are associated with intake of soluble, viscous, gel-forming fibers, including reduced serum cholesterol and the attenuation of postprandial glucose excursions.
>Objective: We assess the effects of psyllium, which is a soluble, gel-forming, nonfermented fiber supplement, on glycemic control in patients who were being treated for type 2 diabetes mellitus (T2DM) and in patients who were at risk of developing T2DM.
>Design: A comprehensive search was performed of available published literature (Scopus scientific database) and clinical records stored by Procter & Gamble with the use of key search terms to identify clinical studies that assessed the glycemic effects of psyllium in nondiabetic, pre-T2DM, and T2DM patients.
>Results: We identified 35 randomized, controlled, clinical studies that spanned 3 decades and 3 continents. These data were assessed in 8 meta-analyses. In patients with T2DM, multiweek studies (psyllium dosed before meals) showed significant improvement in both the fasting blood glucose (FBG) concentration (-37.0 mg/dL; P < 0.001) and glycated hemoglobin (HbA1c) [-0.97% (-10.6 mmol/mol); P = 0.048]. Glycemic effects were proportional to baseline FBG; no significant glucose lowering was observed in euglycemic subjects, a modest improvement was observed in subjects with pre-T2DM, and the greatest improvement was observed in subjects who were being treated for T2DM.
>Conclusions: These data indicate that psyllium would be an effective addition to a lifestyle-intervention program. The degree of psyllium's glycemic benefit was commensurate with the loss of glycemic control. Because the greatest effect was seen in patients who were being treated for T2DM, additional studies are needed to determine how best to incorporate psyllium into existing prevention and treatment algorithms with concomitant hypoglycemic medications.
This is exactly what I expected to see when I dug into their citations. It is always sophistry with these people.
Their studies pertaining to fibers' effects on diabetes say nothing about the effectiveness of conventional diabetes treatment in and of itself, and often in the studies fibers were deployed adjunctively.
They merely investigated possible dietary options which could help better treat diabetes.
>A vegan diet is more effective than the American Dietetic Association diet and as effective as drugs (Diabetes Care 2006;29:1777-83).
Diabetes Care 2006;29:1777-83
Evidently, people in this study were medicated, to varying degrees.[350]
>A low-fat vegan diet improves glycemic control and cardiovascular risk factors in a randomized clinical trial in individuals with type 2 diabetes
>Objective: We sought to investigate whether a low-fat vegan diet improves glycemic control and cardiovascular risk factors in individuals with type 2 diabetes.
>Research design and methods: Individuals with type 2 diabetes (n = 99) were randomly assigned to a low-fat vegan diet (n = 49) or a diet following the American Diabetes Association (ADA) guidelines (n = 50). Participants were evaluated at baseline and 22 weeks.
>Results: Forty-three percent (21 of 49) of the vegan group and 26% (13 of 50) of the ADA group participants reduced diabetes medications. Including all participants, HbA(1c) (A1C) decreased 0.96 percentage points in the vegan group and 0.56 points in the ADA group (P = 0.089). Excluding those who changed medications, A1C fell 1.23 points in the vegan group compared with 0.38 points in the ADA group (P = 0.01). Body weight decreased 6.5 kg in the vegan group and 3.1 kg in the ADA group (P < 0.001). Body weight change correlated with A1C change (r = 0.51, n = 57, P < 0.0001). Among those who did not change lipid-lowering medications, LDL cholesterol fell 21.2% in the vegan group and 10.7% in the ADA group (P = 0.02). After adjustment for baseline values, urinary albumin reductions were greater in the vegan group (15.9 mg/24 h) than in the ADA group (10.9 mg/24 h) (P = 0.013).
>Conclusions: Both a low-fat vegan diet and a diet based on ADA guidelines improved glycemic and lipid control in type 2 diabetic patients. These improvements were greater with a low-fat vegan diet.
It is impossible for this study to make their diet out to be superior to medication, since they were medicated. What a joke this is.
They go on to cite studies relating to chromium, and other minerals. I won't bother quoting from any of these, as they don't compare supplementation of these micronutrients to diabetes medications. They also cite studies that show how certain diets can decrease the chances of developing diabetes, or assist in managing diabetes, among other things. Their studies which covered diets/supplements to assist in managing diabetes often examined people who were medicated, or who did not need medication.
I won't bother going over these because I'm not interested in exploring alternative methods to managing diabetes, I'm interested in the claim of alternative methods being superior to conventional treatments. The evidence they have presented does not remotely demonstrate their solutions as being superior to conventional treatments. Their evidence doesn't even intend to do so. Nothing they cited suggested alternative methods of managing diabetes to be superior to medications. Nothing.
Diabetes can be a complicated disease in that it varies in severity and presentation from person to person. Everybody is different. You can't dish out dietary recommendations universally in the manner that Linda and Ted have, especially when virtually all of the studies they cited in support of dietary methods for managing diabetes did not venture to demonstrate the ineffectiveness of drugs. They examined people not taking medication but instead dieting for diabetes, and people taking medication and bolstering this with some sort of supplement. The people in these studies were not receiving intensive glycemic control whatsoever, or were people that seemed to need it. The findings of those studies may apply to the contexts in which they occurred. Of course, further research of the broader literature is necessary to verify this, as Linda and Ted are very clearly biased.
Nonetheless, certain diets and the consumption of certain herbs, spices, and micronutrients, I'm sure could help diabetes. But the extent to which one relies upon that is dictated by their personal condition. It's very reckless for Linda and Ted to be giving out misinformed advice like this.
Diabetes is a serious medical condition.
People with diabetes are significantly more likely to have a stroke. Cleveland Clinic states the risk of stroke to be 1.5 times higher, and the risk of death from stroke to be almost twice as high. From Cleveland Clinic: [351]
>Adults with diabetes are 1.5 times more likely to have a stroke than people who don’t have diabetes. And they are almost twice as likely to die from heart disease or stroke as people without diabetes.
This review from Cardiovascular Prevention and Pharmacotherapy shows that people with diabetes are around twice as likely to have a stroke.[352]
>Stroke is notably prevalent among patients with diabetes. According to the 2019 Diabetes Fact Sheet published by the Korean Diabetes Association, the incidence of stroke among patients with diabetes in Korea was 254 cases per 10,000 male patients and 258 cases per 10,000 female patients. Cerebrovascular diseases accounted for 8.9% of deaths in this population [1].
>Cohort studies consistently report an elevated stroke risk in diabetes. In a UK study by Mulnier et al. [2], the age-adjusted hazard ratio (HR) for stroke in type 2 diabetes patients was 2.19 (95% confidence interval [CI], 2.09–2.32) over 7 years. Risk factors such as the duration of diabetes, smoking, obesity, atrial fibrillation, and hypertension were identified. Similarly, statistics from Korea’s National Health Insurance indicated a 2.2-fold higher stroke risk in diabetes patients (95% CI, 2.08–2.32) [3]. Type 1 diabetes was also associated with increased stroke risk in retrospective observational study (HR, 1.50; 95% CI, 1.23–1.83) [4].
>A meta-analysis of 64 cohort studies found the HR for diabetes-related stroke to be 2.28 (95% CI, 1.93–2.69) in women and 1.83 (95% CI, 1.60–2.08) in men [5]. The increased risk was particularly pronounced in younger women, likely due to their relatively lower prevalence of other stroke risk factors, highlighting diabetes as a significant independent contributor to stroke occurrence.
>There are differences in risk according to the stroke type. In a cohort observational study in Sweden with a mean follow-up of 7.9 years, HRs for ischemic and hemorrhagic strokes were 3.29 (95% CI, 2.96–3.66) and 2.49 (95% CI, 1.96–3.16), respectively [6].
>A meta-analysis study also demonstrated that prediabetes—defined as fasting plasma glucose of 100 to 125 mg/dL, and/or 2-hour post-load plasma glucose levels of 140 to 199 mg/dL following a 75 g oral glucose tolerance test—was modestly associated with an increased risk of stroke compared to individuals with normoglycemia (HR, 1.20; 95% CI, 1.07–1.35) [7].
This Harvard report states that the in diabetics, the incidence of cardiovascular problems occurs at double the rate of non-diabetics.[353]
Giving people various dietary recommendations, which tend to have very little significance towards the management of diabetes from the position of a diabetic avoiding any sort of treatment, could have deadly outcomes. This is horrible, half-assed advice.
>Common surgeries have high complication rates - https://www.cheatsheet.com/health-fitness/these-common-surgeries-have-the-highest-mortality-rates.html/ [354]
>No one wants to consider complications when they undergo surgery. The odds are in your favor, but some common procedures still involve fatalities. These are the most dangerous surgeries, ranked by their mortality rates. One heart-related procedure has a death rate of 32% (page 10).
>1. Spinal osteomyelitis surgery
>Mortality rate: 6.9%
>Complications: secondary infection
>Antibiotics take care of most spinal infections, so requiring spinal osteomyelitis surgery is unusual. However, when you need it, the complex procedure will remove the spine’s infected disk or disks. Recovery can be quite painful.
As the article itself states, spinal osteomyelitis surgery is performed in the event of severe infections, among other things. These people can die if they do not get surgery. Digdeeper is a thoroughly unserious individual. His criticism of medicine is completely devoid of all seriousness.
People with a life-threatening health crisis may receive surgery which may kill them, while they would have still died had they not received surgery. Yes. We do not live in a perfect world where all surgery is completely safe. You've really struck at some profound contradiction here.
>2. Esophagectomy
>Mortality rate: 6-7%
>Complications: blood loss, pneumonia, and injury to the spleen or the trachea
This is often performed in the case of esophageal cancer, another lethal disease. The operation is not performed frivolously.
How about this, I will simply mention a surgery that does not apply to a strictly life-threatening condition.
>1. Stomach ulcer surgery
>Mortality rate: 6.8%
This is actually not a routine surgery, and usually is done out of necessity, when regular treatments don't work. Ulcers that don't go away could become a serious issue, possibly deadly in the long term.
>5. Gastric bypass
>Mortality rate: <0.5%
That's a fairly low mortality rate. This is also not a routine surgery. It's usually an elective surgery. The individual ultimately is choosing to have it done, and gives informed consent.
The remainder of the surgeries concern life-threatening conditions, and the article itself states at times that with some surgeries patients are very ill at the time of their operation, putting them at greater risk of death. This obviously skews the results.
Digdeeper is not a serious person when it comes to his criticism of medicine. He's grasping at straws, looking for anything he can to discredit medicine. If a person is going to die from a heart problem, and the only thing they can do to stop this is receive a risky heart surgery, there's literally nothing more to be said. You can advocate for research into making the surgeries more sophisticated and safer. If you identify some systemic issue that causes certain groups of people to be more likely to die than others, you can point that out and call for it to be addressed. But, to use the fact that some surgeries carry risks — especially surgeries which seek to address otherwise fatal conditions — as ammunition against modern medicine is utterly ridiculous.
>And again - many, many more. Modern medicine does not cure diseases - seriously, if you search for "diseases cured by medicine" all you get are various infections allegedly wiped out by vaccinations. But no chronic disease, certainly. And the reason for that is it's not profitable. What is, on the other hand? Producing drugs, doing surgery, scaring people into useless and dangerous screenings. In fact, if a medicine causes another disease or there is a complication after surgery it's even better - more profit for the capitalists, since now the sick person has to do more drugs and procedures. The goal is to keep the patient alive - but dependent on the medical system - for as long as possible.
Cancers have been cured with the use of conventional cancer treatments. Cancers are not categorically "cured", in that treatments which eliminate cancers with 100% reliability do not exist, but like I've said many times, nothing can be cured in this manner. Even rabies vaccines have a rate of error, however minute it is. All forms of cancer are highly different from one another, and many of them are inherently difficult to treat, for reasons that you clearly have no interest in understanding, seeing as you've never explored the subject.
Survival rates are gradually increasing with the passage of time. You may insolently demand cures now, just like you childishly demand that we waste hundreds of billions on going to the Moon while people on earth are starving to death, but that's not realistic. There are actual issues with regards to cancer treatment, like the inability of many people to access high-quality cancer treatment, or general incompetence, even malicious incompetence, in the medical system (in America), which causes people to be more likely to die, or outright kills people, but you don't care about this at all. Because with conspiracists, the real issues get sidelined in favor of the fake ones.
An example in this article is how Africans had less access to the COVID vaccines. Digdeeper dismissed the issue out of hand, because he thought the vaccines were snake venom, and didn't believe anyone was dying. He demonized people advocating for the dispersal of vaccines in African countries.
Which reminds me of an anecdote I have. I remember on one of the occasions where I sat in the digdeeper MUC anonymously, someone brought up a headline about a supposed mosquito-distributed malaria vaccine. If I'm not mistaken, this should be the vaccine-system:[355][356]
Essentially, it is a genetically modified version of the malaria parasite that infects humans without becoming pathogenic. By doing this, the human's immune system can combat the infection and develop immunity. It's an interesting concept.
What was digdeeper's response, along with some other morons in the MUC? Immediate denouncement of the proposition, of course. They fearmongered about how it was infecting people's liver, while not realizing that malaria infection begins in the liver, and this is just a modified version of malaria. They speculated about it genetically altering the liver and so forth. They simply did not like the sound of the vaccine. A genetically modified parasite that infects the liver? Well, that simply cannot be a good thing.
These people have been so utterly brain broken by their fearmongering about COVID vaccines as being genetic therapies, that any sort of vaccine technology which explicitly touches upon concepts relating to genetics causes them to start short-circuiting.
They have zero appreciation of just how much harm malaria causes to African peoples.
Every year, malaria kills over half a million people, primarily children in Africa. It routinely steals the futures of countless human beings every year. In the last 25 years over ten million people have died.
It's not just death either, malaria infection in early childhood can stunt the cognitive development of children. This can hamper a child's ability to learn, which can lower their performance in school, and reduce their opportunities in life. The disease is preventing people from reaching their full potential as humans.
Malaria is a scourge. Infection does not reliably provide one with immunity, which ensures that individuals can be infected throughout their life, and become blighted by the disease, before typically recovering. This traps people in a constant cycle of unwellness, which is one of many elements lowering the quality of life of African peoples. There's a personal cost in the sense that a person could be temporarily disabled by disease, and there's a societal toll for this, when a person cannot work, cannot contribute to their community, and needs to be cared for.
To significantly reduce the prevalence of this disease, or outright eradicate it through prophylactic measures of this sort would undoubtedly be extremely beneficial to people in Africa.
This does not however mean that there aren't ulterior motives behind vaccination campaigns of this sort, or that this is a half-hearted effort.
Improved infrastructure in African nations would undoubtedly lower malaria infection. With proper shelter, people could be less likely to be exposed to mosquitoes, and infection rates could drop. But, to improve infrastructure in African nations would necessitate ceasing the exploitation of those nations, by putting a stop to the unequal exchange that deprives them of their natural resources and the wealth that these resources generates.
Capitalists would never consider ending unequal exchange. That would spell the end of their hegemony. They would lose a great deal of their wealth, and all of the people living in developed nations would find themselves paying more for their electronics. We would likely see westerners supposed concern for the plight of Africans challenged when the price of their iPhones rose.
The best that capitalists are going to do is throw a bunch of genetically-modified mosquitoes out into the jungle to infect people with a less potent form of malaria, in the hopes of providing Africans with immunity, without letting these African people build towards a long-lasting solution for themselves.
This is what they've been doing forever. Aid, like medications and specialized foods, are sent to Africa as life support. They ensure that the population is healthy enough to maintain enough organization to facilitate the harvesting of resources, without being able to build towards anything lasting for themselves.
There undoubtedly could be safety concerns with this vaccine system, much like there are with any novel form of medicine. I don't mean to cast mere concerns over the safety of such a vaccine system as foolish. But, this is not just mere concerns over the safety of the vaccine system. This is a person seeing the world "genetically-modified" and immediately discarding the utility of a vaccine which could be beneficial to the population of Africa.
When I gave pushback in the MUC, stating that there would probably be study into its safety, they doubted this, made me out to be a fool, questioned the veracity of studies into the safety of medicines in general, and went as far as to cast the potential vaccine campaign as a plot to further lower the quality of life of Africans, because to them all medicine is evil.
And it evinces the routine miscalculations of conspiracists.
You have a negative thing in the world which is the result of capitalism. You then have a potential response to this negative thing, which may be somewhat helpful, but not necessarily a substantive solution. Does the conspiracist critique it on this basis? No, they instead immediately jump to this being part of an overarching grand conspiracy to kill people, or harm their health, for the secret reason, as per usual.
Often they will simply latch onto a negative thing which is the result of capitalism in a situation where some treatment for this negative thing is not being proposed, and they will make the negative thing out to be more than it is. This cannot simply be something harmful in the world that is caused by capitalism, no, it is deliberate work of the globalists trying to harm everybody for the secret reason.
An easy example of this is Alex Jones' rant about the chemicals in the water turning the friggin' frogs gay.
What happened here? Companies heavily marketed atrazine, an herbicide that is neurotoxic, a probable human carcinogen, and an endocrine disruptor, which could impact not only humans but organisms like frogs, causing ecological destruction.
The companies made great profits off of this herbicide, while spraying the environment with a chemical that was harmful to many organisms in the ecosystem.
As per usual, America, the global hub of capitalism and imperialism, did not ban the usage of atrazine, unlike many other developed nations.
What was Alex Jones' calculus here?
The globalists were deliberately putting a chemical in the water to turn frogs gay, which would probably turn humans gay in turn. Why? Because they want everyone to be gay for the secret reason.
This completely throws us off track from where we need to be. That's not what happened at all. They marketed something they knew was unsafe because they wanted money, and didn't care about the harm caused by their product. They certainly couldn't find any losses in ecological destruction or disease brought about by their product.
Instead of concerning himself with how real issues can be addressed, digdeeper spends most of his time tearing down people trying to treat deadly diseases with evidence-based medicine as a cabal of murderous, greedy, psychopaths, and links to conmen who promote a bunch of snake oil that does genuinely sick people no good at all. These conmen are the real psychopaths. In many cases, they know they are liars, and in the case of dire diseases like cancer are taking advantage of desperate people. It is not uncommon for these people to have been wronged by the medical system, turning towards the conmen as a last hope.
Conspiracists will gladly analyze scientific studies for the sake of diminishing the effectiveness of some form of modern medicine, but when it comes to scientific studies in favor of their placebo treatment, this interest is noticeably absent. It is because these are people without genuine principles. They wield skepticism as a cudgel, and do not adhere to it themselves, although they pretend to be skeptics and free-thinkers. They call genuine skeptics "pseudo-skeptics", but it is they who are the pseudo-skeptics.
It's clear that digdeeper's hatred for modern medicine is driven by its inability to treat all medical problems. The nature of diseases like cancer is unsettling to him. The idea that one can develop a disease to no fault of their own, for which treatments may not always be effective, especially in the sense of curing one for life, is a hard pill to swallow. In response to this, some people turn towards snake oil which has no evidence proving its efficacy in treating cancers. This is not the answer to the problem, it only makes things worse.
The world is brutally cruel. Looking to how people outside of the developed world live will quickly show you this. We should be living in spite of this. We should not allow the cruelty of the world, and our perception of the senselessness in how it strikes us down with disease and general misfortune, to then cause us to turn towards beliefs which provide us with a sense of comfort by giving us the illusion of security in an otherwise bleak world. You should take good care of your health. You should do everything you can do ensure this. But, doing this does not mean that you will never develop conditions like heart disease, or diabetes, or cancer. People who exercise and who eat well can develop these things, cancer in particular. Taking good care of yourself does not mean you may suffer some health crisis which necessitates surgery in order to save your life. It does not mean that you cannot develop a disease for which surgery is necessary to correct it. You can no doubt reduce your chances of developing diseases like cancer, or heart issues, you can lower your chances of suffering from a whole assortment of diseases, but you are not immune. You shouldn't let yourself go thinking this way. This is merely a way of trying to shield yourself from reality.
You're doing whatever you can to exercise control over your health and this control is limited by your genetics, your environment, and chance itself. But that's fine, because it's all you can do.
Don't go letting snake oil salesmen con you with false cures.
>Every so often, you hear news saying that a cancer cure is just around the corner. However, modern medicine has pocketed 100 billion $ from cancer drugs in 2014. Do you think they would just give up all those profits? There is no chance of seeing a cancer cure from those "researchers"; "cancer funds" are pretty much a fraud and the scammers are laughing their way to the bank. Hey, look, they've even said the quiet part out loud - "Is curing patients a sustainable business model?":
What you're doing here is jumping the gun.
In America, capitalists charge people for life-saving medical treatments. Worldwide, scarcity with some treatments exists which can cause people outside of America to have to spend great deals of money treating their cancer, or other serious medical conditions that they may suffer. Others will outright die for lack of access to treatment.
The figures in the article you cited come from America where the healthcare system is designed to extract as much wealth as possible from patients, often patients in desperate need of care. This sort of profit motive is absent in the remainder of the world. In spite of this, we don't have any cancer cures coming out of highly-developed countries that aren't America.
The mere fact that capitalists do seek to profit off of disease in America does not then make the treatments they profit off of phony. Nor does it mean that there could be some dependable, universal cure were these people not in power. The matter is much more complex than that, if you've bothered to examine cancer research.
To turn away from modern medicine will itself play into this profit motive, to a worse extent. You have people rejecting treatment or vaccination against diseases, which causes them to fall ill. Before, during, and after their sickness, they may depend upon supplements. Supplements formulate a multi-billion dollar industry of their own. Supplements in America often are devoid of regulation ensuring their quality and safety. These are being manufactured by the same vicious capitalists you supposedly revile.
In this commercialized pursuit of wellness, people are lured away from the thought of simply seeking out a universal healthcare program, because they're made to think that they as an individual have the power to maintain good health, by controlling their diet, and by exercising, which is not the case. While those are important aspects of maintaining one's health, there's only so much they can achieve on your own. Your ability is highly constrained by your socioeconomic status. In our current global society blighted by late stage capitalism, many people cannot even maintain a strictly healthy diet, as their food is contaminated. Many people don't have the time or energy to exercise.
>Medical companies are really angry at anything that would actually make people healthy, because it would decrease their "pool of treatable patients" and thus kill profits forever (I don't necessarily endorse those treatments; just wanted to show the attitude). Another similar example: Aspirin seen costing pensions $100 billion as lifespans increase.
Nothing you've presented has shown that medical "companies" feel this way. Virtually all of these medical "companies" whose criticism you've shown have been government health agencies. These tend to be the only element of the healthcare system in a country like America that is not driven solely by profit, and can actually embark on humanitarian initiatives.
>What a disgusting headline, first of all. Here we have something that (allegedly) cures cancer and increases lifespan and the first thing the writer worries about is "how much more money we are going to waste on the oldies". In a sane world, the headline would be "Aspirin cures cancer and lengthens lifespan, and that's FUCKING AMAZING!" with none of the "but our precious profits!" crap mentioned even once in the article. But instead we get this:
"What a disgusting headline," Spare me. You don't give a shit about old people.
>The pension costs for men in the U.K. could rise by 0.7% within 20 years if more people begin taking aspirin daily, according to a statement by Risk Management Solutions Inc. this week.
>Employers and governments are grappling with obligations to retirees as low bond yields make it harder to generate returns on funds set aside for the benefits.
>Capitalism ensures that cheap and effective remedies will get shoved aside in favor of expensive and not very effective - or even dangerous - ones. The cheap remedies aren't effective. The effective remedies are
>Now, aspirin is still technically a medical drug, and so still provides profit for the medical companies and still isn't the comprehensive health intervention that's needed. I am certainly not shilling aspirin as some kind of a cure-all; just - again - using it as an example of the attitude of medical companies towards something too cheap or too effective for their liking.
That article was published by Bloomberg, and cited a market economics company called Risk Management Solutions Inc. These aren't medical companies. These are companies which do not add any perceptible value to society, and can generate information which can encourage the wealthy to push for economic changes that lower the quality of life for many people.
>This situation also shows how - after reaching the retirement age - you are supposed to expire as quickly as possible so that you don't suck up too many resources. That's your reward for 40+ years of devotion to working for your nation. It's also the reason for the recent increases in the retirement age of some European countries. Do you now understand why capitalism is so cancerous? It judges everything - even human life - in terms of profits gained or lost. There is nothing sacred in capitalism, and in fact it makes long life and good health become burdens instead of blessings. This is also why all the food, air, water, etc. was made to be so toxic - guaranteeing a steady influx of patients. And so, the junk food and the other health destroying things send people to the medical mill, which grinds them down and makes huge profits on their expense. It all seems like it's been designed that way.
>The final piece of the puzzle is how the alternatives to modern medicine are so hated in the mainstream. Since they are alleged to be cheaper, more effective, and safer - they're going to threaten the profits of modern medicine - so of course they must become targets. Modern medicine has taken over the legal system and the media to protect its monopoly on healing. This is why websites or product labels are prohibited from making health claims that haven't been approved by a government agency (which derives 2/3 of the drug approval money from the drug companies themselves, making it basically a pay-to-get-approved game) unless they deny them later with "This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease". This is also why all the mainstream health websites - when writing about alternative remedies - include disclaimers such as "don't take this without the doctor's approval" or "this doesn't really do anything / isn't a replacement for medicine". And it's also one of the reasons why all other treatments for COVID were buried in favor of the vaccines. It's also why many of the most effective alternative therapies have either been made illegal or have had disinformation campaigns run on them. What the medical mafia hates the most is the idea of the patient taking charge of his own health. They want him inside the medical mill that will abuse him with expensive drugs, screenings and procedures that will squeeze him for millions and eventually bring his demise. Don't get me wrong - "natural medicine" is also an industry and you can find scammers there as well - but at least they don't persecute or kill their opponents. In the end - for true health to be cultivated - it has to become completely divorced from the profit motive.
It's sad to see how digdeeper confuses positive government regulation, which actively prevents companies from marketing snake oil to people, as part of an overarching conspiracy to deprive people of effective treatments. It is the very thing that capitalists hate.
Medical practicioners recommend against the use of alternative medicines because they care for the lives of humans, and don't want people to harm themselves by disusing effective medical treatments.
No evidence digdeeper has presented has built towards a substantive case against modern medicine. Digdeeper has largely taken issue with modern medicine's non-absolute effectiveness in saving lives, and has compounded this with the fact that in countries like America, corporations like HMOs do make great profit off of the pursuit of medical care. The abandonment of modern medicine will not improve survival rates. The only reason why digdeeper has any data to weaponize against modern medicine, like data relating to mortality associated with medical procedures, is because there is a scientific basis behind the development and application of modern medicines. The effectiveness and risks of treatments are tracked. This is hardly the case with snake oil alternative "medicine". It's why there's such profound differences in the quality of evidence between a legitimate medical treatment, and some sham alternative medicine. The truth can be so painful that it may drive people to turn towards unreliable standards for determining the effectiveness of a given treatment. Standards like mere testimony, devoid of any empirical evidence. Testimony given by people who stand to profit off of lying. The conflict of interest goes unnoticed, nonetheless.
He incorrectly perceived "medical companies" as taking issue with aspirin. As I pointed out, it was not a medical company but some market research firm which pointed out how aspirin may be economically harmful by "costing pensions" money. Aspirin as far as I know is still easily accessible, in spite of that article being over a decade old.
Nonetheless, there's an important miscalculation I'd like to point out. Digdeeper feels that "they", the capitalist class presumably, would seek to eliminate aspirin because of there being too many people using up resources. He brings up how the retirement age is slowly increasing in European countries, to support this.
It's not quite the case that the capitalist class seeks mass depopulation, and is clearly a belief motivated by conspiracy theories such as the "Great Reset", which digdeeper spent quite some time pontificating upon in his COVID article.
The capitalist class does not inherently wish for us all to die off, as far as I can tell. They need us to generate wealth for them. Their concern is in there not being enough "resources" being generated by us. There would not be enough economic activity to sustain society in its current form, were the government to allow too many people to rightfully retire. But that's not necessarily because there's "too many" humans. It's because there are too many billionaires hoarding wealth. They've hoarded wealth to such a degree that society will cease to function if too many people go off into retirement. The solution is to redistribute wealth. When you lean into conspiratorial narratives like mass depopulation for the sake of mass depopulation, you distract yourself from that objective.
This has really dragged on quite long now. I think much of what I've said stands for itself. I don't think I can conclude this article without repeating what has been repeated by myself many times now.
I would urge digdeeper to challenge his own beliefs, in the hope that he will spend less of his time obsessing over imaginary conspiracy theories.
It's what I have done, and what motivated me to write all of this.
I hope he will see how flawed some of his conspiratorial beliefs are, and will perhaps have a change of mind, or at least that some of his readers will. I don't expect for this to be an instantaneous process. It's anything but.
It's not easy, it's a fairly long process, but once you do it, you expand your opportunities quite a bit.
{kind=link}
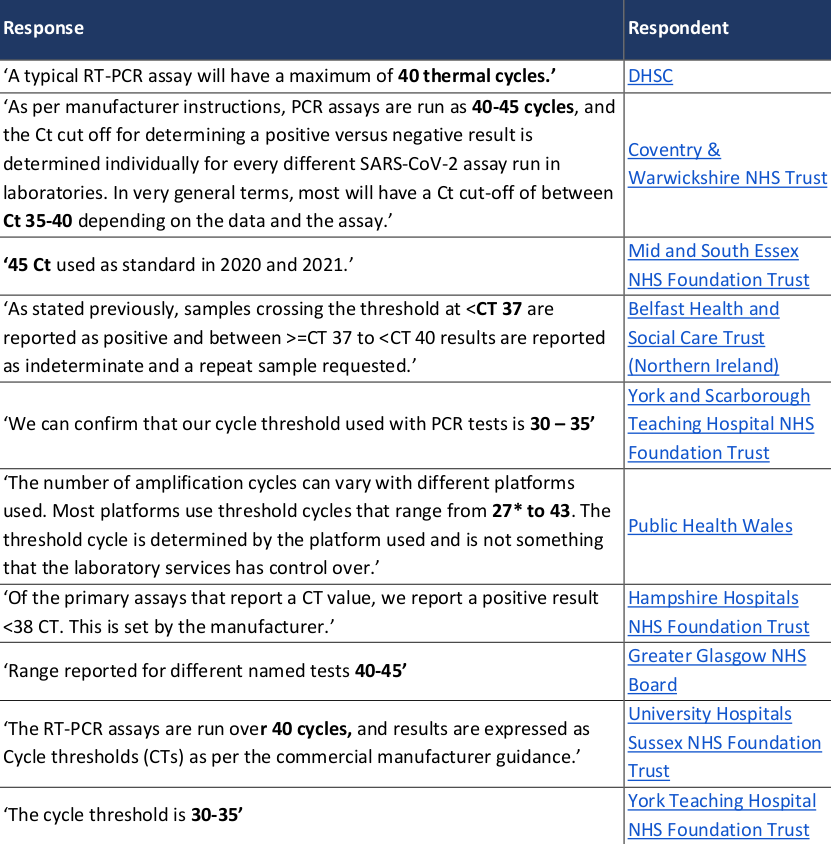{kind=link}
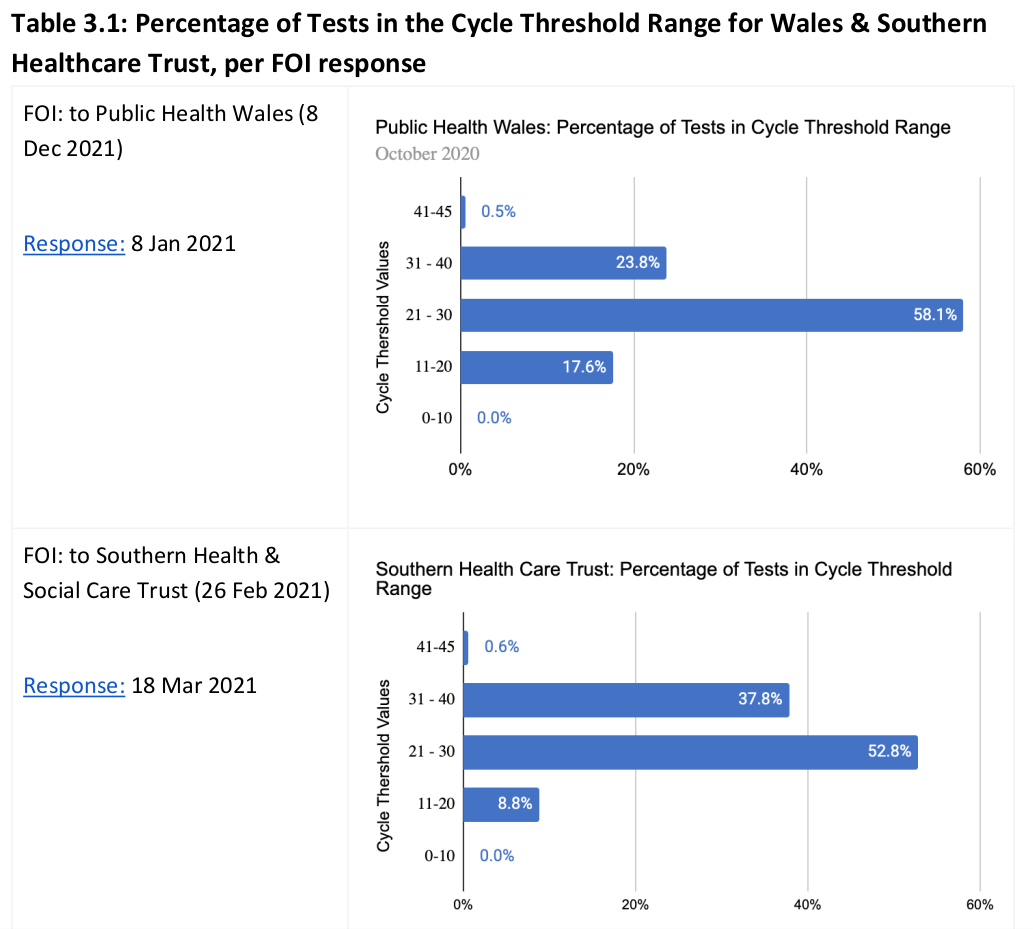{kind=link}
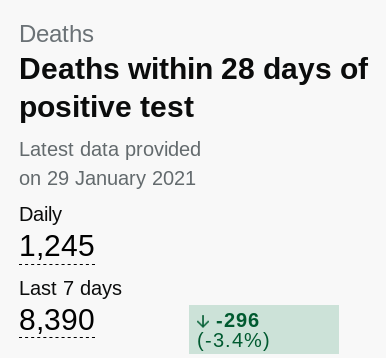{kind=link}
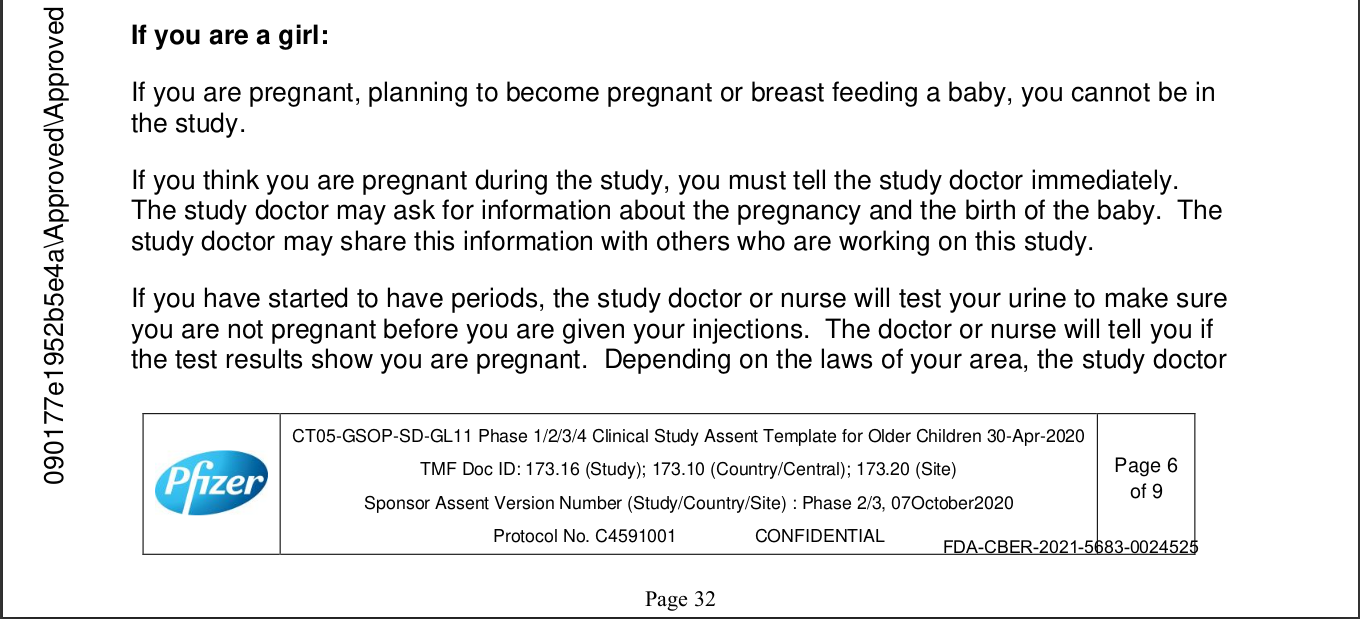{kind=link}
{kind=link}
{kind=link}
{kind=link}